Introducing PERT Pilot, the first iOS app designed for people with exocrine pancreatic insufficiency (EPI / PEI) and the only iOS app for specifically recording pancreatic enzyme replacement therapy (PERT) dosing!
But, that still isn’t the most user-friendly way to enable people to do this.
What else could I do, though? I wasn’t sure.
More recently, though, I have been experimenting with various projects and using ‘large language model’ (LLM) tools like GPT-4 to work on various projects. And a few weeks ago I realized that maybe I could *try* to build an iOS app version of my idea. I wanted something to help people log what they are eating, record their PERT dosing, and more easily see the relationship in what they are eating and what enzymes they are dosing. This would enable them to use that information to more easily adjust what they are dosing for future meals if they’re not (yet) satisfied with their outcomes.
PERT Pilot is designed to help people living with Exocrine Pancreatic Insufficiency (EPI or PEI) more easily deal with pancreatic enzyme replacement therapy (PERT). Aka, “taking enzymes”.
PERT Pilot enables you to log the PERT that you are taking along with a meal, how many pills you take for it, and whether this dosing seems to work for you or not. You can also edit this any time and add any symptoms you may experience after the meal.
Don’t know what your meal is? You can put in a plain language description to the AI meal estimation feature and get back estimates for “a plate of spaghetti” or “two chicken breasts with vegetables” or “two gluten free hot dogs with buns” (or anything else that you eat or drink!).
PERT Pilot then shows you the relationship between how much PERT you have been taking and what you are eating, supporting you as you fine-tune your enzyme intake.
PERT Pilot enables you to share what’s working – and what might not be working – with your healthcare provider. PERT Pilot not only lists every meal you’ve entered, but also has a visual graph so you can see each meal and how much fat and protein from each meal were dosed by one pill – and it’s color coded by the outcome you assigned that meal! Green means you said that meal’s dosing “worked”; orange means you were “unsure”, and red matches the meals you said “didn’t work” for that level of dosing.
You can press on any meal and edit it, and you can swipe to delete a meal.
You can also use the EPI/PEI-SS to track your symptoms over time, recording the frequency and severity, to help you gauge overall progress with EPI symptom management and understanding if your enzyme dosing is working and helping you reduce your symptoms.
Why use PERT Pilot if you have EPI or PEI or PI?
PERT Pilot is the first and only specific app for those of us living with EPI (PEI or PI). People who use the approach in PERT Pilot of adapting their PERT dosing to what they are eating for each meal or snack often report fewer symptoms. PERT Pilot was designed and built by someone with exocrine pancreatic insufficiency, just like you!
With PERT Pilot you can:
Log your meals and PERT dosing. No other app specifically is designed for PERT dosing.
Edit or adjust your meal entry at any time – including if you wake up the next morning and realize your last dose from the day before ‘didn’t work’.
Review your dosing and see all of your meals, dosing, and outcomes – including a visual graph that shows you, for each meal, what one pill ‘covered’ so you can see where there are clusters of dosing that worked and if there are any clear patterns in what didn’t work for you.
You can also export your data if you want to analyze your data elsewhere, or share it with your doctor.
Your data is your data, period. No one has access to your dosing data, symptom data, or outcome data, and nothing you enter into PERT Pilot leaves your device – unless you decide to export your data or share your anonymized EPI/PEI-SS symptom data. No identifying information is ever collected in the app. (See more in the PERT Pilot Privacy Policy.)
Note: this app was not funded by nor has any relationship to any pharmaceutical or medical-related companies. It’s simply built by a person with EPI for other people with EPI.
Here is a quick demonstration of PERT Pilot in action:
You can share your feedback about PERT Pilot:
Feel free to email me (Dana+PERTPilot@OpenAPS.org) any time.
I’d love to hear what works or is helpful, but also if something in the app isn’t yet working as expected.
And, you can share your feature requests! I’m planning to build more features soon (see below).
Look, I get it: you don’t care about a crouton in your salad.
If you don’t like croutons, you simply pick them out of your salad and nudge them to the side of your plate. No harm done.
But for me, a crouton in my salad IS harm done. Even if I were (or the restaurant were) to pick off the croutons, the harm is done. There are specks and crumbs of gluten remaining in my food, and since I have celiac disease, my body is going to overreact to microscopic flecks of gluten and cause damage to my intestines and actively block absorbing the nutrients in the other food that I’m eating.
You might scoff at this concept, but one of the reasons celiac is so risky is because there are both the short term effects (days of abdominal pain, for example) and the long-term risk of causing holes in my intestine and drastically increasing the risk of stomach cancer, if I were to continue consuming gluten.
Some people with celiac aren’t symptomatic, meaning, they could eat the specks (or heck, chunks) of gluten and not feel what I feel.
When I eat specks of gluten? Bad news bears. Literally. It feels like bears clawing at my insides for hours, then days of abdominal soreness, headaches, and feeling unwell. That’s from a SPECK of gluten. I have a strong symptomatic response, so that makes it easier – perhaps – for me than for those with celiac without symptomatic response to choose to be very, very careful and avoiding cross-contamination in my food, and lower my long-term risk of things like stomach cancer that is linked to celiac long-term.
But knowing what I know about how my brain works and the rest of what I’m dealing with, I can imagine the alternative that if I was asymptomatic but lucky enough to discover that I did have celiac disease (through routine screening), I would probably still go to 99% of the same lengths that I do now to avoid gluten and cross-contamination of gluten, because of the long-term risks being so high.
I also don’t have celiac in a silo. I also have type 1 diabetes, which raises my risk of other things…and now I also have exocrine pancreatic insufficiency (EPI) which means every meal I am fighting to supply the right amount of enzymes to successfully digest my food, too. Oh, and now I also have Graves’ disease, so while my thyroid levels are nicely in range and always have been, I’m fighting battles with invisible ghosts in my body (thyroid-related antibodies) that are causing intermittent swelling of my eyelids and messing with my heart rate to tell me that there’s something going on in my body that I have no direct control over.
My plate is already full. (Or my dance card is already full, if you prefer that analogy). I don’t want, and can’t mentally envision right now, handling another thing. I work really hard every day to keep myself in good health. That involves managing my glucose levels and insulin delivery (for Type 1 diabetes), taking my thyroid-related medication that might be helping bring my antibody levels down and monitoring for symptoms to better provided feedback to the 6-week loop of data I get from blood testing to decide how we should be treating my Graves’, to thinking about EVERY SINGLE THING I put in my mouth so that I can take the right amount of enzymes for it, to making sure EVERY SINGLE THING I put in my mouth is gluten-free and is safe from cross-contamination.
Every meal. Every snack. Every drink. Every day.
Probably for the rest of my life: I can’t stop thinking about or doing those things.
Perhaps, then, if you could imagine being in this situation (and I’m so glad most of you are not!), you can imagine that I work really hard to make things easier and better for myself. Both with the plate that I’ve been given, but also in doing my best to lower the risk of more things being added to my already over-loaded plate.
(Preface for this next section: this is about ME not about YOU.)
COVID is one such example. I have worked very hard to avoid COVID, and I am still working very hard to avoid COVID. Like celiac and EPI, if I were to get COVID or other viral illnesses (like the flu), there is the risk of feeling very bad for a short period of time (e.g. 5-7 days). (I’m vaccinated, so the risk of short-term illness being severe (e.g. hospitalization, death) is lowered, and is probably at the same risk as being hospitalized for flu. Even when vaccinated for flu, I’ve been sick enough to almost be hospitalized, which is also why I don’t discount this risk, albeit recognizing it is lower with vaccination).
But like celiac and EPI, if I were to get COVID etc, that increases health risks for the long-term. This is true of most viral illnesses. And when you have an autoimmune condition which indicates your body is a super-star at overreacting to things (which causes other autoimmune conditions), you can imagine that poking the bear is going to make the bear (over)react, whether it is in the short-term or long-term.
It’s not so much if, but when, I would get handed my FIFTH chronic condition if I do get COVID. I went from two (type 1 diabetes and celiac) to four (adding EPI and Graves’) within the course of the same year. This is without having COVID. Given the data showing the increased risk in the long-term of developing many other conditions following COVID, even in people who don’t have superstar overreactive immune systems, it is easy to draw a dotted line to predict the future post-COVID infection to imagine it is not if, but when, my fifth thing would develop and get added to my plate.
So this is why I choose to do things differently than perhaps you do. I mask in indoor spaces. I am currently still choosing to avoid indoor dining. I don’t mind if you choose to do differently; I similarly don’t begrudge you eating croutons. But just like I wouldn’t expect you to pelt me with croutons and yell at me for not eating croutons when you can, I also prefer people not to propel possibly-infectious air at me at short-range when I am unmasked, which is why I prefer to be masked in indoor public spaces. The air is lava (or crouton dust) to me in terms of COVID.
Again, the point here is not to convince you to act any differently than you are acting. You do you! Eat your croutons, do what you like in regard to breathing the air however you like.
But like most folks are 100% fantastic about respecting that I’m not going to eat flecks of croutons, I wish folks would be more understanding of all the background situations behind my (and others’) choices regarding masking or avoiding indoor dining. What I do is not hurting someone else, whether it is not eating croutons or choosing to be masked in an indoor space.
Why would someone want to force me to eat a crouton, knowing it would cause immense harm in the short-term and contribute to long-term damage to my body and increase the risk of life-ending harm?
This is the direction in which I wish we could shift thinking about individual behaviors. Me wearing a mask is like me not eating croutons. Also, I don’t usually ask people to not eat croutons, but many of my friends and family will be happy to agree to eat at a 100% gluten free place if that’s the best option, because it doesn’t harm them not to eat gluten on occasion. Sometimes we do eat at a place that serves gluten, and they eat their croutons without thinking about it. I’m fine with that, too, as long as I am not asked or put at risk of having my mouth be stuffed with crouton dust. That’s how, maybe, I wish people would think about masking. Even if you don’t typically wear masks because you don’t feel you need to, you might choose to occasionally mask indoors when you’re around others who are masking to protect themselves. Like eating at a gluten free restaurant with your friends on occasion, it probably won’t be a big deal for you. You get plenty of gluten at other times. Then you can go back to eating your usual dietary choices (croutons all day, not masking).
COVID is interesting because it is something that potentially impacts all of us, which is why I think maybe the dynamics are changed. Someone might say “oh sure, I wouldn’t throw croutons at you or yell at you for choosing not to eat gluten”. But some people might also think they have the right to judge me regarding my choices around showing up somewhere masked, because they are ‘in the same situation’ and are choosing differently than I.
But my point is: this is not the same situation, the risks to me are not the same, which is why I may choose differently.
TLDR – I guess the point is, what looks like the ‘same’ situation on the outside is not the same for everyone; these differences influence our individual choices and needs; and I wish this is the way more people saw things.
I’ve been training for a big goal of mine: running a 100k in a specific amount of time. Yes, I’ve run farther than that before: last year I ran ~82 miles. However, I had someone in my family network who ran 100k last year, and I realized their time made a reasonable goal for me. I’m competitive, so the extra motivation of striving for a certain time is helpful for channeling my “racing”, even if I’m “racing” someone virtually (who ran a year ago!).
Like last year, I decided I would run my 100k (which is 62+ miles) as a solo or DIY ultramarathon. I originally plotted five laps of various lengths, then figured out I could slightly alter my longest route by almost a mile, making it so I would do 2 laps of the same length, a third lap of my original longest length, and then a fourth lap of a shorter length that’s also one of my preferred running routes. Only four laps would be mentally easier than doing five laps, even though it would end up being exactly the same distance. Like last year, I leveraged extensive planning (most of it done last year) to plan my electrolytes, enzymes, and fueling in advance. I had a lot less work to do this year, because I simply refreshed the list of gear and prep work from last year, shortened of course to match the length of my expected race (less than 18 hours vs ~24+ hours). The main thing I changed in terms of preparation is that while I set out a few “just in case” supplies, most of them I left in their places, figuring they’d be easy enough to find in the house by Scott (my husband) if I needed to ask him to bring out anything in particular. The few things I laid out were emergency medical supplies like inhaled insulin, inhaled glucagon, a backup pump site, etc. And my usual piles of supplies – clothes, fuel to refill my vest, etc – for each lap.
One thing that was different for my 100k was my training. Last year, I was coming back from a broken toe and focused on rebuilding my feet. I found that I needed to stick with three runs per week. This year, I was back up to 4-5 runs per week and building up my long runs beginning in January, but in early February I felt like my left shin was getting niggle-y and I backed down to 3 runs a week. Plus, I was also more active on the weekends, including most weekends where we were cross-country skiing twice, often covering 10-15 miles between two days of skiing, so I was getting 3+ extra hours of “time on legs”, albeit differently than running. Instead of just keeping one longer run, a medium run, and two shorter runs (my original plan), I shifted to one long run, one medium long run (originally 8 and then jumping to 13 miles because it matched my favorite route), and the big difference was making my third run about 8 miles, too. This meant that I carried my vest and fueled for all three runs, rather than just one or two runs per week. I think the extra time training with the weight of my vest paid off, and the miles I didn’t do or the days I didn’t run didn’t seem to make a difference in regard to recovering during the weeks of training or for the big run itself. Plus, I practiced fueling every week for every run.
I also tapered differently. Once I switched to three runs a week, my shin felt a lot better. However, in addition to cross country skiing, Scott and I also have access now to an outdoor rock climbing wall (so fun!) and have been doing that. It’s a different type of workout and also helps with full body and upper body strength, while being fun and not feeling like a workout. I bring it up mostly because three weeks ago, I think I hurt the inside of my hip socket somehow by pressing off a foothold at a weird angle, and my hip started to be painful. It was mostly ok running, but I backed off my running schedule and did fewer miles for a week. The following week I was supposed to do my last longest long run – but I felt like it wouldn’t be ideal to do with my hip still feeling intermittently sore. Sometimes it felt uncomfortable running, other times it didn’t, but it didn’t feel fully back to normal. I decided to skip the last long run and stick with a week of my medium run length (I did 13, 13, and 8). That felt mostly good, and it occurred to me that two shorter weeks in a row were essentially a taper. If I didn’t feel like one more super long run (originally somewhere just under a 50k) was necessary to prepare, then I might as well consider moving my ‘race’ up. This is a big benefit of DIY’ing it, being able to adjust to injury or schedule – or the weather! The weather was also forecasted to be REALLY nice – no rain, high 50s F, and so I tentatively aimed to do a few short runs the following week with my 100k on the best weather day of the weekend. Or if the weather didn’t work out, I could push it out another week and stick with my original plan.
My taper continued to evolve, with me running 4 easy miles on Monday (without my vest) to see how my hip felt. Mostly better, but it still occasionally niggled when walking or running, which made me nervous. I discussed this endlessly with Scott, who as usual thought I was overcomplicating it and that I didn’t need to run more that week before my 100k. I didn’t like the idea of running Monday, then not running again until (Friday-Sunday, whenever it ended up being), but a friend unexpectedly was in town and free on Wednesday morning, so I went for a walk outside with her and that made it easy to choose not to run! It was going to be what it was going to be, and my hip would either let me run 100k or it would let me know to make it a regular long run day and I could stop at any time.
So – my training wasn’t ideal (shifting down to 3 runs a week) and my taper was very unexpected and evolved differently than it usually does, but listening to my body avoided major injury and I woke up feeling excited and with a good weather forecast for Friday morning, so I set off at 6am for my 100k.
(Why 6am start, if I was DIYing? My goal was to finish by 11:45pm, to beat the goal time of 11:46pm, which would have been 17 hours and 46 minutes. I could start later but that would involve more hours of running at night and keeping Scott awake longer, so I traded for an hour of running before it got light and finishing around midnight for a closer to normal bedtime for us both.)
*One other major thing I did to prep was that as soon as I identified that I wanted to shift my race up a week, I went in and started scheduling my bedtimes, beginning with the night before the race. If I raced at 6 from home, I would wake up at 5 to get ready, so I wanted to be sleeping by 9pm at the latest in order to get close to a normal night of sleep. Ideally it would be closer to 8-8:30. I set my bed time and each night prior, marked the bedtime 15 minutes later, so that when I started I was trying to push my bedtime from ~11pm to 10:45 pm then the next night 10:30pm etc. It wasn’t always super precise – I’ve done a better job achieving the goal bedtimes previously, but given that I did an early morning cross country ski race on the morning of daylight saving time the week before (ouch), it went pretty ok, and I woke up at 5am on race morning feeling rested and better than I usually do on race days. 7 hours and 45 minutes of sleep is an hour to an hour and a half less than usual, but it’s a LOT better than the 4-5 hours of sleep I might have otherwise gotten without shifting my schedule.
THE START (MILES 0-17)
I set out at 6am, It was 33 degrees (F), so I wore shorts and a short sleeve shirt, with a pair of fleece lined pants over my shorts and a long sleeve shirt, rain jacket, ear cover, and gloves on my hand. It was dry, which helped. I was the only one out on the trail in the dark, and I had a really bright waist lamp and was running on a paved trail, so I didn’t have issues seeing or running. I felt a bit chilly but within 3 minutes could tell I would be fine temperature wise. As I got on the trail, I glanced up and grinned – the stars were out! That meant I could “check” something off my experience list at the very start. (I make a list of positive and less great experiences to ‘check off’ mentally, everything from seeing the stars or seeing bunnies or other wildlife to things like blisters, chafing, or being cold or tired or having out of whack glucose levels – to help me process and “check them off” my list and move on after problem solving, rather than dwelling on them and getting myself into a negative mood). The other thing I chuckled about at the start was passing the point where, about a half mile in to my 82 miles, I had popped the bite valve off of my hydration hose and gotten water everywhere and couldn’t find the bite valve for 3 minutes. That didn’t happen this time, phew! So this run was already off to a great start, just by nothing wild like that happening within the first few minutes. I peeled off my ear cover at 0.75 miles and my gloves at a mile. My jacket then peeled off to tie around my waist by the second mile, and I was surprised when my alarm went off at 6:30am reminding me to take in my first fuel. My plan calls for fuel every 30 minutes, which is why I like starting at the top of the hour (e.g. 6:00am) so I can use the alarm function on my phone to have alarms pre-set for the clock times when I need to fuel. As I continued my run/walk, just like I do in all my training runs, I pulled my enzymes out of my left pocket, swallowed them, put them away, grabbed my fuel out of my right pocket (starting with chili cheese Fritos), then also entered it into my fuel tracking spreadsheet so I could keep an eye on rolling calorie and sodium consumption throughout my run. (Plus, Scott can also see it and keep an eye on it as an extra data point that I’m doing well and following all planned activities, as well as having live GPS tracking and glucose tracking capabilities). I carried on, and as the sky began to lighten, I could see frost covering the ground beside the trail – brrr! It actually felt a little bit colder as the sun rose, and I could see wafts of fog rolling along the river. I started to see more people out for early morning runs, and I checked my usual irritation at people who were likely only out for (3? 5? 10? Psh!) short morning runs while I was just beginning an all day slog.
I was running well and a little ahead of my expected pace, closer to my usual long run/walk paces (which have been around 14:30-14:50 min/mi lately). I was concerned it was too fast and I would burn out as so many people do, but I did have wiggle room in my paces and had planned for an eventual slow down regardless. I made it to the first turnaround, used the trail bathroom there, and continued on, noting that even with the bathroom stop factored in, I was still on or ahead of schedule. I texted Scott to let him know to check my paces earlier than he might otherwise, and also stopped in my tracks to take a picture of a quail-like bird (which Scott thinks was a pheasant) that I’d never seen before. Lap 1 continued well, and I was feeling good and maintaining an overall sub-15 pace while I had been planning for a 15:10/ish average pace, so although Scott told me he didn’t need me to warn him about being particular miles away for aid station stops, I saw he was still at home by the time I was less than a mile out, and texted him. He was finishing a work call and had to rush to finish packing and come meet me. It wouldn’t have been a big deal if he had “missed” me at the expected turnaround spot, because there’s other benches and places where we could have met after that, but I think he was still stressed out (sorry!) about it, although I wasn’t. However, he biked up to me right at the turnaround spot, grabbed my vest and headed back to our normal table for refueling, while I used the bathroom and then headed out to meet him.
The other thing that might have stressed him out a little – and did stress me out a little bit – was my glucose levels. They were running normal levels for me during a run, around ~150mg/dL in the first 2-3 hours of my run. This is higher than I normally like to be for non-running times but is reasonable for long runs. I usually run a bit higher at the start and then settle in around 120-130mg/dL, because the risk of having too much insulin at the start from breakfast is prone to causing lows in the first hour; therefore I let myself reduce insulin prior to the run so that the first hour or so runs higher. However, instead of coming down as usual from the start of my run, I started a steady rise from 150 to 180. That was weird, but maybe it was a physiological response to the stress? I issued a correction, but I kept rising. I crossed 200 when I should have been beginning to flatten, and it kept going. What on earth? I idly passed my hand over my abdomen to check my pump site, and couldn’t feel my pump site. It had come unclipped!!! This was super frustrating, because it means I didn’t know how much insulin was in my body or when it had come unclipped. (Noteworthy that in 20+ years of using an insulin pump, this has NEVER happened before until this month, and it has now happened twice, so I need to record the batch/lot numbers and report it – this batch of sites is easily coming unclipped with a tug on the tubing, which is clearly dangerous because you can’t feel it come unclipped and don’t know until you see rising glucose levels.) “Luckily” though, this was when I was within 30 minutes or so of being back to Scott, so I texted him and told him to grab the inhaled insulin baggie I had set out, and I would use that at the aid station to more quickly get my body back into a good state (both in terms of feeling the insulin action as well as normalizing glucose levels more quickly. For those who don’t know, injected/pump insulin takes ~45 minutes to peak activity in the body, whereas inhaled insulin is much faster in the ballpark of ~15-20 minutes peak action, so in situations like this I prefer to, when possible, use inhaled insulin to normalize how my body is feeling while also resuming/fixing the pump site for normal insulin from then on).
As planned, at every aid station stop he brought water and ice to refill my camelback, which he did while I was at the bathroom. When I came up to the table where he was, I quickly did some inhaled insulin. Then I sat down and took off my socks and shoes and inspected my feet. My right foot felt like it had been rubbing on the outside slightly, so I added a piece of kinesiology tape to the outer edge of my foot. I already had pieces on the bottom of my feet to help prevent blisters like I got during my 82, and those seemed to be working, and it was quick and easy to add a straight piece of tape, re-stick pieces of lamb’s wool next to each big toe (to prevent blisters there), put fresh socks on, and put a fresh pair of shoes on. I also changed my shirts. It was now 44 F and it was supposed to warm up to 61 F by the end of this next lap. I stood up to put my pack on again and realized I had forgotten to peel off my pants! Argh. I had to unlace my shoes again, which was the most annoying part of my stop. I peeled off the pants (still wearing my shorts under), put my shoes back on and laced them again, then put my vest back on. I removed the remaining trash from my vest pockets, pulled out the old enzyme and electrolyte baggies, and began to put the new fuel supply and enzyme and electrolyte supply in the front vest pockets. Last time for my 82, I had Scott do the refilling of my vest, but this time I just had him set out my gallon bag that contained all of these, so that I could place the snacks how I like best and also have an idea of what I had for that lap. I would need to double check that I had enzymes and electrolytes, anyway, so it ended up being easier for me to do this and I think I’ll keep doing this moving forward. Oh, and at each aid station stop we popped my (non-ultra) Apple Watch on a watch charger to top off the charge, too. I also swapped in a new mini battery to my pack to help keep my phone battery up, and then took off. All this, including the bathroom time, took about 15 minutes! I had budgeted 20 minutes for each stop, and I was pleased that this first stop was ahead of schedule in addition to my running slightly ahead of schedule, because that gave me extra buffer if I slowed down later.
A 24 hour view of my CGM graph to show my glucose levels before (overnight), during the run including marks where my pump site likely unclipped, where I reclipped it, and how my glucose was in range for the remainder of the run.
LAP 2 (MILES 18-34)
The next lap was the same route as the first, and felt like a normal long run day. It was mid 40s and gradually warmed up to 63 F and actually felt hot for the second half! It hadn’t been 60+ degrees in Seattle since October (!) so my body wasn’t used to the “heat”. I was still feeling good physically and running well – in fact, I was running only ~10s slower than my average pace from lap 1! If I kept this up and didn’t fall off the pace much in the second lap, I would have a very nice buffer for the end of the race. I focused on this lap and only thought about these 16-17 miles. I did begin to squirt water from my camelback on to the ‘cooling’ visor I have, which evaporates and helps your head feel cooler – especially since I wasn’t used to the heat and was sweating more, that felt good. The end of the second lap, I started to feel like I was slightly under my ideal sodium levels. I’m pretty sensitive to sodium; I also drink a lot (I was carrying 3-3.5L for every 17 mile lap!); and I’m a salty sweater. Add increased heat, and even though I was right on track with my goal of about ~500mg/hour of sodium intake between my fuel and additional electrolyte pills, I felt a bit under, and so the next while I added an extra electrolyte pill to increase my sodium intake, and the feeling went away as expected.
(My glucose levels had come back down nicely within the first few miles of this lap, dipped down but as I was fueling every 30 minutes, came nicely into range and stayed 100% in range with no issues for the next ~12 hours of the run!)
This time, Scott was aware that I was ahead of expected paces and had been mapping my paces. He told me that if I stayed at that pace for the lap, I would be able to slow down to a 16 min/mi pace for lap 3 (16 miles) and down further to a 17 min/mi pace for the last (almost 13 miles) lap and still beat my goal time. That sounded good to me! He ended up biking out early to meet me so he could start charging my watch a few minutes early, and I ended up taking one of my next snacks – a warmed up frozen waffle – for my ‘last’ snack of the lap because it was time for a snack and there was no reason to wait even though it was part of the ‘next’ lap’s fuel plan. So I got to eat a warm waffle, which was nice!
Once we got almost there, Scott took my vest and biked ahead to begin the camelback process. I hit the turnaround, made another quick bathroom stop, and ran over to the table. This time, since it was 60s and I would finish my next lap while it was still above 50 degrees and light, I left my clothing layers as-is, other than a quick shirt switch to get rid of my sweaty shirt. I decided not to undo my shoes and check my feet for blisters; they felt fine and good. Because I didn’t need a shoe change or have anything going on to troubleshoot, I was in and out in 5 minutes! Hooray, that gave me another 10 minute buffer (in addition to 5 before, plus all my running ahead of schedule). I took off for lap 3, but warned Scott I would probably be slowing down.
LAP 3 (MILES 35-50)
The third lap was almost the same route, but shorter by a little less than a mile. I was originally concerned, depending on how much I had slowed down, that I would finish either right around sunset or after sunset, so that Scott might need to bring me out a long sleeve shirt and my waist lamp. However, I was ahead of schedule, so I didn’t worry about it, and again set out trying to not fall off my paces too much. I slowed down only a tiny bit on the way out, and was surprised at the turnaround point that I was now only slightly above a 15 min/mi pace! The last few miles I felt like slowing down more, but I was motivated by two thoughts: one was that I would finish this lap and essentially be at 50 miles. This meant, given my excellent pacing, that I would be “PR”ing my 50 mile pace. I’ve not run a standalone 50 miles before, just as part of my 82 mile when I wasn’t paying attention to pace at all (and ran 2-3 min/mi slower as a result), so I was focused on holding my effort level to be close to the same. Plus, after this lap, I “only” had a ~13 mile single lap left. That was my usual route, so it would be mentally easier, and it’s my last lap, so I knew I would get a mental boost from that. Psychologically, having the 50 mile mark to PR here really helped me hold my pace! I ended up only slowing down ~13s average pace compared to the ~10s deterioration between laps 1 and 2. I was pretty pleased with that, especially with hitting 50 miles then!
At this aid station stop, I was pretty cheerful even though I kept telling Scott I would be slowing down. I took ~10 minutes at this stop because I had to put my jacket back on around my waist and put my double headlamp on (which I wear around my waist) for when it got dark, plus do the normal refueling. I changed my short sleeve shirt again so I had a dry shirt, and debated but went ahead and put my fresh long sleeve shirt on and rolled up the sleeves. I figured I’d be putting it on as soon as it got dark, and I didn’t want to have to hassle with getting my vest on and off (while moving) in order to get the shirt on, especially because I’d also have to do that with my jacket later, so I went with the long sleeve shirt on and rolled up the sleeves for now. I had originally planned to put my long pants back on over my shorts, but it was still 63 degrees and the forecast was only going to get down to 45 degrees by midnight, and I seemed ahead of schedule and should finish by then. If I did get really cold, Scott could always bike out early and bring me more layers, but even 45 degrees in the dark with long sleeves, jacket, ear cover, and two pairs of gloves should be fine, so I went without the pants.
Speaking of ahead of schedule, I was! I had 5 minutes from the first aid station, 15 minutes from the second aid station, 5 minutes from this last aid station…plus another ~15 minutes ahead of what I thought my running time would have been at this point. Woohoo!
LAP 4 (MILES 51-63)
However, as soon as I walked off with my restocked vest, I immediately felt incredibly sore thighs. Ouch! My feet also started complaining suddenly. I did an extra walk interval and resumed my run/walking and my first mile out of the aid station stop was possibly my slowest mile (barring any with a bathroom stop) for the entire race, which is funny, because it was only about a 16:30 pace. But I figured it would be downhill from there and I’d be lucky to hold a sub 17 pace for these last 13 miles, especially because most of them would be in the dark and I naturally move a bit slower in the dark. Luckily, I was so far ahead that I knew that even a 17 min/mi average pace (or even slower) would be fine. However, I had joked to Scott coming into the end of lap 3 that I was tempted to just walk lap 4 (because I was finally starting to be tired) but then I’d have to eat more snacks, because I’d be out there longer. Sounds funny, but it was true – I was eating ok but occasionally I was having trouble swallowing my enzyme pills. Which is completely reasonable, I had been swallowing dozens of those (and electrolyte pills) all day and putting food down my throat for ~12+ hours consistently. It wasn’t the action of swallowing that was a problem, but I seemed to be occasionally mistiming how I would get the pills washed to the back of my mouth at the top of my throat to be able to swallow them down. Once or twice I had to take in some extra water, so it really wasn’t a big deal, but it was a slight concern that if I stopped being able to enzyme, I couldn’t fuel (because I have EPI) and I’d either have to tough it out without fueling (bad idea) or stop (not a fun idea). So I had that little extra motivation to try to keep run/walking!
Luckily, that first mile of the last lap was the worst. My thighs were still sore but less so and my feet stopped yelling at me and were back to normal. I resumed a reasonable run/walk pace, albeit at closer to a 15:30+ pace, which was a bigger jump from my previous lap average pace. I didn’t let it stress me out, but I was wishing I felt like fighting harder. But I didn’t, and focused on holding that effort level. I texted Scott, telling him I was averaging sub-16 pace (barely) at miles 4 and 5, then asking him to check my assumption that if I didn’t completely walk it in, I could maybe be an hour ahead of schedule? He confirmed that I “only” needed 16:53 average pace for the lap to come in at 10:30pm (75 minutes ahead of goal) and that if I kept sub-16 I could come in around 10:19pm. Hmmm, that was nice to hear! I didn’t think I would keep sub-16 because it was getting dark and I was tired, ~55 miles into the run, but I was pretty sure I’d be able to be sub 17 and likely sub 16:53! I carried on, turning my light on as it got dark. I was happily distracted by checking happy experiences off my mental list, mostly seeing bunnies beside and darting across the trail in the dark!
I hit the almost-halfway mileage point of the last lap, but even though it wasn’t halfway in mileage it felt like the last big milestone – it was the last mini-hill I had to climb to cross a bridge to loop around back to finish the lap. Hooray! I texted Scott and told him I coudn’t believe that, with ~7 miles left, I would be done in <2 hours. It was starting to sink in that I’d probably beat my goal of 11:45 and not doubt that it was real, and that I’d beat it by more than a few minutes. I then couldn’t resist – and was also worried Scott wouldn’t realize how well I was moving and be prone to coming out too late – and texted him again when I was <5 miles out and then 4 miles out. But by the time I was at 3 miles, he replied to ask if I needed anything else other than the bag I had planned for him to bring to the finish. Nope, I said.
At that point, I was back on my home turf, as I think about the last 2-3 miles that I run or walk on most days of the week. And I had run these miles 3 times already (in each direction, too), but it was pretty joyful getting to the point where I know not only every half mile marker but every tenth of a mile. And when I came up under the last bridge and saw a bright light biking toward me, it was Scott! He made it out to the 1.75 mile mark and rode in with me, which was fun. I was still holding just under sub-16 pace, too. I naturally pick up the pace when he’s biking with me – even when I’ve run 60+ miles! – and I was thinking that I’d be close but a few minutes under an hour and a half of schedule. It didn’t really matter exactly, but I like even numbers, yet I didn’t feel like I had tons of energy to push hard to the end – I was pleased enough to still be moving at a reasonable speed at this point!
Finally, about a half mile out, Scott biked ahead to set up the finish for me. (Purple painter’s tape and a sign I had made!) I glanced at my watch as I rounded the last corner, about .1 mile away, and though “oh, I was so close to beating the goal by over an hour and a half, too bad I didn’t push harder a few minutes ago so I could come in by 10:16 and be an hour and a half ahead”. I ran a tiny bit more but didn’t have much speed, walked a few last steps, then ran the rest of the way so Scott could video me coming into the finish. I could see the light from his bike’s light glowing on the trail, and as I turned the corner to the finish I was almost blinded by his waist light and his head lamp. I ran through the finish tape and grinned. I did it! He stopped videoing and told me to stop my trackers. I did but told him it didn’t matter, because I was somewhere under an hour and a half. We took a still picture, then picked up my tape and got ready to head home. I had done it! I had run 100k, beat my goal time…and it turns out I DID beat it by over an hour and a half! We checked the timestamp on the video Scott took of the finish and it has me crossing at 10:16pm, so that makes it a 16 hour and 16 minute finish – woohoo!
My last lap ended up being ~37 seconds average pace slower, so I had :10, :13, and :37 differences between the laps. Not too bad for that distance! I think I could’ve pushed a little harder, but I honestly didn’t feel like it psychologically, since I was already exceeding all of my goals, and I was enjoying focusing on the process meta-goals of trying to keep steady efforts and paces. Overall, my average pace was 15:36 min/mi which included ~30 min of aid station stops; and my average moving pace (excluding those 30 minutes of aid station time but did include probably another ~8-10 min of bathroom stops) was 15:17 min/mi. I’m pleased with that!
FUN STATS
One of the things I do for all training runs but also races is input my fueling as I go, because it helps me make sure I’m actually fueling and spot any problems as they start to develop. As I mentioned, at one point I felt a tiny bit low on sodium and sure enough, I had dipped slightly below 500mg/hr in the two hottest hours of the day when I had also been sweating more and drinking more than I had been previously. Plus, it means I have cool post-run data to see how much I consumed and figure out if I want to adjust my strategy. This time, though? I wouldn’t change a thing. I nailed it! I averaged 585 mg/hour of sodium across all ~16 hours of my run. I also averaged ~264 calories/hour, which is above my ~250/hr goal. I did skip – intentionally – the very last snack at the top of the 16th hour, and it still meant that I was above goal in all my metrics. I don’t set goals for carb intake, but in case you were wondering, I ended up averaging 29.9 grams of carbs/hour (min 12, max 50, and the average snack is 15.4 carbs), but that’s totally coincidental. Overall, I consumed 3,663 calories, which was 419 carbs, 195 g of fat, and 69 grams of protein.
With EPI, as I mentioned that means I have to swallow enzyme pills with every snack, which was every 30 minutes. I swallowed 71 OTC enzyme pills (!) to match all that fuel, plus 26 electrolyte pills…meaning I swallowed 97 pills in 16 hours. You can see why I get tired of swallowing!
Here’s a visual where you can see my consumption of calories, sodium, (and carbs) over the course of my race. The dip at the end is because I intentionally skipped the second snack of the hour 16 because I was almost done. Up to 15 hours (excluding the last hour), I had a slightly rolling increase in sodium/hr and a very slight decrease in calories/hr, with carbs/hr slightly increasing. Including the 16th hour (with a skipped snack intentionally), this changed the trends to slight rolling decrease in sodium/hr; the slight decrease trend in calories/hr continued; but it flattened the carbs/hr trend line to be neutral.
In contrast to my 82 mile where I had more significant fluctuations in sodium (and really felt it), I’m glad I was able to keep my sodium consumption at goal levels and also more easily respond when the conditions changed (hotter weather causing more sweat and more water intake than previous hours) so I could keep myself from getting into a hole sodium-wise. Overall, I feel like I get an A+ for executing my fueling and sodium strategy as planned. GI-wise, I get an A+++ because I had ZERO GI symptoms during and after the run! That’s really rare for any ultrarunners, let alone those of us with GI conditions (in my case, exocrine pancreatic insufficiency). Plus, despite the unclipped pump site and BG rise that resulted, I resumed back to typical running glucose levels for me and achieved 100% TIR 70-180 after that and I think likely 100% TIR for a more narrow range like 70-140, too, although I haven’t bothered to run those stats because I don’t care exactly what the numbers are. More importantly, I never went low, I never had any big drops or rises, and other than the brief 30 minutes of annoyance due to an unclipped pump site, diabetes did not factor any more into my thinking than blister management or EPI pill swallowing or sodium did – which is great!
Here’s a view of what I had leftover after my run. I had intentionally planned for an extra snack for every lap, plus I ran faster so I needed fewer overall. I also had packed extra enzymes and electrolytes for every lap, hoping I would never need to stress about running out on any individual lap – and I didn’t, so those amounts worked well.
POST-RUN RECOVERY
As soon as I stopped running and took a picture at the finish line, we got ready to head home. My muscles froze up as soon as I stopped, just like always, so I moved like a tin person for a few steps before I loosened back up and was able to walk normally. I got home, and was able to climb into the shower (and out!) without too much hardship. I climbed into bed, hydrated, and was able to go to sleep pretty normally for about 5 hours. I woke up at 5am pretty awake, which possibly was also due to the fact that I had been sleep shifting my sleep schedule, but I also felt really stiff and used the opportunity to point and flex my ankles. I slept every 20-30 minutes off and on for another few hours before I finally got up at 8am and THEN felt really sore and stiff! My right lower shin was sore and had felt sore just a tiny bit in the last few miles of my run, so it wasn’t surprising that it was sore. My right hip, which is the one I had been watching prior to the race, was sore again. I hobbled around the house and started to loosen up, enough that I decided that I would put shoes on and try to go for a short easy walk. Usually, I can’t psychologically fathom putting shoes on my feet after an ultra, but my feet felt really decent! I had some blisters, sure, but I hadn’t even noticed them running and they didn’t hurt to walk on. My hip and ankle were more noticeable. I didn’t try to take the stairs and used the elevator, then began hobbling down the sidewalk. Ouch. My hip was hurting so much that I stopped at the first bench and laid down on it to stretch my hip out. Then I walked .3 miles to the next bench and again stretched my hip. A little better, so we went out a bit farther with the plan to turn around, but my hip finally loosened up after a half mile where I could mostly walk normally! Hooray. In total, I managed 1.5 miles or so of a walk, which is pretty big for me the day after an ultra run.
Meaningfully, overnight, I still had 100% time in range (ideal glucose levels). I did not have to do any extra work, thanks to OpenAPS and autosensitivity which adjusts automatically to any increases and later return to normal insulin sensitivity from so much activity!
The next night, I slept even better, and didn’t notice any in-bed stiffness, although again on the second morning I felt stiff getting out of bed, but was able to do my full 5k+ walk route with my hip loosening up completely by a mile so that I didn’t even think about it!
On day 3, I feel 90% back to normal physically. I’m mostly fatigued,which Scott keeps reminding me is “as one should be” after runnning 100k! The nice change is that with previous ultras or long runs, I’ve felt brain fog for days or sometimes weeks – likely due to not fueling enough. But with my A+ fueling, my brain feels great – and good enough that it’s annoyed with my body still being a little bit tired. Interestingly, my body is both tired but also itching for more activity and new adventures. My friend compared it to “sea legs” where the brain has learned that the body should always be in motion, which is a decent analogy.
WHAT I HAVE LEARNED
I wouldn’t change anything in terms of my race pacing, execution, aid station stops, fueling, etc. for this run.
What I want to make sure I do next time includes continuing to adapt my training to listen to my body, rather than sticking to my pre-decided plan of how much to run. I feel like I can do that both because I now have 3000+ miles on my body of lifetime running (that I didn’t have for my first ultra); and I now have two ultras (last year’s 82 miles post-broken toe and this year’s 100k with minor hiccups like a sore shin and a hip at different times) where I was forced to or chose to adapt training, and it turned out just as good as I would have expected. For my 100k, I think the adaptation to 3 runs per week, all with my vest, ended up working well. This is the first run where I didn’t have noticeable shoulder soreness from my pack!
Same goes for taper: I don’t think, at my speed/skill level, that exact taper strategy makes a difference, and this experience confirmed it, doing DIY ultras and being able to flex a week forward or back based on how I’m physically feeling and when the best weather will be is now my preferred strategy for sure.
—-
If you’re new to ultras and haven’t read any of my other posts, consider reading some of the following, which I’ve alluded to in my post and directly contribute to the above situation being so positive:
Feel free to leave questions if you have any, either about slow ultra running in general or any other aspects of ultra running! I’m a places-from-last kind of ultra runner, but I’m happy to share my thinking process if it helps anyone else plan their own adventures.
I’ve previously written about ultrarunning preparation and a little bit about how I approach fueling. But it occurred to me there might be others out there wondering exactly HOW to find fuel that works for them, because it’s an iterative process.
The way I approach fueling is based on a couple of variables.
First and foremost, everything has to be gluten free (because I have celiac). So that limits a lot of the common ultrarunning fuel options. Things like bars (some are GF, most are not), Uncrustables, PopTarts, and many other common recommendations in the ultra community just aren’t an option for me. Some, I can find or make alternatives to, but it’s worth noting that being gluten free for celiac (where cross-contamination is also an issue, not just the ingredients) or having a food allergy and being an ultrarunner can make things more challenging.
Then, I also have exocrine pancreatic insufficiency. This doesn’t limit what I eat, but it factors in to how I approach ideal fueling options, because I have to match the enzyme amounts to the amount of food I’m eating. So naturally, the pill size options I have of OTC enzymes (one is lipase only and covers ~6g of fat for me, the other is a multi-enzyme option that includes protease to cover protein, and only enough lipase to cover ~4g of fat for me; I also have one much larger that covers ~15g of fat but I don’t typically use this one while running) influence the portion sizes of what I choose.
That being said, I probably – despite EPI – still tend toward higher fat options than most people. This is in part because I have had type 1 diabetes for 20+ years. While I by no means consume a low c-a-r-b diet, I typically consume less than the people with insulin-producing pancreases in my life, and lean slightly toward higher fat options because a) my taste buds like them and b) they’ve historically had less impact on my glucose levels. Reason A is probably the main reason now, thanks to automated insulin delivery, but regardless of reason, 20+ years of a higher level than most people’s fat consumption means I’m also probably better fat-adapted for exercise than most people.
Plus, ultrarunning tends to be slower than shorter runs (like marathons and shorter for most people), so that’s also more amenable to fat and other nutrient digestion. So, ultrarunners in general tend to have more options in terms of not just needing “gu” and “gel” and “blocks” and calorie-sugar drinks as fuel options (although if that is what you prefer and works well for you, great!).
All of these reasons lead me toward generally preferring fuel portions that are:
Gluten free with no cross-contamination risk
~20g of carbs
~10g of fat or less
~5-10g of protein or less
Overall, I shoot for consuming ~250 calories per hour. Some people like to measure hourly fuel consumption by calories. Others prefer carb consumption. But given that I have a higher tolerance for fat and protein consumption – thanks to the enzymes I need for EPI plus decades of practice – calories as a metric for hourly consumption makes sense for me. If I went for the level of carb intake many recommend for ultrarunners, I’d find it harder to consistently manage glucose levels while running for a zillion hours. I by no means think any of my above numbers are necessarily what’s best for anyone else, but that’s what I use based on my experiences to date as a rough outline of what to shoot for.
After I’ve thought through my requirements: gluten free, 250 calories per hour, and preferably no single serving portion size that is greater than 20ish grams of carbs or 10g of fat or 5-10g or protein, I can move on to making a list of foods I like and that I think would “work” for ultrarunning.
“Work” by my definition is not too messy to carry or eat (won’t melt easily, won’t require holding in my hands to eat and get them messy).
My initial list has included (everything here gluten free):
Oreos or similar sandwich type cookies
Yogurt/chocolate covered pretzels
PB or other filled pretzel nuggets
Chili cheese Fritos
Beef sticks
PB M&M’s
Reese’s Pieces
Snickers
Mini PayDays
Macaroons
Muffins
Fruit snacks
Fruit/date bars
GF (only specific flavors are GF which is why I’m noting this) of Honey Stinger Stroopwaffles
I wish I could include more chip/savory options on my lists, and that’s something I’ve been working on. Fritos are easy enough to eat from a snack size baggie without having to touch them with my hands or pull individual chips out to eat; I can just pour portions into my mouth. Most other chips, though, are too big and too ‘sharp’ feeling for my mouth to eat this way, so chili cheese Fritos are my primary savory option, other than beef sticks (that are surprisingly moist and easy to swallow on the run!).
Some of the foods I’ve tried from the above list and have eventually taken OFF my list include:
PB pretzel nuggets, because they get stale in baggies pretty fast and then they feel dry and obnoxious to chew and swallow.
Muffins – I tried both banana muffin halves and chocolate chip muffin halves. While they’re moist and delicious straight out of the oven, I found they are challenging to swallow while running (probably because they’re more dry).
Gluten free Oreos – actual Oreo brand GF Oreos, which I got burnt out on about the time I realized I had EPI, but also they too have a pretty dry mouthfeel. I’ve tried other brand chocolate sandwich cookies and also for some reason find them challenging to swallow. I did try a vanilla sandwich cookie (Glutino brand) recently and that is working better – the cookie is harder but doesn’t taste as dry – so that’s tentatively on my list as a replacement.
Other than “do I like this food” and “does it work for carrying on runs”, I then move on to “optimizing” my intake in terms of macronutrients. Ideally, each portion size and item has SOME fat, protein, and carbs, but not TOO MUCH fat, protein and carbs.
Most of my snacks are some fat, a little more carb, and a tiny bit of protein. The outlier is my beef sticks, which are the highest protein option out of my shelf-stable running fuel options (7g of fat, 8g of protein). Most of the others are typically 1-3g of protein, 5-10g of fat (perfect, because that is 1-2 enzyme OTC pills), and 10-20g of carb (ideal, because it’s a manageable amount for glucose levels at any one time).
Sometimes, I add things to my list based on the above criteria (gluten free with no cross-contamination list; I like to eat it; not messy to carry) and work out a possible serving size. For example, the other day I was brainstorming more fuel options and it occurred to me that I like brownies and a piece of brownie in a baggie would probably be moist and nice tasting and would be fine in a baggie. I planned to make a batch of brownies and calculated how I would cut them to get consistent portion sizes (so I would know the macronutrients for enzymes).
However, once I made my brownies, and started to cut them, I immediately went “nope” and scratched them off my list for using on runs. Mainly because, I hate cutting them and they crumbled. The idea of having to perfect how to cook them to be able to cut them without them crumbling just seems like too much work. So I scratched them off my list, and am just enjoying eating the brownies as brownies at home, not during runs!
—
I first started taking these snacks on runs and testing each one, making sure that they tasted good and also worked well for me (digestion-wise) during exercise, not just when I was sitting around. All of them, other than the ones listed above for ‘dry’ reasons or things like brownies (crossed off because of the hassle to prepare), have stayed on the list.
I also started looking at the total amount of calories I was consuming during training runs, to see how close I was to my goal of ~250 calories per hour. It’s not an exact number and a hard and fast “must have”, but given that I’m a slower runner (who run/walks, so I have lower calorie burn than most ultrarunners), I typically burn in the ballpark of ~300-400 calories per hour. I generally assume ~350 calories for a reasonable average. (Note, again, this is much lower than most people’s burn, but it’s roughly my burn rate and I’m trying to show the process itself of how I make decisions about fuel).
Aiming for ~250 calories per hour means that I only have a deficit of 100 calories per hour. Over the course of a ~100 mile race that might take 30 hours, this means I’ll “only” have an estimated deficit of 3,000 calories. Which is a lot less than most people’s estimated deficit, both because I have a lower burn rate (I’m slower) and because, as described above and below, I am trying to be very strategic about fueling for a number of reasons, including not ending up under fueling for energy purposes. For shorter runs, like a 6 hour run, that means I only end up ~600 calories in deficit – which is relatively easy to make up with consumption before and after the run, to make sure that I’m staying on top of my energy needs.
It turns out, some of my preferred snacks are a lot lower and higher calories than each other! And this can add up.
For example, fruit snacks – super easy to chew (or swallow without much chewing). 20g of carb, 0g of fat or protein, and only 80 calories. Another easy to quickly chew and swallow option: a mini date (fruit) bar. 13g carb, 5g fat, 2 protein. And…90 calories. My beef stick? 7g of fat, 8g of protein, and only 100 calories!
My approach that works for me has been to eat every 30 minutes, which means twice per hour. Those are three of my favorite (because they’re easy to consume) fuel options. If I eat two of those in the same hour, say fruit snacks and the date bar, that’s only 170 calories. Well below the goal of 250 for the hour! Combining either with my beef stick (so 180 or 190 calories, depending), is still well below goal.
This is why I have my macronutrient fuel library with carbs, fat, protein, *and* calories (and sodium, more on that below) filled out, so I can keep an eye on patterns of what I tend to prefer by default – which is often more of these smaller, fewer calorie options as I get tired at the end of the runs, when it’s even more important to make sure I’m at (or near) my calorie goals.
Tracking this for each training run has been really helpful, so I can see my default tendency to choose “smaller” and “easier to swallow” – but that also means likely fewer calories – options. This is also teaching me that I need to pair larger calorie options with them or follow on with a larger calorie option. For example, I have certain items on my list like Snickers. I get the “share size” bars that are actually 2 individual bars, and open them up and put one in each baggie. ½ of the share size package (aka 1 bar) is 220 calories! That’s a lot (relative to other options), so if I eat a <100 calorie option like fruit snacks or a date bar, I try to make it in the same hour as the above average option, like the ½ snickers. 220+80 is 300 calories, which means it’s above goal for the hour.
And that works well for me. Sometimes I do have hours where I am slightly below goal – say 240 calories. That’s fine! It’s not precise. But 250 calories per hour as a goal seems to work well as a general baseline, and I know that if I have several hours of at or greater than 250 calories, one smaller hour (200-250) is not a big deal. But this tracking and reviewing my data during the run via my tracking spreadsheet helps make sure I don’t get on a slippery slope to not consuming enough fuel to match the demands I’m putting on my body.
And the same goes for sodium. I have read a lot of literature on sodium consumption and/or supplementation in ultrarunning. Most of the science suggests it may not matter in terms of sodium concentration in the blood and/or muscle cramps, which is why a lot of people choose sodium supplementation. But for me, I have a very clear, distinct feeling when I get not enough sodium. It is almost like a chemical feeling in my chest, and is a cousin (but distinct) feeling to feeling ketones. I’ve had it happen before on long hikes where I drank tons to stay hydrated and kept my glucose levels in range but didn’t eat snacks with sodium nor supplement my water. I’ve also had it happen on runs. So for me, I do typically need sodium supplementation because that chemical-like feeling builds up and starts to make me feel like I’m wheezing in my chest (although my lungs are fine and have no issues during this). And what I found works for me is targeting around 500mg/hour of sodium consumption, through a combination of electrolyte pills and food.
(Side note, most ultrarunning blogs I’ve read suggest you’ll be just fine based on food you graze at the aid station. Well, I do most of my ultras as solo endeavors – no grazing, everything is pre-planned – and even if I did do an organized race, because of celiac I can’t eat 95% of the food (due to ingredients, lack of labeling, and/or cross contamination)…so that just doesn’t work for me to rely on aid station food to supplement me sodium-wise. But maybe it would work for other people, it just doesn’t for me given the celiac situation.)
I used to just target 500mg/hour of sodium through electrolyte pills. However, as I switched to actually fueling my runs and tracking carbs, fat, protein, and calories (as described above), I realized it’d be just as easy to track sodium intake in the food, and maybe that would enable me to have a different strategy on electrolyte pill consumption – and it did!
I went back to my spreadsheet and re-added information for sodium to all of my food items in my fuel library, and added it to the template that I duplicate for every run. Some of my food items, just like they can be outliers on calories or protein or fat or carbs, are also outliers on sodium. Biggest example? My beef stick, the protein outlier, is also a sodium outlier: 370mg of sodium! Yay! Same for my chili cheese Fritos – 210mg of sodium – which is actually the same amount of sodium that’s in the type of electrolyte pills I’m currently using.
I originally had a timer set and every 45 minutes, I’d take an electrolyte pill. However, in the last year I gradually realized that sometimes that made me over by quite a bit on certain hours and in some cases, I ended up WAY under my 500mg sodium goal. I actually noticed this in the latter portion of my 82 mile run – I started to feel the low-sodium chest feeling that I get, glanced at my sheet (that I hadn’t been paying close attention to because of So. Much. Rain) and realized – oops – that I had an hour of 323mg of sodium followed by a 495mg hour. I took another electrolyte pill to catch up and chose some higher sodium snacks for my next few fuels. There were a couple hours earlier in the run (hours 4 and 7) where I had happened to – based on some of my fresh fuel options like mashed potatoes – to end up with over 1000mg of sodium. I probably didn’t need that much, and so in subsequent hours I learned I could skip the electrolyte pill when I had had mashed potatoes in the last hour. Eventually, after my 82-mile run when I started training long runs again, I realized that keeping an eye on my rolling sodium tallies and tracking it like I tracked calories, taking an electrolyte pill when my hourly average dropped <500mg and not based on a pre-set time when it was >500mg, began to work well for me.
And that’s what I’ve been experimenting with for my last half dozen runs, which has worked – all of those runs have ended up with a total average slightly above 500mg of sodium and slightly above 250 calories for all hours of the run!
Now, you may be wondering – she tracks calories and sodium, what about fat and protein and carbs?
I don’t actually care about or use these in real-time for an hourly average; I use these solely as real-time decision in points as 1) for carbs, to know how much insulin I might need dependent on my glucose levels at the time (because I have Type 1 diabetes); and 2) the fat and protein is to make sure I take the right amount of enzymes so I can actually digest the fuel (because I have exocrine pancreatic insufficiency and can’t digest fuel without enzyme pills). I do occasionally look back at these numbers cumulatively, but for the most part, they’re solely there for real-time decision making at the moment I decide what to eat. Which is 95% of the time based on my taste buds after I’ve decided whether I need to factor in a higher calorie or sodium option!
For me, my higher sodium options are chili cheese Fritos, beef stick, yogurt covered pretzels.
For me, my higher calorie options are the ½ share size Snickers; chili cheese Fritos; Reese’s pieces; yogurt covered pretzels; GF honey stinger stroopwaffle; and 2 mini PayDay bars.
Those are all shelf-stable options that I keep in snack size baggies and ready to throw into my running vest.
Most of my ‘fresh’ food options, that I’d have my husband bring out to the ‘aid station’/turnaround point of my runs for refueling, tend to be higher calorie options. This includes ¼ of a GF PB&J sandwich (which I keep frozen so it lasts longer in my vest without getting squishy); ¼ of a GF ham and cheese quesadilla; a mashed potato cup prepared in the microwave and stuck in another baggie (a jillion, I mean, 690mg of sodium if you consume the whole thing but it’s occasionally hard to eat allll those mashed potatoes out of a baggie in one go when you’re not actually very hungry); sweet potato tots; etc.
So again, my recommendation is to find foods you like in general and then figure out your guiding principles. For example:
Do you have any dietary restrictions, food allergies or intolerances, or have already learned foods that your body Does Not Like while running?
Are you aiming to do carbs/hr, calories/hr, or something else? What amounts are those?
Do you need to track your fuel consumption to help you figure out how you’re not hitting your fuel goals? If so, how? Is it by wrappers? Do you want to start with a list of fuel and cross it off or tear it off as you go? Or like me, use a note on your phone or a drop down list in your spreadsheet to log it (my blog post here has a template if you’d like to use it)?
My guiding principles are:
Gluten free with no cross contamination risk (because celiac)
~250 calories per hour, eating twice per hour to achieve this
Each fuel (every 30 min) should be less than ~20g of carb, ~10g of fat, and ~5-10g of protein
I also want ~500mg of sodium each hour through the 2x fuel and when needed, electrolyte pills that have 210mg of sodium each
Dry food is harder to swallow; mouthfeel (ability to chew and swallow it) is something to factor in.
I prefer to eat my food on the go while I’m run/walking, so it should be all foods that can go in a snack or sandwich size baggie in my vest. Other options (like chicken broth, soup, and messy food items) can be on my backup list to be consumed at the aid station but unless I have a craving for them, they are secondary options.
Not a hassle to make/prepare/measure out into individual serving sizes.
Find foods that you like, figure out your guiding principles, and keep revising your list as you find what options work well for you in different situations and based on your running needs!
Recently, I’ve been thinking about the feeling I have that ultrarunning races (ultramarathons) are exclusionary.
Running is theoretically very accessible: you go out and do it. No special equipment or clothes needed. Same for ultrarunning: go run a distance longer than a marathon (26.2 miles or ~42 kilometers). You don’t even have to do it in an organized “race”, as many of us run DIY or solo ultramarathons for training or in lieu of races (like I did for my 82 miler). Run 26.3 miles? Technically you’re an ultrarunner (although it’s more common for a 50k/31 mile race to be the first distance most people consider ‘ultra’).
For many people, though, an organized ‘race’ or event is important for a number of reasons. It provides a commitment device and a firm and hard deadline for which to train. It might be the only safe way to achieve a distance, with aid stations and volunteers to support achieving the endeavor, if they don’t have family or friends able to crew runs otherwise or lack safe places to run these distances. It also provides motivation and camaraderie of setting out to achieve the same goal as a group of other people at the same time. And of course, it provides competition – not only with one’s self to achieve their best that day, but also against other people.
Most of us, though, statistically aren’t racing in an ultramarathon for a podium place or top-whatever finish.
So why do the rules work to exclude so many people from participating in ultramarathons?
I’m talking about rules like those often found listed in the 200 mile ultramarathon race descriptions and rule handbooks that say that aid cannot be administered outside of the aid station. Crew may not hand anything to racers outside of the aid station:
Cowboy 200, runner manual last updated 8/16/22: “Crew is only allowed to assist runners at FULL/MANNED aid stations. No exceptions. Crew cannot give anything to or take anything from runners anywhere except at manned aid stations.”
Bigfoot 200, 2022 runner manual: “Pacers are not allowed to mule (carry items) for their runner. Pacers may not give their runner any aid, food or water unless it is an emergency situation, in which case the runner may be disqualified. Pacers are for safety, not for giving aid or gaining an advantage over fellow participants.” and “Crew may not meet their runner between aid”
Tahoe 200, 2022 runner manual: A full disqualification may be given if “Contacts crew anywhere between aid stations; Has crew leave items left for the runner anywhere along the course; Takes outside aid between aid stations”
Moab 240, 2022 runner manual – same as above Tahoe 2022
Cocodona 250, accessed January 2023: “Crew may not meet their runner at any point on the course other than designated crew access aid stations. Runners will be automatically disqualified for receiving aid from crew outside of crew access aid stations.”
It’s a thing in 100 miles races, too.
Western States 100, 2023 participant guide: “Runners may not accept aid or assistance from their crew or other spectators in between crew-accessible aid stations.” and “Pacers may not carry water, food, flashlights, shoes, clothing, or other supplies for their runner or provide any other type of mechanical or physical assistance to their runner on the course.”
Hardrock 100, 2022 guide: “No stashing of supplies along the course and no accepting aid except within 400 yards of a designated aid station.” and “Pacers may not carry water, food, flashlights, shoes, clothing, or other supplies for their runner or provide any other type of mechanical or physical assistance to their runner on the course.”
Why is this a problem?
Well, say that an ultrarunner has type 1 diabetes and uses an insulin pump and the insulin pump breaks. (Battery dies; the pump itself smashes against a rock and breaks the screen; or like in my 82 miler last year, the water busts the button panel and it is no longer operable.) If you have a backup pump and a crew member, in a non-race setting they’d simply bike or run or drive out to you (whatever was feasible and safe for them) and hand you the pump. You’d replace it, and continue on your way.
But according to the ‘rules’ of these ultramarathon ‘races’, you’d be immediately disqualified and stopped from continuing the ultramarathon. In order to not be disqualified, you’d have to wait until you got to the aid station to swap to a backup insulin pump. Sure, you’d likely have a back up insulin delivery method (syringe or insulin pen), but those are stop gaps and not a strategy to get you to the end of the race, most likely. Knowing those rules, it incentivizes non-optimal decision making of participants to choose to continue for miles (in some cases, could be hours to the next crew-accessible aid station), all the while racking up high blood sugar and low insulin levels that can be really, really, physically unpleasant and further put ultrarunners at risk of physical injury due to the altered state of unnaturally high blood sugar levels.
My guess is these rules are there to limit cheating and a non-fair playing field for those competing for podium. (In some cases, it might be to limit traffic on narrow parts of trail, etc. so for safety reasons, but for the most part the reasons cited seem to be about ‘a fair playing field’.)
But you know what? It’s already an unfair playing field between them and people with diabetes: because those runners without diabetes have a fully functioning insulin production system inbuilt to their body! People with diabetes are already at a disadvantage. Allowing someone to switch to their backup insulin pump outside of an aid station isn’t an unfair advantage or “cheating”, nor does it even “level the playing field” with the other runners.
Instead, the ability to get medical supplies for a chronic disease outside of an aid station reduces medical and physical injury risk to the participant.
Maybe you think I’m being dramatic about the rules of these races and feeling excluded from participating. Because in fact, I do feel excluded. I know things can happen and there’s no point in paying hundreds or thousands of dollars to participate in an event where if I need to switch medical equipment mid-race and outside of an aid station, that I’ll be disqualified and receive an automatic DNF (did not finish) on my race record.
Further, there are other races with even more stringent rules that point blank exclude people with diabetes from participating at all in their races.
Yes, really.
In 2021, UTMB (one of the world’s top ultrarunning race series) announced a new medical policy (based on the Quartz Program) that forbids use of any substance on the WADA (World Anti-Doping Agency) Prohibited List that would require a TUE (therapeutic use exemption) within 7 days prior to competition or during competition.
Guess what’s on the WADA Prohibited List? Insulin.
So if you use insulin and are an athlete in another sport, you get a TUE approved and you’re allowed to participate in your sport despite using insulin for insulin-requiring diabetes.
But as a person with diabetes, you’re banned from participating in UTMB’s races! People with insulin-requiring diabetes can’t go 7 days prior to an event without insulin, nor can we go the entire race (hello, 105 miles takes a long time) without insulin. So this means we cannot participate.
This is dumb and outright exclusionary. There’s other people with healthcare conditions who are now outright banned from participating in UTMB races, too. The same exclusionary ‘health’ “program” has also been used by the Golden Trail Running Series.
This makes ultrarunning exclusionary for people with most chronic illnesses.
Think I’m being dramatic again? Check out this quote from an interview with the organizer of the health ‘program’ that UTMB used to generate this list of requirements:
“Whether the athlete is under the influence of drugs or sick, our role consists of protecting them and therefore stop them from starting the race.”
They outright say they’re trying to stop athletes from starting the race, under the guise of policing what is healthy and safe for trail and ultrarunning. It doesn’t allow for individual evaluation.
Point blank: I’m excluded, and so are many other people with chronic illnesses, despite the fact that we are likely in better health than many other prospective participants of the race, regardless of chronic illness.
Personally, I think having a chronic illness, as hard as it makes ultrarunning, makes me better prepared and a better ultrarunner: I am very experienced with listening to my body and adjusting to challenging situations and dealing with physical and medical adversity. I do ultramarathons in part because they are hard and challenging. They’re hard and challenging for everyone! That’s why so few (relatively speaking) people run ultramarathons. If it was easy, everyone would have done it.
But no one should be prevented from entering a race because of living with a chronic illness.
If you’re willing to put in the training and cover the miles and plan what you need to do in order to achieve this with your medical devices and life-critical medications? You should do so. You should not be discouraged from taking the best possible care of your body before, during, and after an ultramarathon. That is what these policies do at best: at worst they exclude you outright from entering the race.
Race directors and race organizers, your ultramarathon policies are exclusionary. You should fix them.
—
Fellow ultrarunners, I encourage you to ask race directors to update their policies, too.
How?
Take a leaf out of Tunnel Hill 100’s book. They say (bold emphasis mine):
“USATF SPECIAL NOTICE: No American, or World Record, including age group records, will be recognized for any athlete who:
1) receives aid outside of a designated Aid Station area, OR
2) uses a pacer who is not entered in the race. These rules fall under the “unfair advantage” rules.
NOTE: Don’t worry about these rules if you aren’t going to set any records other than your own personal records.“
This is how it should be done: make it clear what rules apply to elite/pro runners (aka podium/top 10/whatever places get rank or $$$) and which ones do NOT apply to the rest of us.
Don’t make people with chronic diseases pay yet another time tax to have to contact the race director and (in the US) ask for an accommodation under the Americans with Disabilities Act. Or point out, if declined, that it’s illegal to exclude people with disabilities (which includes people with most chronic diseases). We do enough work and already pay a lot of “time tax” for acquiring health supplies and managing our chronic diseases; don’t put MORE hoops in front of us to be able to participate and run.
That’s not equitable, nor fun, and it’s yet another barrier to keep more people out of running these races and events.
Eating gluten free for the rest of your life, because you were diagnosed with celiac disease? Heard that response (I could never do that) for going on 14 years.
Inject yourself with insulin or fingerstick test your blood glucose 14 times a day? Wear an insulin pump on your body 24/7/365? Wear a CGM on your body 24/7/365?
Yeah, I’ve heard you can’t do that, either. (For 20 years and counting.) Which means I and the other people living with the situations that necessitate these behaviors are…doing this for fun?
We’re not.
More recently, I’ve heard this type of comment come up about tracking what I’m eating, and in particular, tracking what I’m eating when I’m running. I definitely don’t do that for fun.
—
I have a 20+ year strong history of hating tracking things, actually. When I was diagnosed with type 1 diabetes, I was given a physical log book and asked to write down my blood glucose numbers.
“Why?” I asked. They’re stored in the meter.
The answer was because supposedly the medical team was going to review them.
And they did.
And it was useless.
“Why were you high on February 22, 2003?”
Whether we were asking this question in March of 2003 or January of 2023 (almost 20 years later), the answer would be the same: I have no idea.
BG data, by itself, is like a single data point for a pilot. It’s useless without the contextual stream of data as well as other metrics (in the diabetes case, things like what was eaten, what activity happened, what my schedule was before this point, and all insulin dosed potentially in the last 12-24h).
So you wouldn’t be surprised to find out that I stopped tracking. I didn’t stop testing my blood glucose levels – in fact, I tested upwards of 14 times a day when I was in high school, because the real-time information was helpful. Retrospectively? Nope.
—
I didn’t start “tracking” things again (for diabetes) until late 2013, when we realized that I could get my CGM data off the device and into the laptop beside my bed, dragging the CGM data into a CSV file in Dropbox and sending it to the cloud so an app called “Pushover” would make a louder and different alarm on my phone to wake me up to overnight hypoglycemia. The only reason I added any manual “tracking” to this system was because we realized we could create an algorithm to USE the information I gave it (about what I was eating and the insulin I was taking) combined with the real-time CGM data to usefully predict glucose levels in the future. Predictions meant we could make *predictive* alarms, instead of solely having *reactive* alarms, which is what the status quo in diabetes has been for decades.
At the beginning of 2020, my life changed. Not because of the pandemic (although also because of that), but because I began to have serious, very bothersome GI symptoms that dragged on throughout 2020 and 2021. I’ve written here about my experiences in eventually self-diagnosing (and confirming) that I have exocrine pancreatic insufficiency, and began taking pancreatic enzyme replacement therapy in January 2022.
What I haven’t yet done, though, is explain all my failed attempts at tracking things in 2020 and 2021. Or, not failed attempts, but where I started and stopped and why those tracking attempts weren’t useful.
Once I realized I had GI symptoms that weren’t going away, I tried writing down everything I ate. I tried writing in a list on my phone in spring of 2020. I couldn’t see any patterns. So I stopped.
A few months later, in summer of 2020, I tried again, this time using a digital spreadsheet so I could enter data from my phone or my computer. Again, after a few days, I still couldn’t see any patterns. So I stopped.
I made a third attempt to try to look at ingredients, rather than categories of food or individual food items. I came up with a short list of potential contenders, but repeated testing of consuming those ingredients didn’t do me any good. I stopped, again.
When I first went to the GI doctor in fall of 2020, one of the questions he asked was whether there was any pattern between my symptoms and what I was eating. “No,” I breathed out in a frustrated sigh. “I can’t find any patterns in what I’m eating and the symptoms.”
So we didn’t go down that rabbit hole.
At the start of 2021, though, I was sick and tired (of being sick and tired with GI symptoms for going on a year) and tried again. I decided that some of my “worst” symptoms happened after I consumed onions, so I tried removing obvious sources of onion from my diet. That evolved to onion and garlic, but I realized almost everything I ate also had onion powder or garlic powder, so I tried avoiding those. It helped, some. That then led me to research more, learn about the categorization of FODMAPs, and try a low-FODMAP diet in mid/fall 2021. That helped some.
Then I found out I actually had exocrine pancreatic insufficiency and it all made sense: what my symptoms were, why they were happening, and why the numerous previous tracking attempts were not successful.
You wouldn’t think I’d start tracking again, but I did. Although this time, finally, was different.
When I realized I had EPI, I learned that my body was no longer producing enough digestive enzymes to help my body digest fat, protein, and carbs. Because I’m a person with type 1 diabetes and have been correlating my insulin doses to my carbohydrate consumption for 20+ years, it seemed logical to me to track the amount of fat and protein in what I was eating, track my enzyme (PERT) dosing, and see if there were any correlations that indicated my doses needed to be more or less.
My spreadsheet involved recording the outcome of the previous day’s symptoms, and I had a section for entering multiple things that I ate throughout the day and the number of enzymes. I wrote a short description of my meal (“butter chicken” or “frozen pizza” or “chicken nuggets and veggies”), the estimate of fat and protein counts for the meal, and the number of enzymes I took for that meal. I had columns on the left that added up the total amount of fat and protein for the day, and the total number of enzymes.
It also helped me see that within the first month, I was definitely improving, but not all the way – in terms of fully reducing and eliminating all of my symptoms. So I continued to use it to titrate my enzyme doses.
Then it helped me carefully work my way through re-adding food items and ingredients that I had been avoiding (like onions, apples, and pears) and proving to my brain that those were the result of enzyme insufficiency, not food intolerances. Once I had a working system for determining how to dose enzymes, it became a lot easier to see when I had slight symptoms from slightly getting my dosing wrong or majorly mis-estimating the fat and protein in what I was eating.
It provided me with a feedback loop that doesn’t really exist in EPI and GI conditions, and it was a daily, informative, real-time feedback loop.
As I reached the end of my first year of dosing with PERT, though, I was still using my spreadsheet. It surprised me, actually. Did I need to be using it? Not all the time. But the biggest reason I kept using it relates to how I often eat. I often look at an ‘entree’ for protein and then ‘build’ the rest of my meal around that, to help make sure I’m getting enough protein to fuel my ultrarunning endeavors. So I pick my entree/main thing I’m eating and put it in my spreadsheet under the fat and protein columns (=17 g of fat, =20 g of protein), for example, then decide what I’m going to eat to go with it. Say I add a bag of cheddar popcorn, so that becomes (=17+9 g of fat) and (=20+2 g of protein), and when I hit enter, those cells now tell me it’s 26 g of fat and 22 g of protein for the meal, which tells my brain (and I also tell the spreadsheet) that I’ll take 1 PERT pill for that. So I use the spreadsheet functionally to “build” what I’m eating and calculate the total grams of protein and fat; which helps me ‘calculate’ how much PERT to take (based on my previous titration efforts I know I can do up to 30g of fat and protein each in one PERT pill of the size of my prescription)
Essentially, this has become a real-time calculator to add up the numbers every time I eat. Sure, I could do this in my head, but I’m usually multitasking and deciding what I want to eat and writing it down, doing something else, doing yet something else, then going to make my food and eat it. This helps me remember, between the time I decided – sometimes minutes, sometimes hours in advance of when I start eating and need to actually take the enzymes – what the counts are and what the PERT dosing needs to be.
I have done some neat retrospective analysis, of course – last year I had estimated that I took thousands of PERT pills (more on that here). I was able to do that not because it’s “fun” to track every pill that I swallow, but because I had, as a result of functional self-tracking of what I was eating to determine my PERT dosing for everything I ate, had a record of 99% of the enzyme pills that I took last year.
I do have some things that I’m no longer entering in my spreadsheet, which is why it’s only 99% of what I eat. There are some things like a quick snack where I grab it and the OTC enzymes to match without thought, and swallow the pills and eat the snack and don’t write it down. That maybe happens once a week. Generally, though, if I’m eating multiple things (like for a meal), then it’s incredibly useful in that moment to use my spreadsheet to add up all the counts to get my dosing right. If I don’t do that, my dosing is often off, and even a little bit “off” can cause uncomfortable and annoying symptoms the rest of the day, overnight, and into the next morning.
So, I have quite the incentive to use this spreadsheet to make sure that I get my dosing right. It’s functional: not for the perceived “fun” of writing things down.
–
It’s the same thing that happens when I run long runs. I need to fuel my runs, and fuel (food) means enzymes. Figuring out how many enzymes to dose as I’m running 6, 9, or 25 hours into a run gets increasingly harder. I found that what works for me is having a pre-built list of the fuel options; and a spreadsheet where I quickly on my phone open it and tap a drop down list to mark what I’m eating, and it pulls in the counts from the library and tells me how many enzymes to take for that fuel (which I’ve already pre-calculated).
It’s useful in real-time for helping me dose the right amount of enzymes for the fuel that I need and am taking every 30 minutes throughout my run. It’s also useful for helping me stay on top of my goal amounts of calories and sodium to make sure I’m fueling enough of the right things (for running in general), which is something that can be hard to do the longer I run. (More about this method and a template for anyone who wants to track similarly here.)
–
The TL;DR point of this is: I don’t track things for fun. I track things if and when they’re functionally useful, and primarily that is in real-time medical decision making.
These methods may not make sense to you, and don’t have to.
It may not be a method that works for you, or you may not have the situation that I’m in (T1D, Graves, celiac, and EPI – fun!) that necessitates these, or you may not have the goals that I have (ultrarunning). That’s ok!
But don’t say that you “couldn’t” do something. You ‘couldn’t’ track what you consumed when you ran or you ‘couldn’t’ write down what you were eating or you ‘couldn’t’ take that many pills or you ‘couldn’t’ inject insulin or…
You could, if you needed to, and if you decided it was the way that you could and would be able to achieve your goals.
One of these books I wrote years ago, about a month or so after I broke my ankle, inspired by the initial reactions from one of my nephews about me being on crutches. This new book is called Cooper’s Crutches.
I let it sit for several years, though, because I didn’t have illustrations for it. I’ve used a different illustrator or artist for each of my books so far.
My first book, Carolyn’s Robot Relative, was illustrated with art by my aunt, Sandra Massengill.
My second book, Parker’s Peanut Butter, was illustrated by an artist I met through a workshop, Beatrice Baumgartner-Cohen.
The answer is: not yet. It’s hard to create a character who persists throughout image generation for enough scenes that can fit a two-dozen page storyline, although it would probably work for one or two images! (Especially if you managed to AI-illustrate a character that you could then place in various AI-illustrated scenes. The challenge is also having different poses for the same character, to illustrate a story.)
It then occurred to me to search around and I stumbled across a library of free, open source illustrations. Woohoo! Maybe those would work. Actually, I couldn’t even download that one due to a bug in their site, so I started searching (now that I knew to look for it) and found several other sets of illustrations. I even found a site called Blush that had a series of illustrations by various artists, and a web interface (GUI) that allowed you to modify images slightly then download them.
It’s like paper dolls, but digital – you can adjust the coloring of the hair, hair style, accessories, etc to modify the illustrated character.
I gave it a try, building some illustrations and downloading them. I then did some DIY-ing again in PowerPoint to modify them to help illustrate the full story in my children’s book. I printed a proof copy, but the versions I had downloaded for free were too low resolution and were fuzzy. However, the idea as a whole had worked great! I signed up for a free trial of the “Pro” version of Blush which enabled me to download both high-resolution PNG (image) files as well as SVG files.
Having SVG files theoretically would enable me to further modify and customize these, but as a non-illustrator even though I could load them in Figma and modify them, I still struggled to export them as high-enough resolution to work for printing in a book. I gave up and went back to DIY-ing the modifications in PowerPoint. They’re not perfect, but for the use case of my books (for a very small, niche audience), I doubt they care that they’re not perfect.
Here’s a selection of a few of the pages (not in order) in Cooper’s Crutches:
At the same time that I started playing with these illustrations, I wondered whether I had any more ideas for books that I could illustrate at the same time with the same methods. I had had Cooper’s book written and waiting to illustrate; I now had a method to illustrate, but I wasn’t sure what story to illustrate.
But like all of my children’s books, inspiration again struck based on a situation and conversation I had with one of my nieces. She’s newly lactose intolerant and is taking lactase any time she has milk, like with milk and cookies for a bedtime snack. Lactase is an enzyme…and I’ve been taking enzymes of another sort this year, for exocrine pancreatic insufficiency.
Here’s a selection of a few of the pages (not in order) in the book:
—
Both Cooper’s Crutches and Chloe’s Cookies are illustrated with illustrations from a variety of artists who make their work available on Blush, including: Veronica Iezzi; Susana Salas; Pau Barbaro; Ivan Mesaroš; Mariana Gonzalez Vega; Deivid Saenz; and Cezar Berje.
The neat thing about Blush is their license: you can use the illustrations in any way, including commercial products, and you can modify or combine it with other works (like I did, modifying the images and combining illustrations from various artists) however you like.
—
I think I’ve likely maximized my use of Blush between these two books; unless other collections get uploaded in the future. But if you need a handful of illustrations that you can customize, definitely check it out!
And if you have ideas for other cool illustration libraries that I could use for future books, please let me know! (Or if you’re an artist who would like to contribute to one of my future books. )
—
TLDR: I have two new children’s books, and you can find “Cooper’s Crutches” and “Chloe’s Cookies” on Amazon in paperback and Kindle formats.
I’ve had exocrine pancreatic insufficiency (EPI or PEI) for a full year now and have been taking pancreatic enzyme replacement therapy (PERT) ever since diagnosis.
In 365 days of pancreatic enzyme replacement therapy, I have consumed (at least) 3,277 pills.
That’s an average of 8.98 pills per day!
As I previously wrote, the number of pills is in part because I’m trying to lower the total costs (to everyone involved in paying for it) of my PERT by taking a mix of prescription PERT and OTC enzymes to try to balance effective dosing, cost, and the number of pills I swallow. I take one pill with my standard breakfast, so the remaining ~8 average pills are usually split between lunch, dinner, and/or a snack if I have one. (This is also influenced by my ultrarunning where I typically take ~2 pills every 30 minutes with my snacks/fuel for running, so long training days of 4 hours would involve 8 or more pills just for running fuel; obviously longer runs would involve even more, which drives the pills/day average higher.) If I wanted to reduce the total number of pills, I could by driving up the cost by using bigger, prescription PERT pills in lieu of some of the OTC options. However, most of the time, 3-4 pills per meal mixed between prescription and OTC is doable for me. I typically would choose to round up more PERT and reduce OTC pill count when I’m less certain about the macronutrient content of the meal or I want more confidence in better outcomes.
Speaking of better outcomes – is PERT effective?
For me, yes!
Overall, I feel so much better. Most of the time, I hardly ever have ANY symptoms (such as gas, bloating, or feeling icky) let alone my more extreme symptoms of “disrupting” my GI system. In the year of taking PERT, 78% of the time I had no disruption or any noticeable symptoms.
The average length of time between days with noticeable symptoms was 5.37 days.
And, if you look at the second half of the year, this increased quite a bit: 88% of the time I had no noticeable symptoms and the streak length of days between symptom days increased to 6.81 average days! The max streak is now 28 days (and counting)!
That’s approaching a full month without any GI symptoms (woohoo) of any kind, and means less than 1 or 2 instances of symptoms per month for me in the last several months. That’s probably better than average for most people, even people without known GI conditions, and getting a lot closer back to my personal level of “normal”.
And obviously, this is continuing to increase over time as I improve my PERT dosing strategy.
This is pretty meaningful to think about.
PERT made a difference overall straight away, but I was also starting with very small portions of food and a very restricted diet. (This is because before I realized I had EPI I had done all kinds of behavioral gymnastics to try to eliminate foods like onion, garlic, and other foods that seemed to cause issues). So first I figured out PERT successfully for what I was eating; then carefully expanded my portion sizes back to typical quantities of food; then slowly expanded my diet to cover all the foods I used to eat before I started having all my GI problems.
It very much felt like I had three phases this year:
Phase 1: Use PERT to cover small quantities of small varieties of food. Figure out what foods I could eat that could “fit” into one PERT pill.
Phase 2: Start to figure out what quantities of food I wanted to eat, and get the PERT to match the food.
Phase 3: Finish expanding out my food choices to cover everything I was eating before and tackling all my “firsts” with PERT.
You can see this evolution in my diet, too, when you look at the relative changes in the amount of fat and protein I have eaten over the course of the year. (The one big obvious outlier on the graph in October is my 82 mile ultramarathon where I ate every 30 minutes for 25 hours!) There’s been a slight increase in my fat consumption over the course of the year, and protein consumption has stayed relatively flat as I’ve been making a very conscious effort to eat enough protein to fuel my ultrarunning endeavors throughout the year.
You can then see the relationship with increased number of pills (albeit pills with different amounts of lipase) over the course of the year, relative to the fat and protein consumed.
(Note that the pills per day is using a hidden right axis, whereas the fat and protein share the same left axis numbers, also not shown)
For anyone who is new (just diagnosed or recently diagnosed within a few weeks or months) to EPI, here’s what I would hope you take away:
PERT works, but it needs to match what you are eating. Come up with a strategy (here’s mine – you can use it!) to adjust your dosing to match what you are eating. What you eat changes, and so should your PERT dosing.
Things will improve over time, and you will get more effective at matching your dosing to what you are eating. You should be able to have more and more “streaks” of days without symptoms, or with reduced symptoms. However, this may take a few months, because you’ll likely also be – at the same time – re-expanding your variety of foods that you’re eating. The combination of eating more and different foods AND tweaking your dosing can make it take a little bit longer to figure it all out.
If you’re not seeing success, talk with your doctor. There are different sizes of PERT pills – if you’re struggling to take X number of pills, you may be able to take fewer pills of a bigger size. There are different brands of PERT – so if one isn’t working for you (after you match your dosing to how much fat and protein is in each meal), you can switch and try another brand. There are also OTC options, which you can use to “top off” your prescription PERT or substitute, but you need to have an effective strategy for adjusting your dose that you can translate to your OTCs to be sure that they’re working.
I ended up writing a post last year recapping 2021, in part because I felt like I did hardly anything – which wasn’t true. In part, that was based on my body having a number of things going on that I didn’t know at the time. I figured those out in 2022 which made 2022 hard and also provided me with a sense of accomplishment as I tackled some of these new challenges.
For 2022, I have a very different feeling looking back on the entire year, which makes me so happy because it was night and day (different) compared to this time last year.
I started taking enzymes (pancreatic enzyme replacement therapy, known as PERT) in early January. And they clearly worked, hooray!
I quickly realized that like insulin, PERT dosing needed to be based on the contents of my meals. I figured out how to effectively titrate for each meal and within a month or two was reliably dosing effectively with everything I was eating and drinking. And, I was writing and sharing my knowledge with others – you can see many of the posts I wrote collected at DIYPS.org/EPI.
I even published a peer-reviewed journal article about EPI – submitted within 4 months of confirming that I had it! You can read that paper here with an analysis of glucose data from both before and after starting PERT. It’s a really neat example that I hope will pave the way for answering many questions we all have about how particular medications possibly affect glucose levels (instead of simply being warned that they “may cause hypoglycemia or hyperglycemia” which is vague and unhelpful.)
However with the broken toe, I took the time off needed and carefully built back up, put a lot of planning into it, and made my attempt in late October instead.
Eating every 30 minutes like clockwork, consuming enzymes (more than 92 pills!), which means 50 snacks consumed. No GI issues, either, which is remarkable even for an ultrarunner without EPI!
Professionally, I did quite a lot of miscellaneous writing, research, and other activities.
I spent a lot of time doing research. I also peer reviewed more than 24 papers for academic journals. I was asked to join an editorial board for a journal. I served on 2 grant review committees/programs.
I had 13 papers published (with several more in the queue already written and submitted but will be published next year if accepted). You can see links to all of my published research at DIYPS.org/research
*by ton, I mean way more than the past couple of years combined. Some of that has been due to getting some energy back once I’ve fixed missing enzyme and mis-adjusted hormone levels in my body! I’m up to 40+ blog posts this year.
And personally, the punches felt like they kept coming, because this year we also found out that I have Graves’ disease, taking my chronic disease count up to 4. Argh. (T1D, celiac, EPI, and now Graves’, for those curious about my list.)
My experience with Graves’ has included symptoms of subclinical hyperthyroidism (although my T3 and T4 are in range), and I have chosen to try thyroid medication in order to manage the really bothersome Graves’-related eye symptoms. That’s been an ongoing process and the symptoms of this have been up and down a number of times as I went on medication, reduced medication levels, etc.
What I’ve learned from my experience with both EPI and Graves’ in the same year is that there are some huge gaps in medical knowledge around how these things actually work and how to use real-world data (whether patient-recorded data or wearable-tracked data) to help with diagnosis, treatment (including medication titration), etc. So the upside to this is I have quite a few new projects and articles coming to fruition to help tackle some of the gaps that I fell into or spotted this year.
—
And that’s why I’m feeling optimistic, and like I accomplished quite a bit more in 2022 than in 2021. Some of it is the satisfaction of knowing the core two reasons why the previous year felt so physically bad; hopefully no more unsolved mysteries or additional chronic diseases will pop up in the next few years. Yet some of it is also the satisfaction of solving problems and creating solutions that I’m uniquely poised, due to my past experiences and skillsets, to solve. That feels good, and it feels good as always to get to channel my experiences and expertise to try to create solutions with words or code or research to help other people.
I’ve had exocrine pancreatic insufficiency (known as EPI or PEI) for a year now. I have had type 1 diabetes for 20+ years and am experienced in adjusting my medication (previously insulin) in response to everything that I eat or drink.
With EPI, though, most people are given a static prescription, such as one saying “take 3 pills with each meal”.
Well, what if every meal is not the same size?
Let’s think about a couple of hypothetical meals.
Meal A: Baked chicken, sweet potato, and broccoli. This meal likely results in ~31 grams of carbohydrates; 7 grams of fat; and ~30 grams of protein.
How would you dose for this meal? Most people do what they are told and dose based on the fat content of the meal. If they typically take 3 pills, they may take all 3 pills or take fewer pills if this is less fat than their typical meal.
Many people post in EPI social media groups post about restaurant dinners that sound like this complaining about side effects they experience with this type of meal. The commonly mentioned theory is that maybe the chicken is cooked in oil. However, the entire meal is so low in fat compared to other meals that it is unlikely to be the fat content causing symptoms if the typical meal dose of PERT is used, even if the chicken is cooked in oil.
Let’s discuss another meal.
Meal B: A bowl of chili topped with cheddar cheese and a piece of cornbread.
This meal results in ~45 grams of carbs; ~30 grams of fat; and ~42 grams of protein.
—
The fat content between these two meals is quite a bit different (7 grams of fat versus 30 grams of fat). Yet, again, most people are told simply to dose by the amount of fat, so someone might take a lower dose for the chicken meal because it has so little fat relative to other meals.
This could result in symptoms, though. The pancreas actually produces THREE kinds of enzymes. That’s why pancreatic enzyme replacement therapy medicine, called pancrelipase as a common name, has THREE types of enzymes: lipase, to help digest fat; protease, to help digest protein; and amylase, to help digest carbohydrates. A typical PERT pill has different amounts of these three enzymes, although it is usually described by the size/quantity of lipase it has – yet the other enzymes still play an important role in digestion.
I’ve observed that it’s pretty common for people to completely ignore the protein in what they’re eating. But as I mentioned, that seems to be the most obvious thing to try dosing for if “low fat” meals are causing issues. (It could also be sensitivity to carbohydrates, but the above example meal is fairly low carbohydrate.) My personal experience has also been that I am sensitive to fat and protein, and dose my meals based on these macronutrients, but other than eating fruit on an empty stomach (when I would add PERT/enzyme, despite the zero fat and protein in it), I don’t need to dose based on carbohydrates.
But I do need to dose for BOTH fat AND protein in what I’m eating. And I have a theory that a lot of other people with EPI do, too.
So how do you do this?
How do you dose for meals of different sizes, and take into account both fat and protein for these varying meals?
First, you need to figure out what dosing “works” for you.
Most people begin experimenting and find a quantity of food that they can eat with the dose that they typically take. This meal size is going to vary person to person; it’ll also vary based on what it is in the meal they’re eating (such as chicken vs chili, from the above examples).
Once you find a dose that “works” and try it out a few times on the same meal, you can use this to determine what your dosing should be.
How?
Let’s use two examples with different dose sizes and types of PERT.
(PS – did you know there are 6 FDA-approved PERT brands in the US? Sometimes one works for someone where a different brand does not. If you’re struggling with the first type of PERT you’ve been prescribed, and you’ve already ruled out that you’re dosing correctly (see below), make sure to talk to your doctor and ask about trying a different brand.)
First, you can calculate the ratios of lipase needed per gram of fat.
Let’s say the meal that “works” with your typical dose is 30 grams of fat. If 30 grams of fat is fine on your current dose, I would eat another meal with a slightly higher amount of fat (such as 35 or 40 grams of fat). When you get to an amount that “doesn’t work” – meaning you get symptoms – then you go back to the dose that does “work” to use in the math.
If the meal that “worked” was 30 grams of fat I would do the following math for each of these two examples:
—
Example A: You need 1 pill of Zenpep 25,000 to cover this meal
Example B: You need 3 pills of Creon 36,000 to cover this meal
—
Example A: 1 pill of Zenpep 25,000 is 1 multiplied by 25,000, or 25,000 units of lipase. Take that (25,000) and divide it by the grams of fat in the meal that works (30 grams). This would be 25,000/30 = 833. This means you need 833 units of lipase to “cover” 1 gram of fat. You can round up to ~1000 units of lipase to make it easier; your ratio would be 1000 units of lipase for every 1 gram of fat.
Example B: 3 pills of Creon 36,000 is 3 multiplied by 36,000, which is 108,000 units of lipase. Take that number (108,000) and divide it by the grams of fat in the meal that works (30 grams). This would be 108,000/30 = 3,600. This means you need 3,600 units of lipase to “cover” 1 gram of fat.
The next time you wanted to eat a meal, you would look at the grams of fat in a meal.
Let’s say you’re going to eat two bowls of chili and two pieces of cornbread. Let’s assume that is about 64 grams of fat. (Two bowls of chili and two cornbread is 30×2=60, plus a bit of butter for the cornbread so we’re calling it 64 grams of fat).
Example A: Take the meal and multiply it by your ratio. 64 (grams of fat) x 1,000 (how many units of lipase you need to cover 1 grant of fat) = 64,000. A Zenpep 25,000 has 25,000 lipase. Since you need 64,000 (units of lipase needed to cover the meal), you would divide it by your pill/dose size of 25,000. 64,000 divided by 25,000 is 2.56. That means for these ratios and a prescription of Zenpep 25,000 pill size, you need *3* Zenpep 25,000 to cover a meal of 64g of fat. (Remember, you can’t cut a PERT, so you have to round up to the next pill size.)
Example B: Take the meal and multiply it by your ratio. 64 (grams of fat) times 3,600 (how many units of lipase you need to cover 1 grant of fat) = 230,400. A Creon 36,000 has 36,000 lipase. Since you need 230,400 units of lipase to cover the meal, you would divide it by your pill/dose size of 36,000. 230,400 divided by 36,000 is 6.4. This means you need *7* Creon 36,000 to cover a meal of 64g of fat. (Again, you can’t cut a PERT, so you have to round up to 7 from 6.4.)
Another way to think about this and make it easier in the future is to determine how much one pill “covers”.
Example A: A Zenpep 25,000 “covers” 25 grams of fat if my ratio is 1000 units of lipase for every gram of fat (25,000/1000=25).
So if a meal is under 25g of fat? 1 pill. A meal under 50g (25×2)? 2 pills. 75g (25×3)? 3 pills. And so on. Once you know what a pill “covers”, it’s a little easier; you can simply assess whether a meal is above/below your pill size of 1 (25g), 2 (50g), 3 (75g) etc.
Round up if it’s in between, because you can’t divide a pill.
Example B: A Creon 36,000 “covers” 10 grams of fat if my ratio is 3,600 units of lipase for every gram of fat (36,000/3600=10).
So if a meal is under 10 grams of fat? 1 pill. 20 grams of fat is 2 pills (10×2); 30 grams of fat is 3 pills (10×3); etc.
—
When people with EPI share experiences online, they often describe their dose size (such as 1 x 25,000 or 3 x 36,000 like examples A and B above) for most meals, but the meal size and composition is rarely discussed.
Personally, I can eat pretty widely varying amounts of fat in each meal on a day to day basis.
That’s why, instead of a flat dosing that works for everything (because I would be taking a LOT of pills at every meal if I was trying to take enough to cover my highest fat meals every time), I have found it to be more effective to estimate each meal to determine my meal dosing.
Remember that meal estimates aren’t very precise. If you use a nutrition panel on a box serving, the serving size can vary a bit. Restaurants (especially chains) have nutrition information, but the serving size can vary. So recognize that if you are calculating or estimating 59 grams of fat and that means either 2 vs 3 pills or 6 vs 7 pills, that you should use your judgment on whether you want to round up to the next pill number – or not.
Let’s put the hypothetical meals side by side and compare dosing with examples A and B from above:
Using the previous meal examples with either 7 or 30 grams of fat:
With Example A (ratio of 25g of fat for every 1 pill, or 1000 units of lipase to cover 1 gram of fat), we would need 1 pill for the chicken meal and 2 for the chili meal. Why? The chili is >25 grams of fat which means we need to round up to 2 pills.
With Example B (ratio of 10 grams of fat for every 1 pill or 3600 units of lipase to cover 1 gram of fat), we would need 1 pill to cover the chicken (because it’s less than 10 grams of fat) and 3 – or more – pills for the chili. Why “or more”? Well, something like chili is likely to be imprecisely counted – and if you’re like me, you’d want a bit of extra cheese, so chances are I would round up to a 4th pill here to take in the imprecision of the measurements of the ingredients.
–
PERT Dosing for Protein
Wait, didn’t you say something about protein?
Yes, I did. Fat isn’t the only determinant in this math!
I do the same type of math with grams of protein and units of protease. (Remember, PERT has all 3 types of enzymes, even though it is labeled by the amount of lipase. You can look online or on the bottle label to see how much protease is in your PERT.)
For our examples, Zenpep 25,000 contains 85,000 units of protease. Creon 36,000 contains 114,000 units of protease.
For the meal that ‘worked’ of 30 grams of fat, we also want to know the protein that worked. For easy math, let’s also say 30 grams of protein is in this meal.
Following the same math as before:
Example A (Zenpep 25,000): 30 grams of protein divided by 1×85,000 units of protease is ~2,833 units of protease to every 1 gram of protein. Again, I like to think about how much 1 pill “covers” protein-wise. In this case, 1 Zenpep 25,000 “covers” 30 grams of protein.
Example B (Creon 36,000): 30 grams of protein divided into 3 x 114,000 units of protease is 11,400 units of protease per gram of protein. Again, I like to think about how much 1 pill “covers” protein-wise as well. In this case, 1 Creon 36,000 “covers” 10 grams of protein.
Here’s how many pills are needed for protein:
With Example A (ratio of 30g of protein for every 1 pill), we would need 1 pill for the chicken meal and 2 for the chili meal. Why? The chili is 42, which is greater than (30×1) grams of protein which means we need to round up to 2 pills.
With Example B (ratio of 10 grams of protein for every 1 pill), we would need 3 or more pills to cover the chicken. Why 3 or more? Again, it’s on the top edge of what 3 pills would cover, so I’d be likely to round up to 4 pills here. For the chili, 5 pills are needed (42 is more than 4 x 10 and is less than 5 x 10).
So how do you decide the number of pills to take for these meals? Let’s go back to our two example meals and compare the amount needed, pill-wise, for both fat and protein for each meal and each example.
When the pill numbers MATCH (e.g. the same number needed for fat and protein), which is the case for both examples with Zenpep 25,000, it’s easy: take that number of pills total! For Zenpep 25,000, I would take 1 pill for the Chicken (1 fat | 1 protein); and I would take 2 pills for the Chili (2 fat | 2 protein). Remember that PERT pills contain all three enzymes, so the fat and protein are sufficiently *each* covered by the quantities of lipase and protease in this pill type.
When the pill numbers are DIFFERENT between your fat and protein estimates, you use the LARGER number of pills. For Creon 36,000, with the chicken meal the protein quantity is much larger than the fat quantity; I would in this case dose 4 total pills (1 fat | 4 protein), which would then cover the protein in this meal and would also sufficiently cover the amount of fat in this meal. For the chili meal, it is closer: I estimated needing 4 pills for fat and 5 for protein; in this case, I would take 5 total pills which would then successfully cover the protein and the fat in the meal.
If you find the math challenging to do, don’t worry: once you determine your ratios and figure out how much one pill “covers”, it gets a lot easier.
(The calculator is for entering one meal at a time, and doesn’t save them, but if you’d like AI to estimate what is in your meal and help you log and save multiple meals, check out PERT Pilot if you have an iPhone or an Android phone.)
Here’s what it looks like using the two examples above:
You can input your meal that “works”, what your dose is that “works” (the number of pills and pill type), and it will share what your ratios are and what one pill “covers”.
You can also use the second part of the calculator to estimate the amount you need for a future meal! Say it’s coming up on a holiday and you’re going to eat a much larger meal than you normally do.
You can input into the calculator that you’ll be eating 90 grams of fat and 75 grams of protein.
Here’s the example with our dose from Example A (Zenpep 25,000):
Here’s the example large meal with our dose from Example B (Creon 36,000):
You can also hit the button to expand the calculations to see the math it is doing, and how it compares between the fat and protein pill estimates to see what “drives” the total number of pills needed.
You can even download a PDF with this math to have on hand. Here’s what the PDF download looks like for Example B (Creon 36,000):
–
Switching dose sizes or PERT brand types
This calculator can also be useful if you were originally prescribed a smaller quantity of PERT (e.g. Creon 3000 or Zenpep 3000) and you find yourself taking many numbers of these pills (6 or more) to cover a small meal for you, let alone more pills for a larger meal.
You can input this into the calculator and get your ratios; then in the second part, identify a different pill size, to see how many numbers of pills you’d take on a different dose.
You can also use it to help you understand how much you might need if you are switching between brands. Let’s say you were prescribed Zenpep 25,000 and you need to try Creon, either because you don’t think Zenpep works well for you or your insurance is more willing to cover the Creon brand.
You would use the top part of the calculator with your current brand and size (e.g. Zenpep 25,000 of which you take 6 for a standard meal of 30 grams of fat and 30 grams of protein) and then input the new brand and size and the same size meal (e.g. Creon 36,000 and another 30 grams of fat and 30 grams of protein meal) to see that you’d likely need 5 Creon 36,000 to match the 6 Zenpep 25,000 you were taking for a standard size (30 gram of fat and 30 gram of protein) meal.
Note: I’m not suggesting 30 grams of fat and protein at each meal is “standard” or the “right” size of the meal – I picked arbitrary numbers here to illustrate these examples, so make sure to include the meal that your PERT dosing successfully covers for YOU!
–
As a reminder, I’m not a doctor – I’m a person living with EPI. None of this is medical advice. I use this math and this calculator for my own personal use and share it in case it’s helpful to others. If you have questions, please do talk to your doctor. If you’re still experiencing symptoms with your enzyme dosing, you definitely should talk with your doctor. Your prescription size might need updating compared to what you were originally prescribed.
Also, please note that the calculator is open source; you can find the code here, and I welcome contributions (pull requests) and suggestions! You can leave feedback on Github or share feedback in this form. For example, if you’re using a different type of enzyme not listed in the calculator (currently 2/6 of the US FDA-approved versions are listed), please let me know and I can work to add the relevant list.

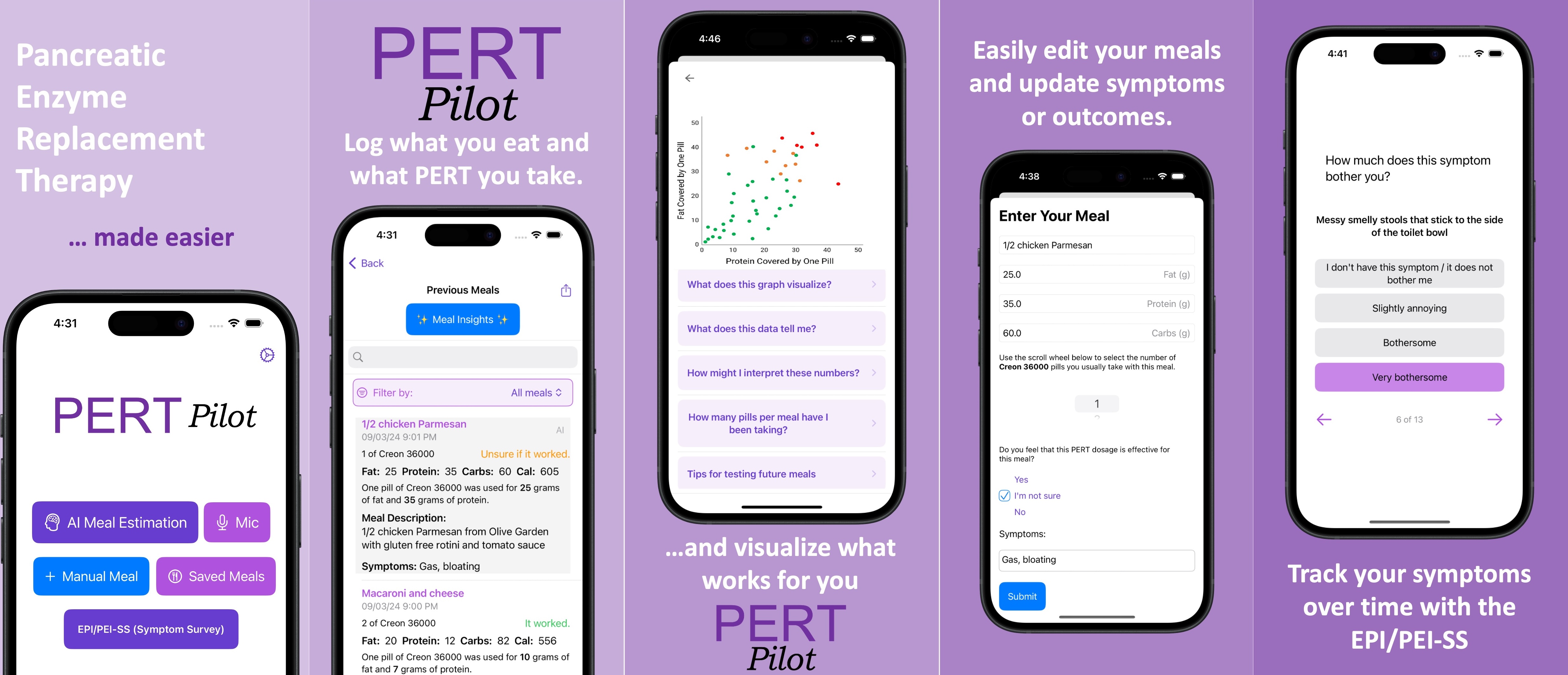
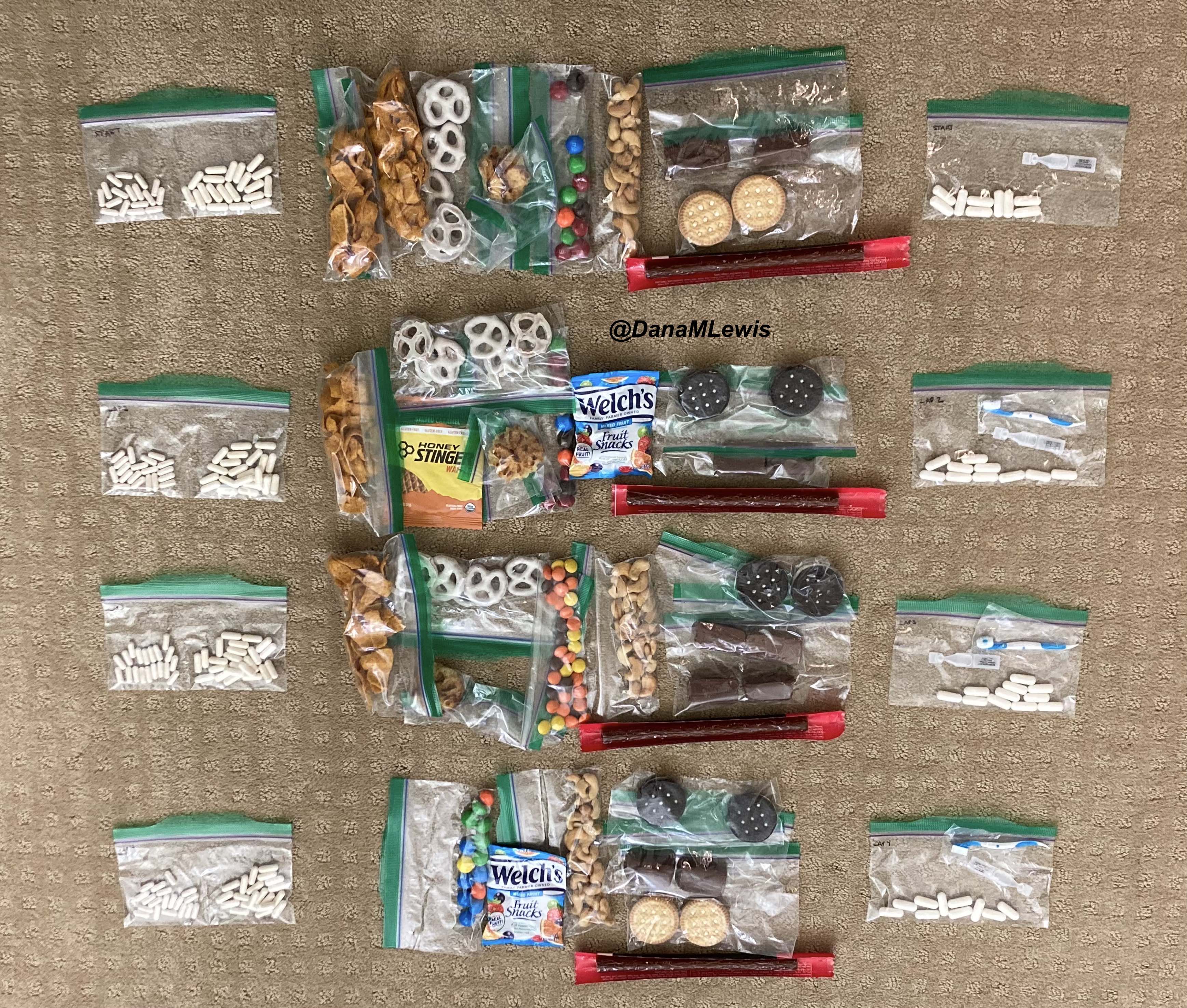
 I set out at 6am, It was 33 degrees (F), so I wore shorts and a short sleeve shirt, with a pair of fleece lined pants over my shorts and a long sleeve shirt, rain jacket, ear cover, and gloves on my hand. It was dry, which helped. I was the only one out on the trail in the dark, and I had a really bright waist lamp and was running on a paved trail, so I didn’t have issues seeing or running. I felt a bit chilly but within 3 minutes could tell I would be fine temperature wise. As I got on the trail, I glanced up and grinned – the stars were out! That meant I could “check” something off my experience list at the very start. (I make a list of positive and less great experiences to ‘check off’ mentally, everything from seeing the stars or seeing bunnies or other wildlife to things like blisters, chafing, or being cold or tired or having out of whack glucose levels – to help me process and “check them off” my list and move on after problem solving, rather than dwelling on them and getting myself into a negative mood). The other thing I chuckled about at the start was passing the point where, about a half mile in to
I set out at 6am, It was 33 degrees (F), so I wore shorts and a short sleeve shirt, with a pair of fleece lined pants over my shorts and a long sleeve shirt, rain jacket, ear cover, and gloves on my hand. It was dry, which helped. I was the only one out on the trail in the dark, and I had a really bright waist lamp and was running on a paved trail, so I didn’t have issues seeing or running. I felt a bit chilly but within 3 minutes could tell I would be fine temperature wise. As I got on the trail, I glanced up and grinned – the stars were out! That meant I could “check” something off my experience list at the very start. (I make a list of positive and less great experiences to ‘check off’ mentally, everything from seeing the stars or seeing bunnies or other wildlife to things like blisters, chafing, or being cold or tired or having out of whack glucose levels – to help me process and “check them off” my list and move on after problem solving, rather than dwelling on them and getting myself into a negative mood). The other thing I chuckled about at the start was passing the point where, about a half mile in to  As I continued my run/walk, just like I do in all my training runs, I pulled my enzymes out of my left pocket, swallowed them, put them away, grabbed my fuel out of my right pocket (starting with chili cheese Fritos), then also
As I continued my run/walk, just like I do in all my training runs, I pulled my enzymes out of my left pocket, swallowed them, put them away, grabbed my fuel out of my right pocket (starting with chili cheese Fritos), then also I was running well and a little ahead of my expected pace, closer to my usual long run/walk paces (which have been around 14:30-14:50 min/mi lately). I was concerned it was too fast and I would burn out as so many people do, but I did have wiggle room in my paces and had planned for an eventual slow down regardless. I made it to the first turnaround, used the trail bathroom there, and continued on, noting that even with the bathroom stop factored in, I was still on or ahead of schedule. I texted Scott to let him know to check my paces earlier than he might otherwise, and also stopped in my tracks to take a picture of a quail-like bird (which Scott thinks was a pheasant) that I’d never seen before. Lap 1 continued well, and I was feeling good and maintaining an overall sub-15 pace while I had been planning for a 15:10/ish average pace, so although Scott told me he didn’t need me to warn him about being particular miles away for aid station stops, I saw he was still at home by the time I was less than a mile out, and texted him. He was finishing a work call and had to rush to finish packing and come meet me. It wouldn’t have been a big deal if he had “missed” me at the expected turnaround spot, because there’s other benches and places where we could have met after that, but I think he was still stressed out (sorry!) about it, although I wasn’t. However, he biked up to me right at the turnaround spot, grabbed my vest and headed back to our normal table for refueling, while I used the bathroom and then headed out to meet him.
I was running well and a little ahead of my expected pace, closer to my usual long run/walk paces (which have been around 14:30-14:50 min/mi lately). I was concerned it was too fast and I would burn out as so many people do, but I did have wiggle room in my paces and had planned for an eventual slow down regardless. I made it to the first turnaround, used the trail bathroom there, and continued on, noting that even with the bathroom stop factored in, I was still on or ahead of schedule. I texted Scott to let him know to check my paces earlier than he might otherwise, and also stopped in my tracks to take a picture of a quail-like bird (which Scott thinks was a pheasant) that I’d never seen before. Lap 1 continued well, and I was feeling good and maintaining an overall sub-15 pace while I had been planning for a 15:10/ish average pace, so although Scott told me he didn’t need me to warn him about being particular miles away for aid station stops, I saw he was still at home by the time I was less than a mile out, and texted him. He was finishing a work call and had to rush to finish packing and come meet me. It wouldn’t have been a big deal if he had “missed” me at the expected turnaround spot, because there’s other benches and places where we could have met after that, but I think he was still stressed out (sorry!) about it, although I wasn’t. However, he biked up to me right at the turnaround spot, grabbed my vest and headed back to our normal table for refueling, while I used the bathroom and then headed out to meet him.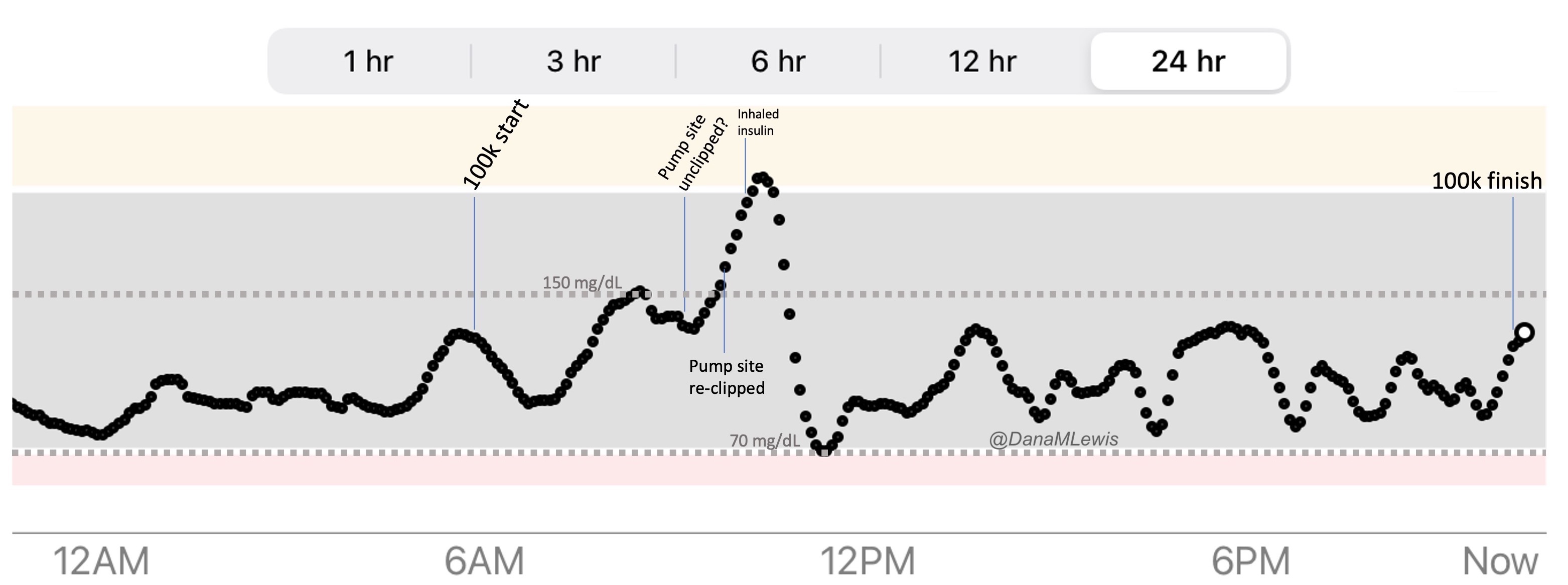

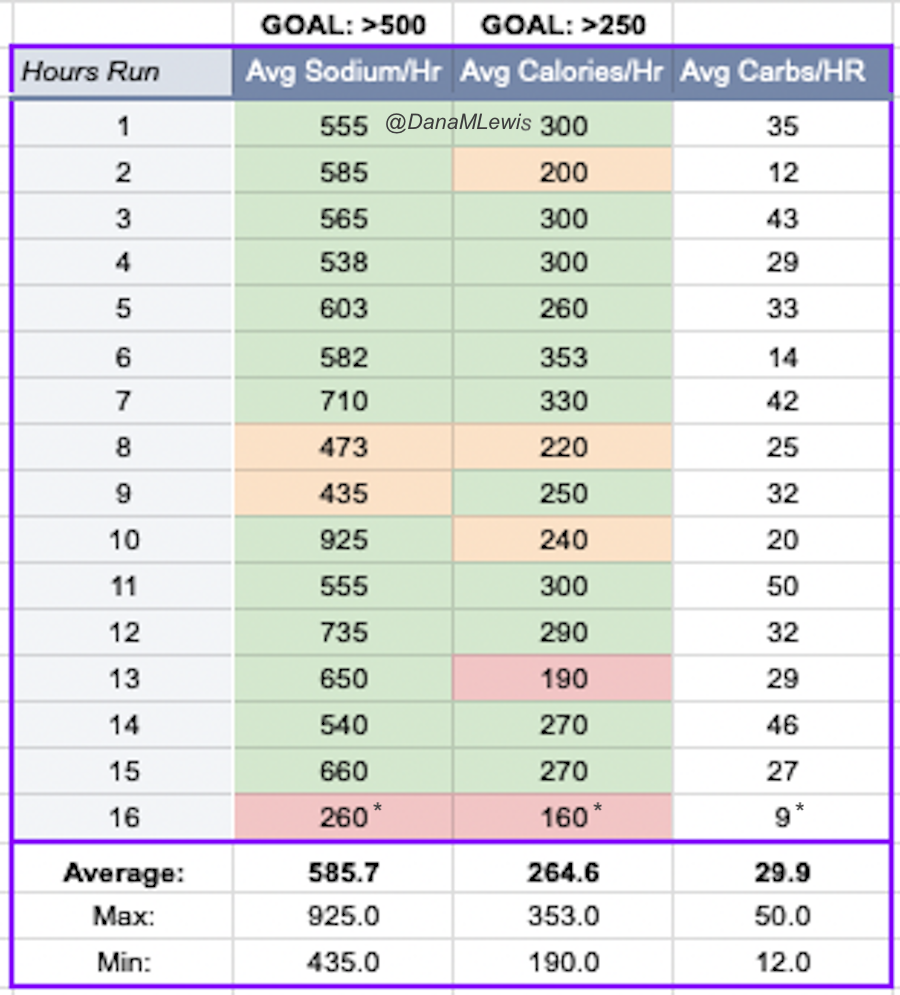 One of the things I do for all training runs but also races is
One of the things I do for all training runs but also races is 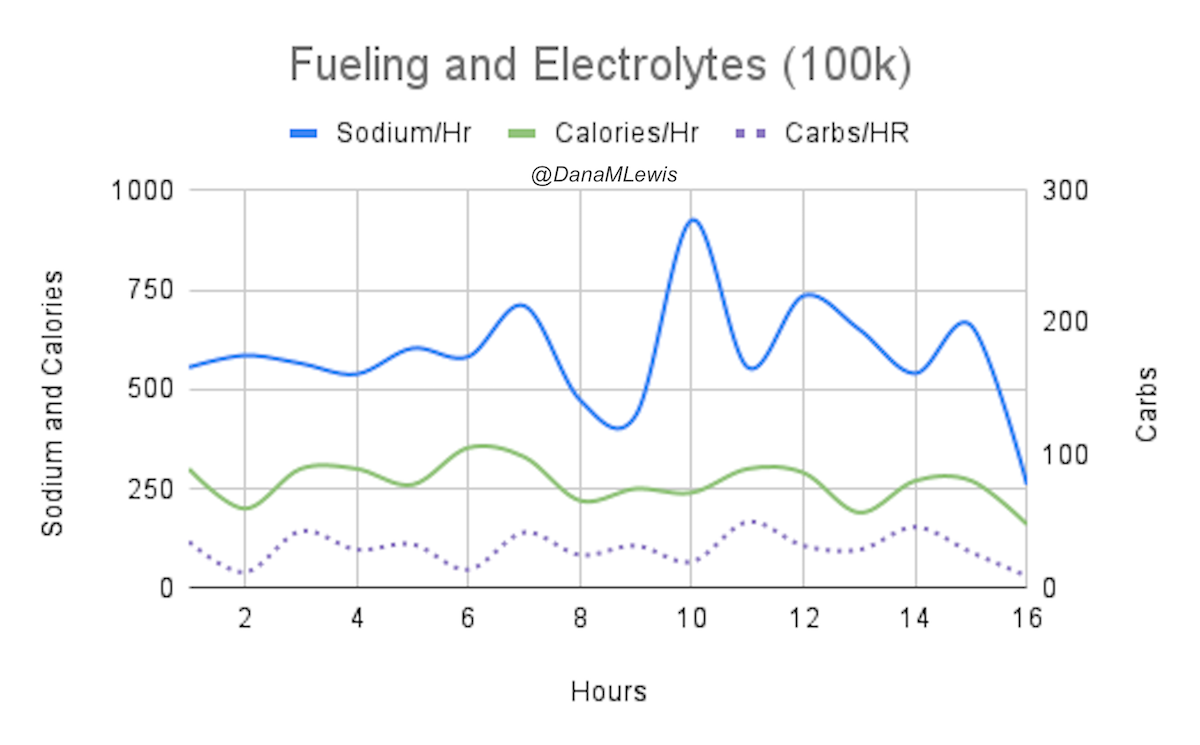
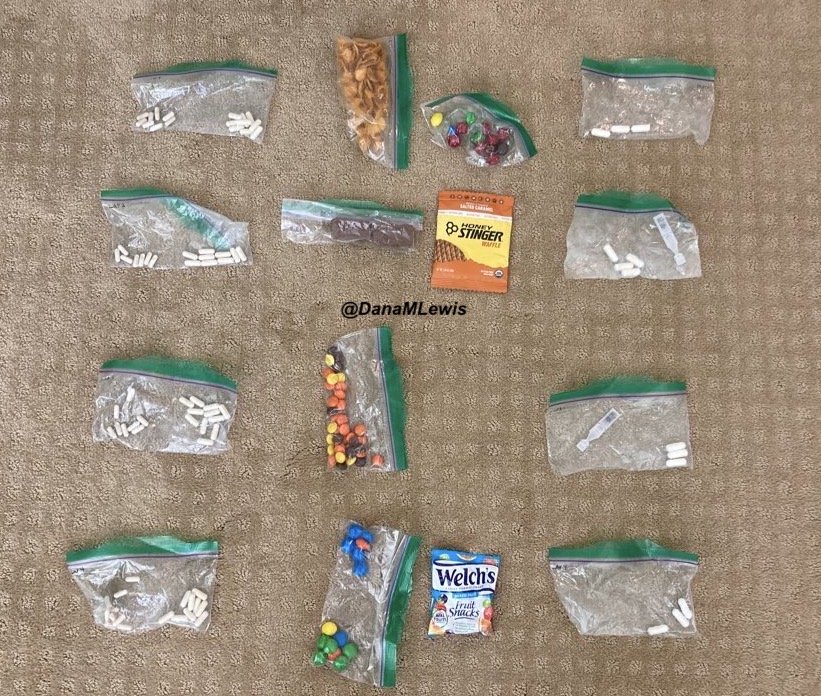
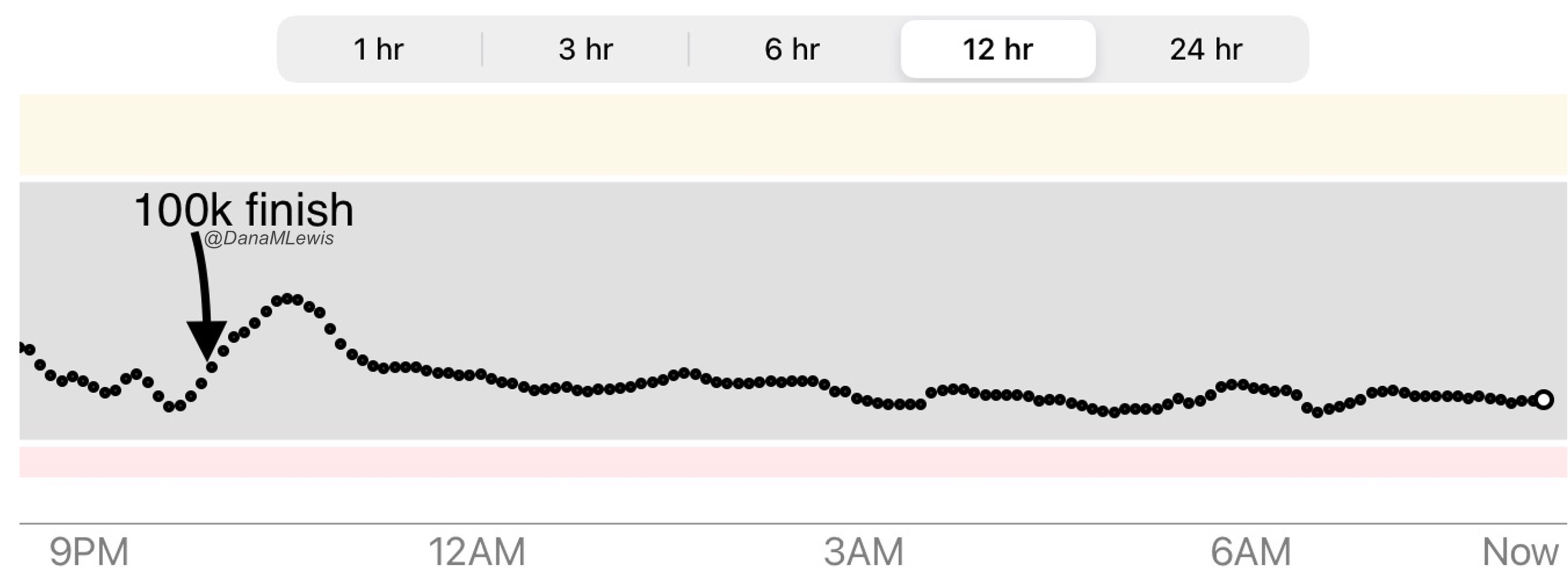



 )
)
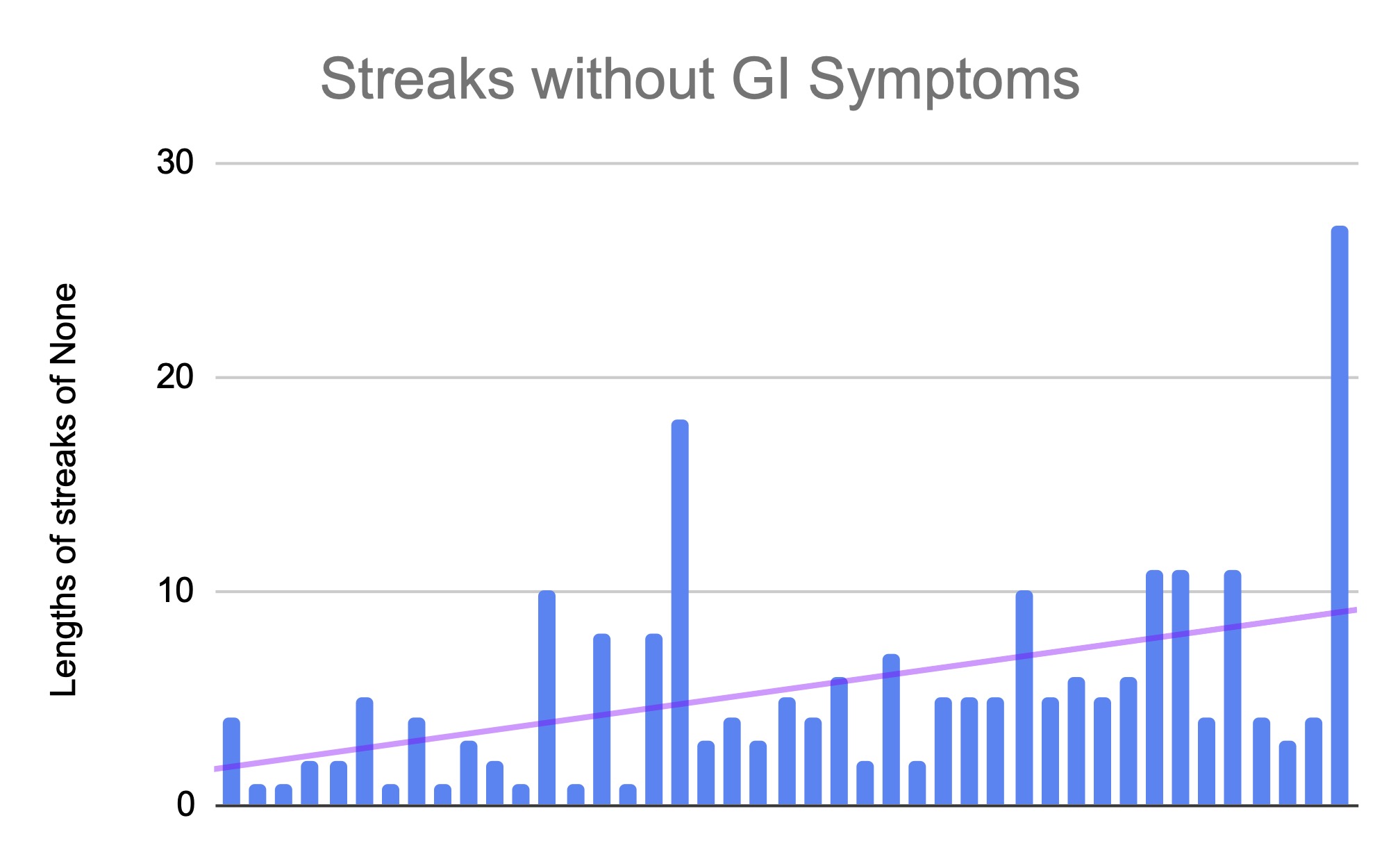
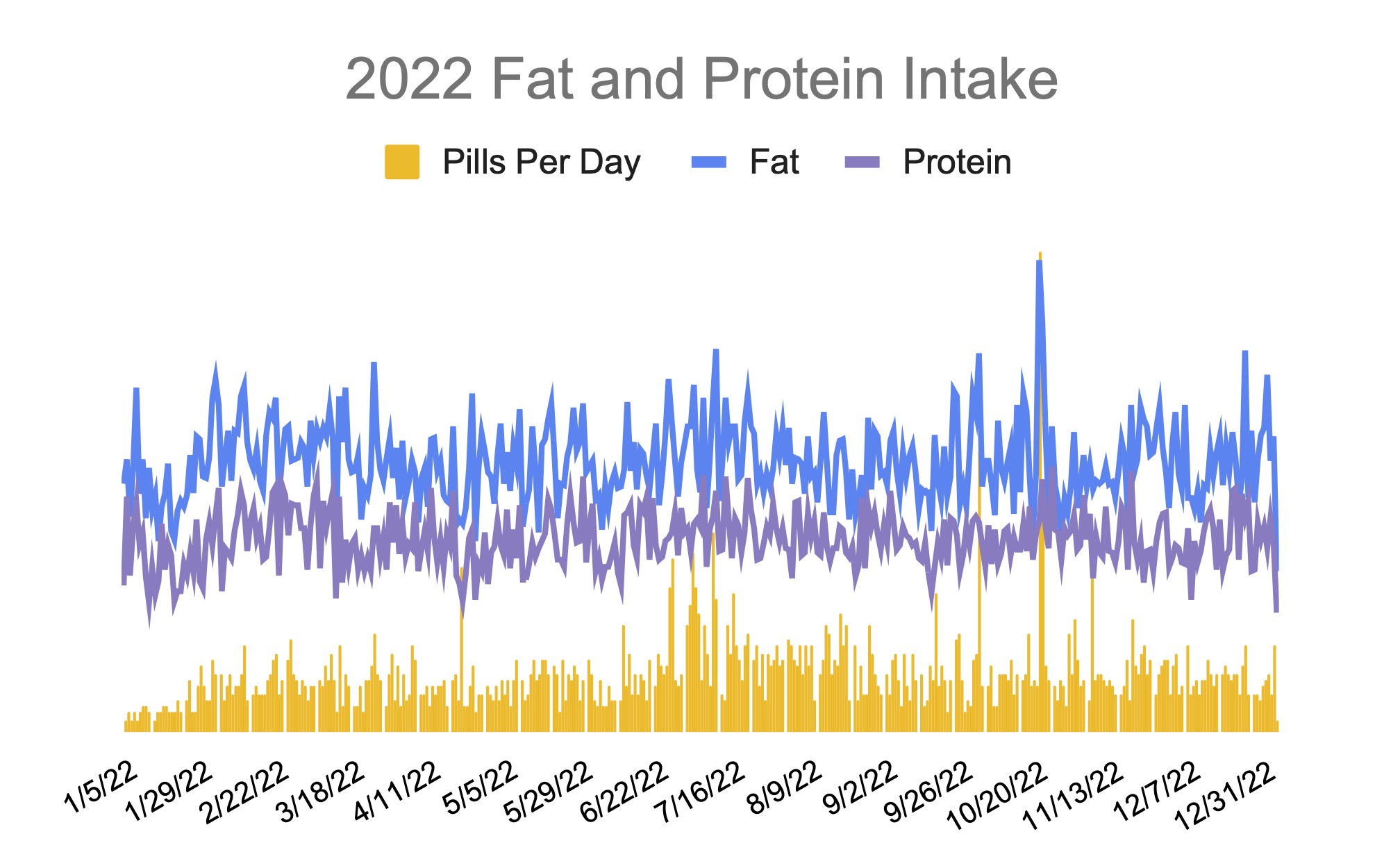
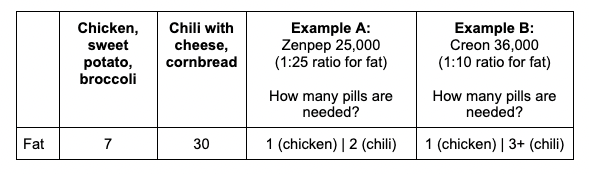
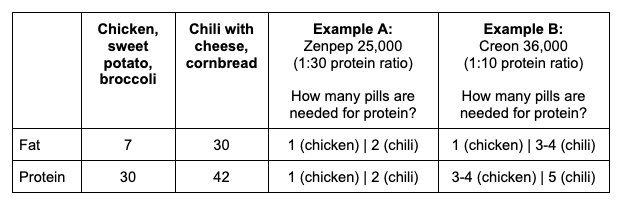
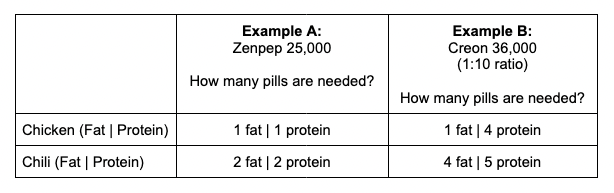
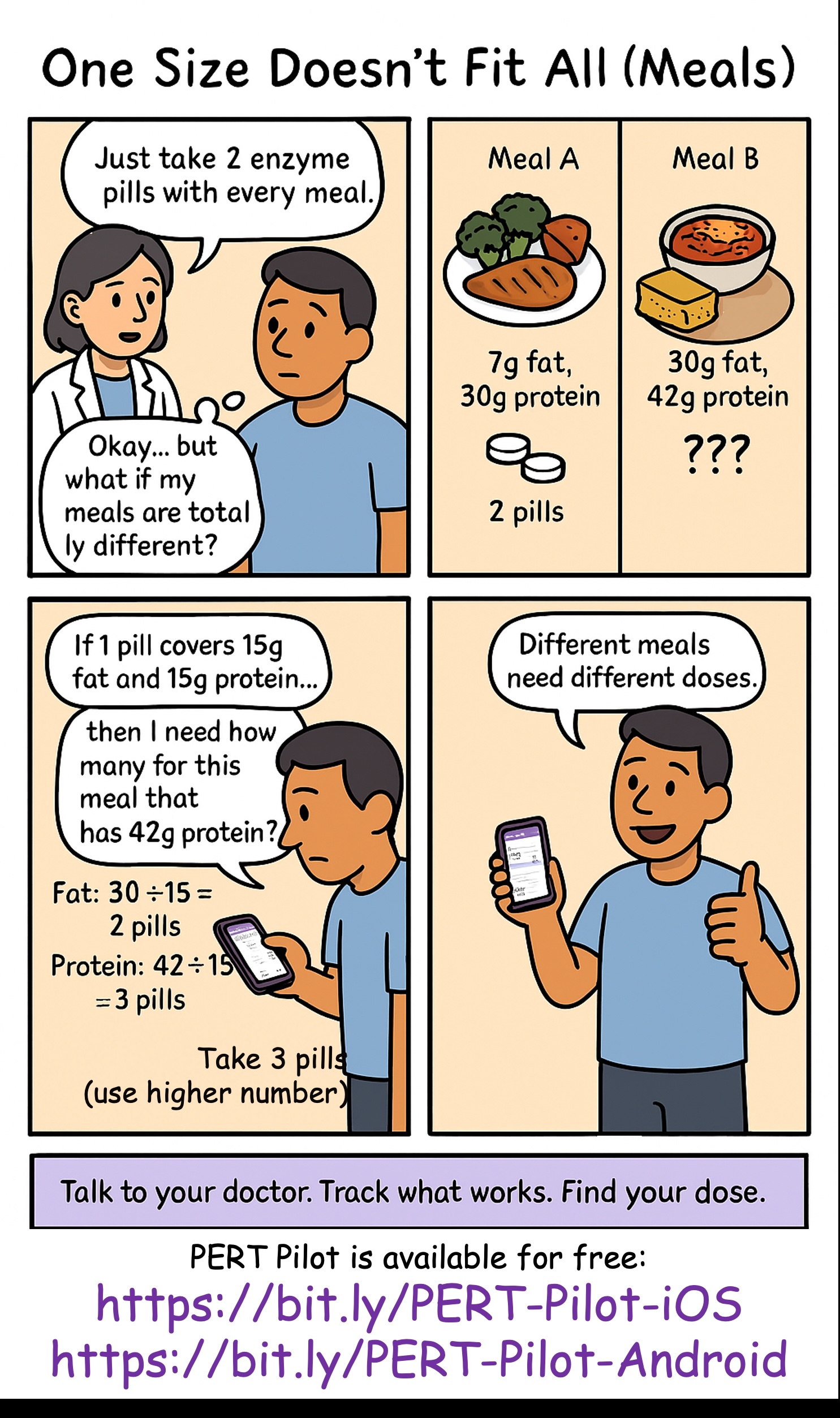
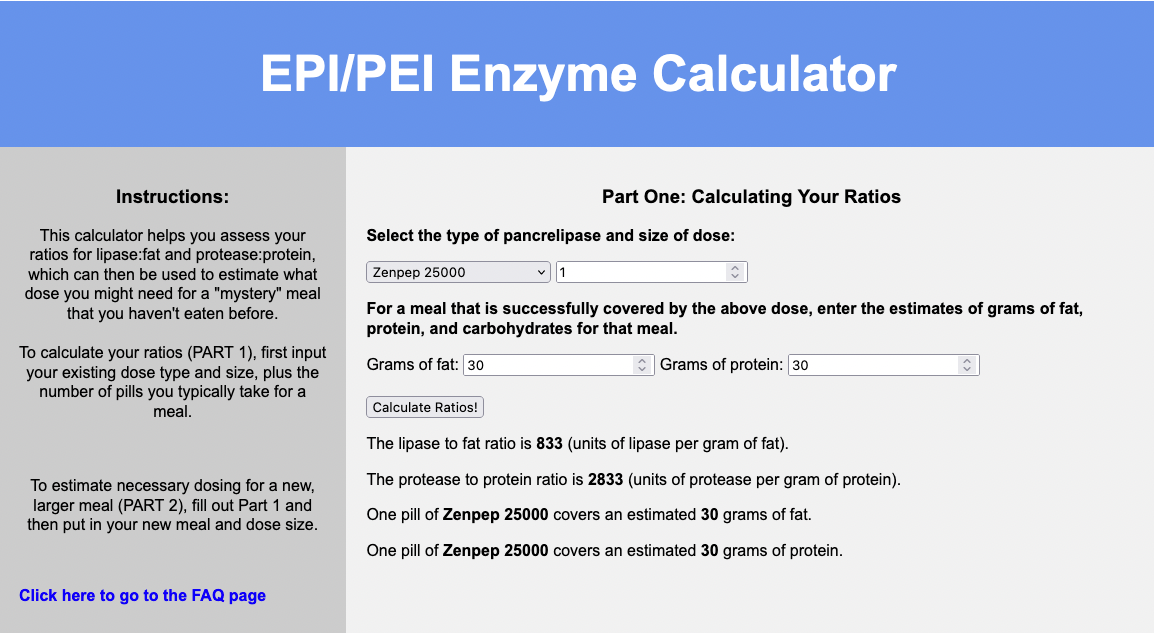

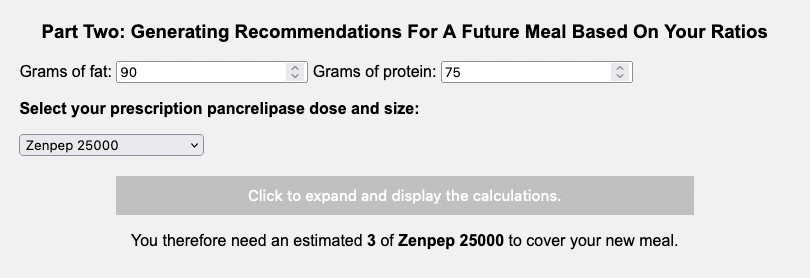
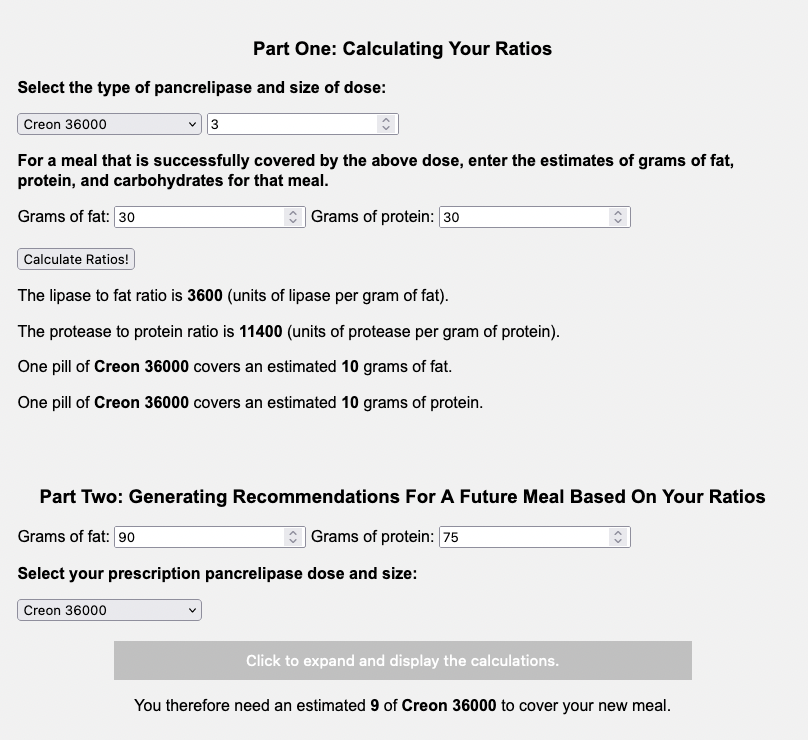
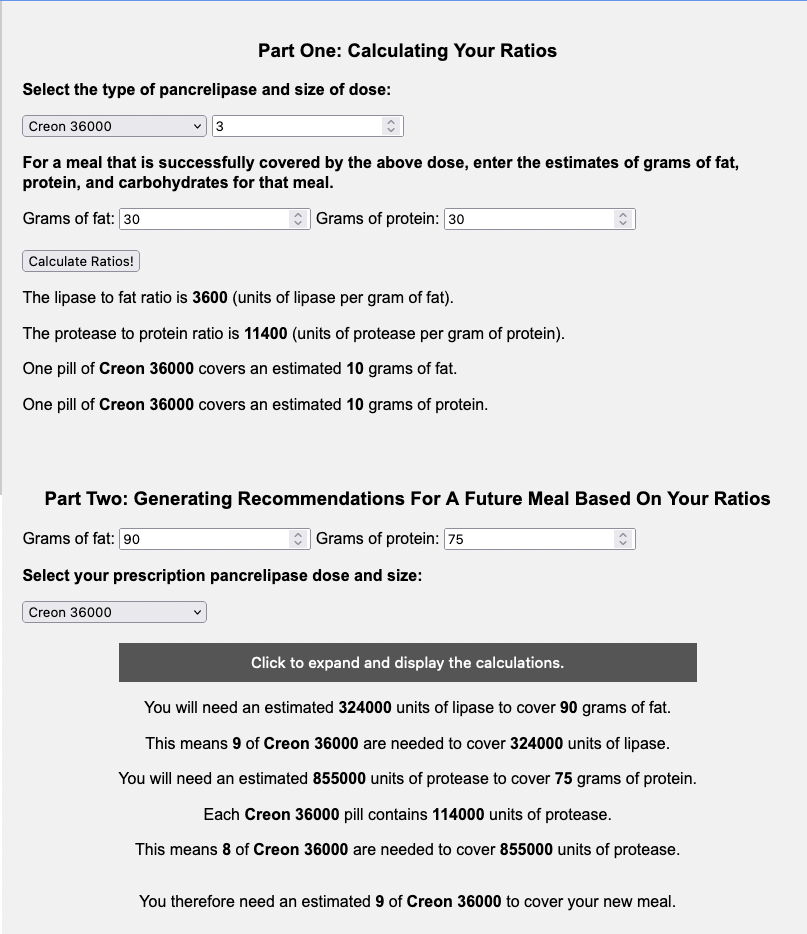
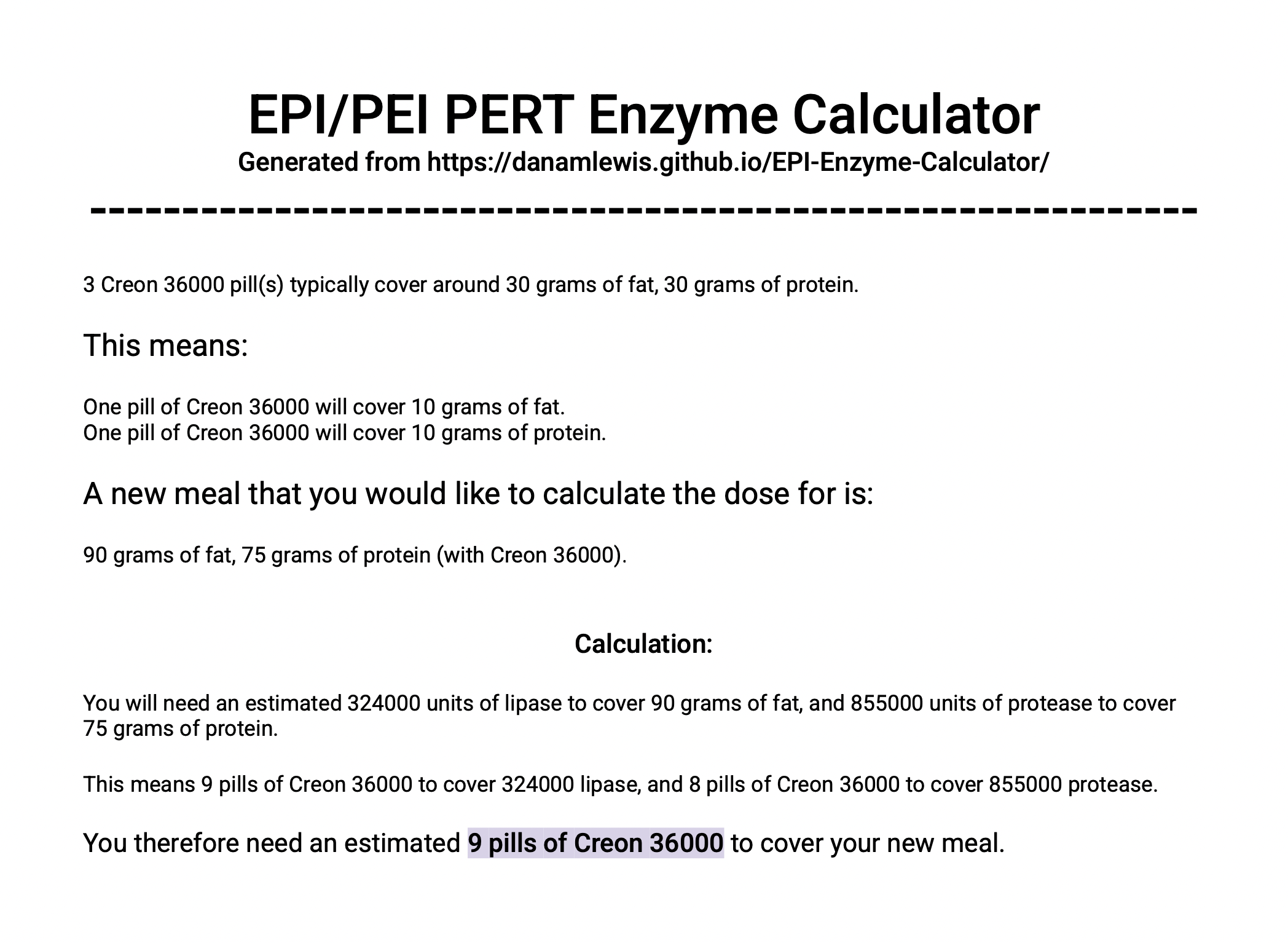
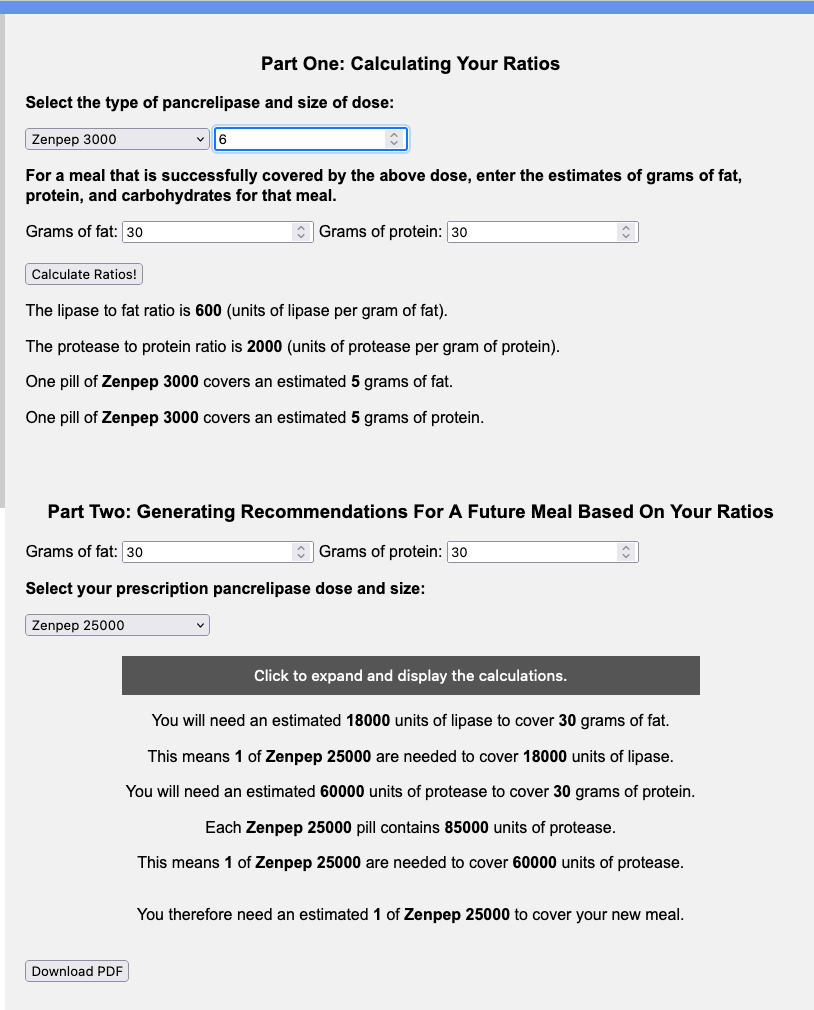
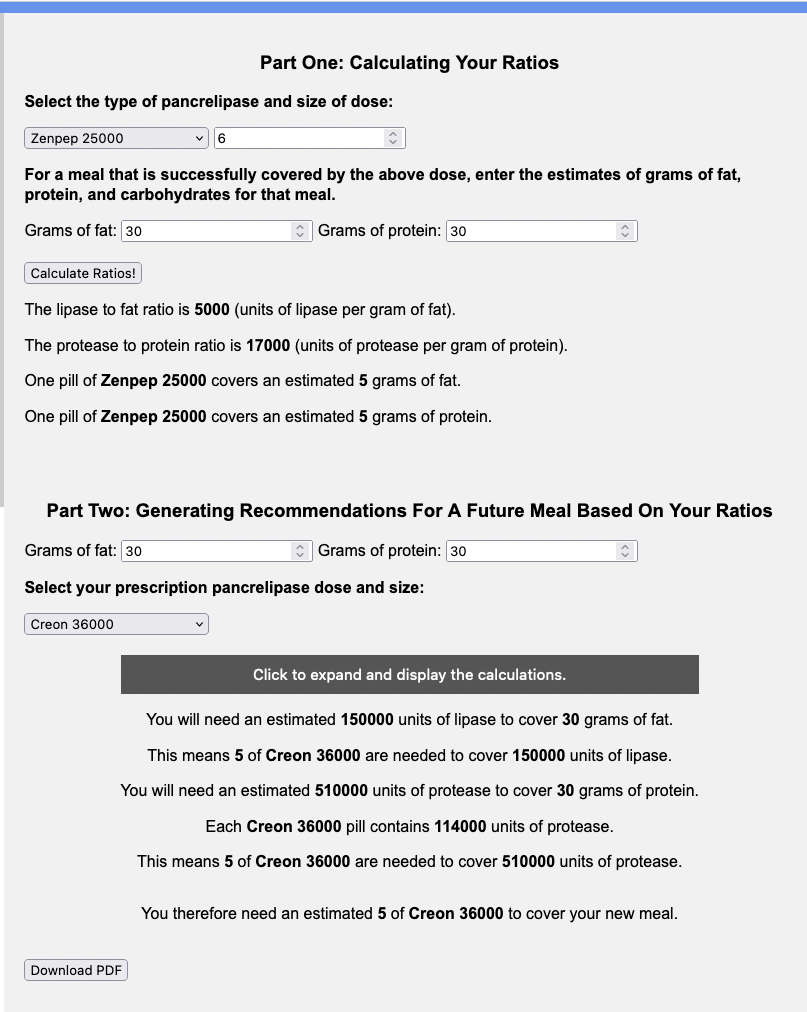
Recent Comments