A humorous side note – the title of this blog, DIYPS, stands for “do-it-yourself pancreas system”, the name I gave my first automated insulin delivery (AID) system, back in 2013. An AID system doesn’t fully replicate all functions of the pancreas, so we evolved from describing it as an artificial pancreas system (APS) to automated insulin delivery (AID). But now that I have exocrine pancreatic insufficiency and am doing quite a bit of DIY around titration of enzymes….the name of this blog feels more appropriate than ever.
After I started writing about exocrine pancreatic insufficiency, I’ve gotten a lot of questions from friends and connections who think they might have EPI. (And they are likely not wrong – there are estimates that as many as 40% of people with type 1 diabetes have lowered elastase levels. Alone, that doesn’t indicate EPI, but if symptomatic and you’ve already ruled out celiac and gastroparesis, it should be (in my opinion) high on the list of things to test for. Ditto for other types of diabetes and anyone with celiac disease.) Some people, though, may have delays in getting doctor’s appointments, and/or clinicians who aren’t (yet) willing to order the elastase or other EPI-related tests without testing for other things first.
This post is for that group of folks, and anyone stumbling across this post who has seen their test results for their fecal elastase testing indicating they have “moderate pancreatic insufficiency” or “severe pancreatic insufficiency” and are wondering what they can do while they wait for their doctor’s appointment.
It’s also for people with EPI who are struggling to afford their pancreatic enzyme replacement therapy (PERT) or are limiting the number or size of meals they eat as a result of the cost of PERT.
A bit of background on why I did the math about OTC enzyme cost and why I had tested them myself
Due to the holidays in December 2021 I had a lag between getting my test results (over Christmas) and then confirming that my doctor would write a prescription for PERT, and then a delay in getting it filled by the pharmacy since they had to order it. One of the things I did during that time was read up a lot about PERT and also look to see if there were any other kinds of enzymes that would be useful to take if my doctor didn’t want to prescribe me PERT. I found out that PERT contains THREE types of enzymes, and together they’re known as pancrelipase. Pancrelipase contains lipase (helps digest fat), protease (helps digest protein), and amylase (helps digest starches and other complex carbohydrates). It’s typically made from ground up pig pancreas, which is one of the reasons that PERT costs so much. Amylase from non-pancreatic sources is not widely available for human consumption, but there are some other ways to make protease and lipase. And it turns out that these standalone enzyme versions, often produced by microbes, are available to buy over the counter.
While waiting for my test to be ordered, I went ahead and ordered a standalone lipase product that is over the counter (OTC). In part, that was because some of the reviews for lipase talked about having EPI and how they were only sensitive to lipase, and so this was a viable and cheaper alternative for them rather than taking PERT with all 3 enzymes, since they didn’t need that. Based on my experience with FODMAPs and trying an enzyme powder to target fructans (which did help me some), it seemed like trying small doses of lipase would help if I did have EPI, and likely wouldn’t hurt even if I did not have EPI.
And it helped. It didn’t reduce all my symptoms, but even minor doses (3000 units of lipase) made a noticeable difference in my symptoms and I got a sense for what meals were more fat and protein-laden than others.
As a result, when my test results came in and I was on the borderline for moderate EPI, I agreed with my HCP that since it likely wouldn’t hurt to take PERT (other than the cost), and it would be obvious if it helped, that I should try PERT.
So having done the tests with OTC (over the counter) lipase was helpful for deciding to take PERT and advocating for my prescription.
And it turns out, wow yes, I do have EPI and do definitely need PERT (more about my first two weeks on PERT here).
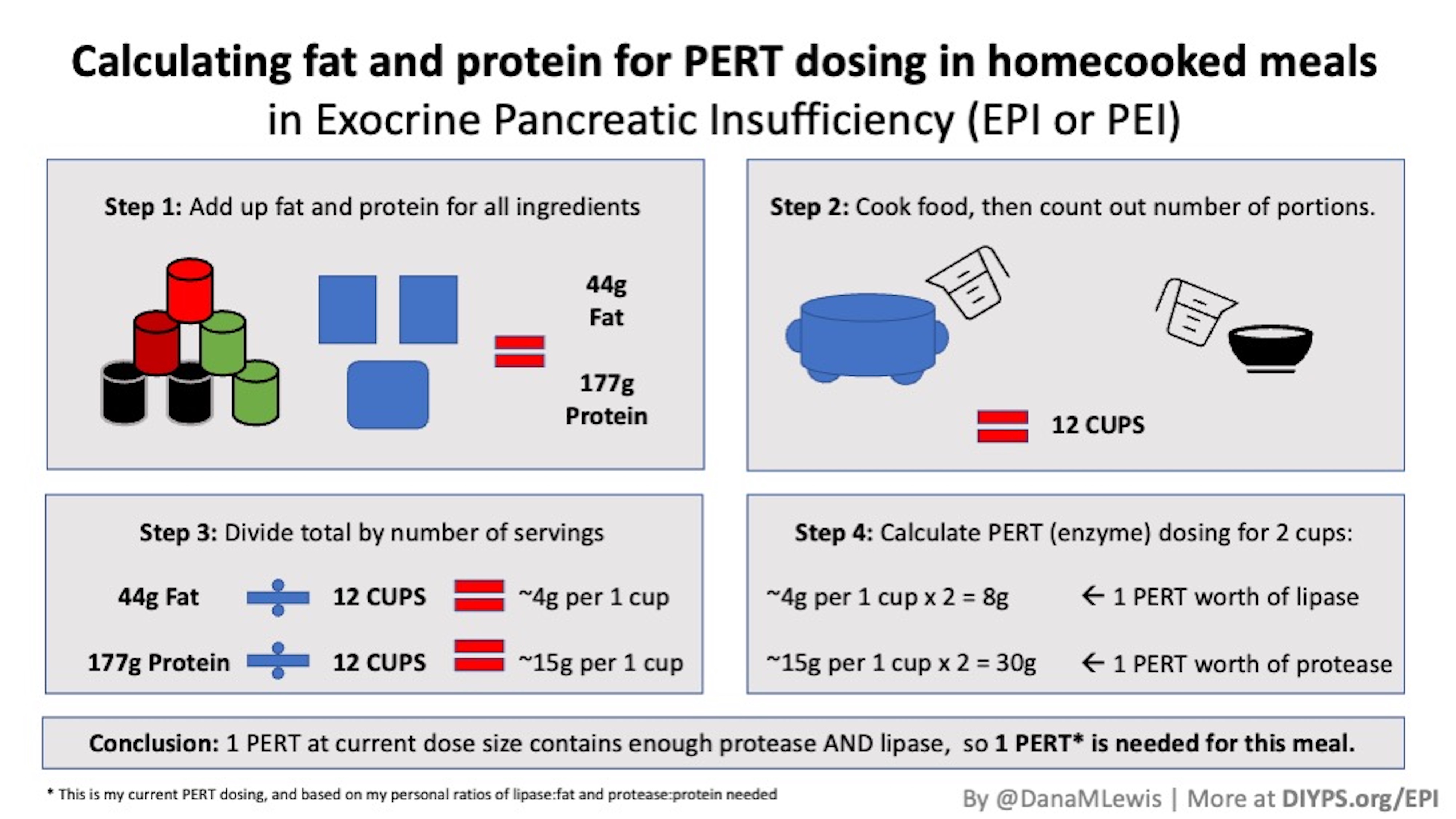
And as I wrote here, because I had the OTC lipase sitting around, even after I finally had access to PERT, I eventually titrated my dosing and calculated separate ratios for lipase:fat and protease:protein, so I can decide for every meal or snack whether I need one full PERT (all three enzymes), two PERT, a PERT plus some lipase (and how much), or just a standalone OTC lipase. The cost differs greatly between those options: one PERT might be $9 and a standalone lipase pill around $0.26. You can’t break apart a PERT (e.g. take only half), so adding a few lipase is a cost-effective approach if you don’t need more protease or amylase and the OTC lipase works for you.
Some of the reasons to explore over the counter enzymes with exocrine pancreatic insufficiency or a suspected case of EPI
One interesting thing about one of the main tests (fecal elastase) used to assess EPI is that it is NOT impacted by taking enzymes. Someone who is started on pancreatic enzyme replacement therapy (PERT) can still have an elastase test without stopping taking PERT. So if someone had an inconclusive result or was borderline and started taking PERT, but their doctor wanted to re-test again, the use of PERT would not affect the test. The same goes for other types of enzymes.
I’ve realized that the following groups of people might want to investigate various OTC enzyme options:
- Someone who has been diagnosed with EPI, but has done careful testing with meals of various sizes (low fat & high protein, high fat & low protein, etc.) to determine that they really only need lipase, may benefit from cheaper lipase-only OTC options.
- Someone who has a test result for EPI but doesn’t yet have an appointment with their doctor or a prescription for PERT could start taking some OTC enzymes for quicker symptom relief, even if they ultimately want to use PERT for all their enzyme needs once they get their prescription filled.
- Someone diagnosed with EPI who cannot afford the ideal dose of PERT that they need for their meals and snacks, may want to calculate the out of pocket costs for OTC lipase (not covered by insurance) vs the cost of PERT with or without insurance.
- Someone who can’t get tested for EPI, but suspects they have EPI, might want to also explore OTC lipase and/or OTC multiple enzyme products.
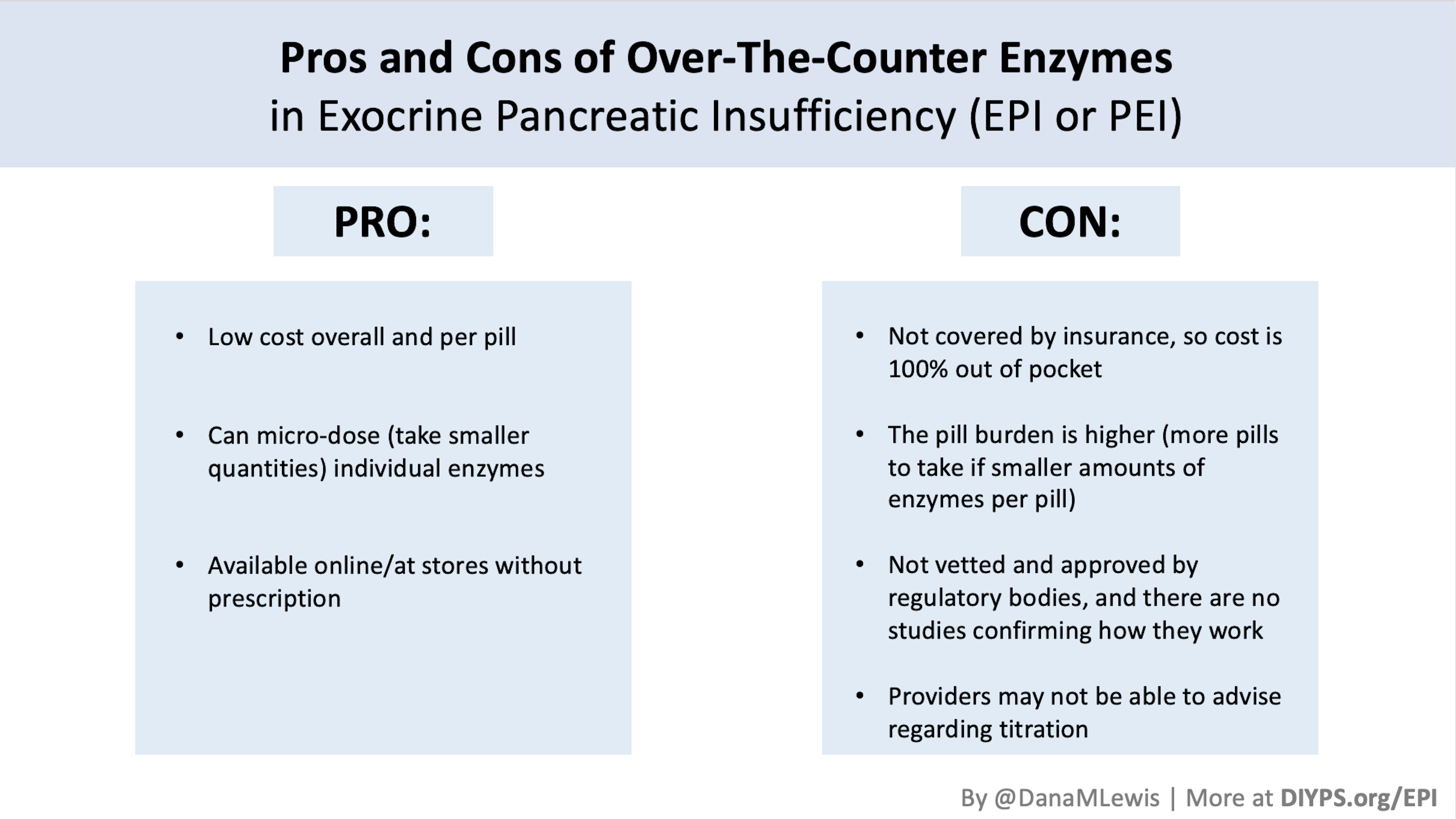
However, not everyone with EPI will want OTC enzymes. Some people may have great insurance coverage, so their PERT costs them less than $9 a pill. OTC enzymes are not covered by insurance, but I’d still do the math and assess what your standard cost is per pill, because it may surprise you how cheap add-on OTC lipase is vs. your insurance deductible or copay to take additional PERT for larger meals. The other reason some people may not want to take OTC enzymes is the pill burden: OTC doses tend to be smaller, so you usually need to take more pills to cover the same meal as a single, larger PERT.
Picking what enzymes (in general, or specific brands) work for you
I often see a variety of OTC enzyme products recommended in peer groups on social media for EPI. There are no studies that I can find assessing the efficacy of these OTC brands (meaning, how good they are). I would be very cautious when trying different single or multiple enzyme products and keep a careful log of your symptoms from before enzymes as well as symptoms at every meal that you take enzymes, and your bathroom results afterward. This can help you assess OTC enzymes as well as PERT if you get access to it. By having a good log of your symptoms, you can tell if you’re taking enough enzymes (OTC or PERT) or if you’re developing new symptoms (which could be a side effect of whatever brand/type you are taking).
There are multiple brands and sizes of PERT, too, and it’s possible that a filler product or how the PERT is made by one brand doesn’t work well for you. If that’s the case, you can try another brand of PERT.
The same goes for OTC enzymes: it is very possible some types of pills may be made with ingredients that could bother you and cause symptoms themselves. You should definitely be very cautious if you go this route and explore small doses and ensure no side effects (no new symptoms) before increasing any doses.
When I search for lipase, it’s easy to find standalone lipase (here is an example, as an Amazon affiliate link). When I search for protease, it’s more common to find products that are multiple enzymes (e.g. lipase AND protease AND other random things that are “good for digestion”). Personally, I’m very wary of anything OTC that’s described as “digestive enzymes” with additional ingredients and prefer to stick to products that only have the ingredients I’m looking for (lipase, protease, and amylase only).
—
The amount of enzyme also matters
The amount of enzyme you take matters, which is probably the second place that people trip up and make mistakes when trialing over the counter (OTC) enzymes. For example, the starting dose recommended for people with EPI is 40,000-50,000 units of lipase. Some of the most common OTC pills have 4-6,000 units of lipase: that means taking 10 OR MORE PILLS per meal in order to get the starting dose. Could you do that? Absolutely. (10 x $0.26 means that is around $2.60 cost, which may still be cheaper than the prescription pills.) However, the burden of consuming that many pills is pretty high in the long run. But you might be ok with that in the short run. There are other OTC options like this one (which I do use myself) that has around ~17,000 units of lipase. They are more expensive per pill, but you have to take fewer (e.g. 3-4 pills per meal) to match the starting dose.
For a lot more info on dosing, read this post about the starting dose and how most people end up needing MORE enzyme than this amount. Then read this post about how to figure out how much enzymes you may need to adjust to the food you’re eating and end up with an optimal dose. (You can also use PERT Pilot to help you with that).
That’s an advanced step, though, so if you’re just getting started I would focus on getting the minimum starting dose (equivalent to 40-50,000 units of lipase per meal) and see how that goes, then titrate (increase) from there.
—
In diabetes, we often say “your diabetes may vary” (YDMV), indicating that different people can have different experiences.
In EPI, it’s no different – “your digestion may vary” and it’s important to test and record and find what works for you, and to find a balance of reducing or eliminating symptoms with enzymes in a cost-effective way that you can afford.
—
(PS, if you didn’t see them, I have other posts about EPI at DIYPS.org/EPI – including one about PERT Pilot, the first iOS app for Exocrine Pancreatic Insufficiency! It’s an iOS app that allows you to record as many meals as you want, the PERT dosing and outcomes, to help you visualize and review more of your PERT dosing data!)
—
You can also contribute to a research study and help us learn more about EPI/PEI – take this anonymous survey to share your experiences with EPI-related symptoms!
—
Recent Comments