Why is everything a titration problem; why does the traditional healthcare / research system not solve titration for so many therapies; and why do I always find myself having to do it?
Good questions that I won’t answer (because I can’t), but it is a good introduction into what I have been working on. I built a titration simulation tool for clinicians and people who want to explore different adjustments to dosing immunoglobulin, especially through subcutaneous methods. AKA, subcutaneous IG, AKA ScIG (rhymes with “rig”).
What exactly is the problem?
ScIG is studied in very few conditions – the approved FDA indications are generally for PI (primary immunodeficiency) and CIDP (chronic inflammatory demyelinating polyneuropathy). But, ScIG (and IVIG) are used to treat a lot of autoimmune conditions (often used off-label, because the few other conditions studied have a much smaller population studied and lower-quality evidence bases). Thus, there are no approval studies nor good data for these other condition use cases. Instead, there is a smattering of literature showing that occasionally it works here and there. The dosing regimens are based on the PI/CIDP studies and there are very few of those studies beyond product-specific studies. ScIG has mostly been tested at a 7 day interval (meaning once per week) and there’s one study checking to see if you do it every 14 days (every two weeks) but double the dose to maintain the total dose per month, you get about the same outcome…that is, in people with PI, which means they were measuring infections. That doesn’t answer the “does it work” question for most other use cases for ScIG, which is a variety of other autoimmune diseases. It also doesn’t appear that they tested lower doses (?), so we can’t tell if the same dose over 14 days was effective because they doubled the weekly dose for the 14 day regimen they studied.
But does it work well if you do the same dose every 9-10 days? No one can tell you that, it hasn’t been studied, so if a patient is struggling with every 7 days scheduling, they may benefit from a schedule change, but there’s no data or guidance from research for the clinician to help estimate whether that may be ok, or a problem. Or, what happens if you slightly drop your dose by 10mL? Or what happens if you split your dose across 14 days? What happens if your dosing is evenly split over time or very differently split based on the pre-filled cartridges you have available?
Clinicians don’t often seem to prescribe ScIG to very many patients, so they also don’t have a strong feedback loop of data on alternative dosing regimens. And most indications are off-label and diverse, so that further dilutes that data stream: what works for someone could be unique to their disease rather than useful to extrapolate to everyone on ScIG.
Why does this matter?
ScIG is dosed based on body size. If you have a larger body, you have a larger dose. You are limited to how much you can infuse per site which influences how many needles you use. Needles have a risk of causing bruises and lumps (resolving to small clots of tissue that can sometimes take weeks to months to go away), so in some cases fewer needles is ideal, but this then drives up the size of the fluid depot which can be painful due to skin stretching and the amount of fluid that has to be cleared. It is a tradeoff between all of these factors. And, over time, people may have less skin real estate for various reasons. But, there’s no tool that helps patients make this kind of tradeoff. Current dosing calculators can help with dose and volume and figuring out infusion times, and tracking apps can record what happened, but they usually do not show what different schedules might mean over time. For example, whether doing smaller amounts less often changes the overall amount dosed, whether this creates bigger highs and lows in IgG levels, or simply reduces the number of sites. There’s also the question of how much time it takes for these varied dose schedules given the tradeoffs where fewer needles means larger depots and slower infusion times.
I wanted a tool to make those trade-offs easier to see. I wanted to be able to compare possible schedules side by side, showing the expected pattern over time, the amount per week, the number of infusion sites, the volume per site, and also model what the impacts are for the IG itself.
ScIG Pilot
ScIG dosing decisions often involve trade-offs among dose interval, total dose intensity, infusion volume, number of sites, per-site volume, and patient tolerability, but existing product calculators don’t cover this. They generally are designed for clinicians or pharmacists and focus on narrow tasks such as converting weight-based dose to volume, estimating sites or infusion time, or supporting labeled weekly/biweekly schedules. Published PK models describe ScIG absorption, peak/trough behavior, and exposure under standard regimens, but these are not available as a practical tool for comparing based on real-world constraints.
ScIG Pilot is a literature-informed simulator that compares candidate ScIG schedules against a reference regimen (aka a standard 7-day dosing schedule), showing normalized exposure curves, predicted peak/trough patterns, weekly-equivalent dose intensity, site burden, dose volume per site, and infusion frequency. (It is also open source.)
It can help someone think through a scenario and ask these types of questions of a proposed change:
- If I change the schedule, how does this change the volume I am getting over time? How does this compare to the existing schedule?
- When might this dose change impact the body?
- What is the burden trade-off: sites, dose per site, infusion days, time per infusion, longest gap? How does this stack up over a month or a year?
Then, based on outcomes (does it work) and various preferences (less time; fewer sites; smaller fluid depots; etc), someone can decide what works for their scenario, or at least have visuals to help them think through a decision and understand various tradeoffs. This is also helpful when trying to estimate out to longer time frames, for example: not just what this regimen does in a month in terms of number of sites, number of infusion days etc; but also how does this translate to a year of this therapy in terms of number of infusions and sites, etc?
–
 It can be really hard to titrate these types of therapies and infusions, because there is no good data. I’d love to see studies in future collect this type of data or have repositories (like I described here) that are not limited to one disease indication, so a patient or clinician could go and research across populations to better get some data to triangulate from to better inform a subsequent decision to go on a therapy or change a treatment regimen. Right now, there are no visuals, no data, and no tools. But now, for this, there is at least ScIG Pilot to help visualize and triangulate across what little data we do have.
It can be really hard to titrate these types of therapies and infusions, because there is no good data. I’d love to see studies in future collect this type of data or have repositories (like I described here) that are not limited to one disease indication, so a patient or clinician could go and research across populations to better get some data to triangulate from to better inform a subsequent decision to go on a therapy or change a treatment regimen. Right now, there are no visuals, no data, and no tools. But now, for this, there is at least ScIG Pilot to help visualize and triangulate across what little data we do have.
(And it’s open source so if you have ideas to improve ScIG Pilot or suggestions to make the models more useful, please feel free to open issues or PRs or email me to discuss – Dana+ScIGPilot@OpenAPS.org)
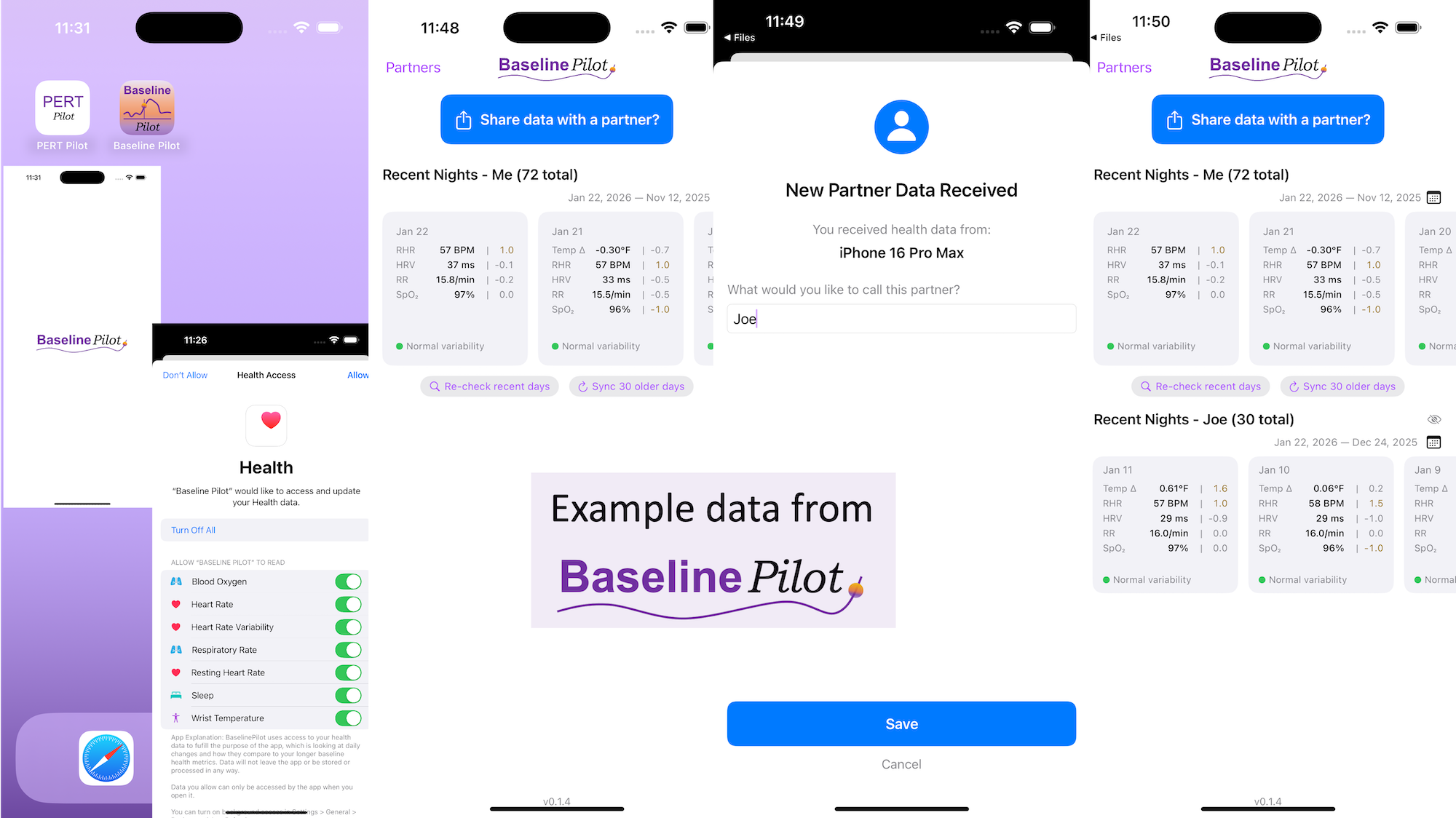
 All of this data is local to the app and not being shared via a server or anywhere else. It makes it quick and easy to see this data and easier to spot changes from your normal, for whatever normal is for you. It makes it easy to share with a designated person who you might be interacting with regularly in person or living with, to make it easier to facilitate interventions as needed with major deviations. In general, I am a big fan of being able to see my data and the deviations from baseline for all kinds of reasons. It helps me understand my recovery status from big endurance activities and see when I’ve returned to baseline from that, too. Plus the spotting of infections earlier and preventing spread, so fewer people get sick during infection season. There’s all kinds of reasons someone might use this, either to quickly see their own data (the Vitals access problem) or being able to share it with someone else, and I love how it’s becoming easier and easier to whip up custom software to solve these data access or display ‘problems’ rather than just stewing about how the standard design is blocking us from solving these issues!
All of this data is local to the app and not being shared via a server or anywhere else. It makes it quick and easy to see this data and easier to spot changes from your normal, for whatever normal is for you. It makes it easy to share with a designated person who you might be interacting with regularly in person or living with, to make it easier to facilitate interventions as needed with major deviations. In general, I am a big fan of being able to see my data and the deviations from baseline for all kinds of reasons. It helps me understand my recovery status from big endurance activities and see when I’ve returned to baseline from that, too. Plus the spotting of infections earlier and preventing spread, so fewer people get sick during infection season. There’s all kinds of reasons someone might use this, either to quickly see their own data (the Vitals access problem) or being able to share it with someone else, and I love how it’s becoming easier and easier to whip up custom software to solve these data access or display ‘problems’ rather than just stewing about how the standard design is blocking us from solving these issues! These are actionable, doable, practical things we can all be doing, today, and not just gnashing our teeth. The sooner we course correct with improved data availability, the better off we’ll all be in the future, whether that’s tomorrow with better clinical care or in years with AI-facilitated diagnoses, treatments, and cures.
These are actionable, doable, practical things we can all be doing, today, and not just gnashing our teeth. The sooner we course correct with improved data availability, the better off we’ll all be in the future, whether that’s tomorrow with better clinical care or in years with AI-facilitated diagnoses, treatments, and cures.  (Thank you).
(Thank you). TL;DR: Instead of arbitrarily lowering or increasing fat or fiber in the diet, measure and estimate what you are consuming first. If you have EPI,
TL;DR: Instead of arbitrarily lowering or increasing fat or fiber in the diet, measure and estimate what you are consuming first. If you have EPI,  If you can shift your mindset from fear and avoidance to curiosity and experimentation, you might discover new skills, solve problems you once thought were impossible, and open up entirely new opportunities.
If you can shift your mindset from fear and avoidance to curiosity and experimentation, you might discover new skills, solve problems you once thought were impossible, and open up entirely new opportunities.
Recent Comments