If I had a nickel every time I saw conflicting advice for people with EPI, I could buy (more) pancreatic enzyme replacement therapy. (PERT is expensive, so it’s significant that there’s so much conflicting advice).
One rule of thumb I find handy is to pause any time I see the words “too much” or “too little”.
This comes up in a lot of categories. For example, someone saying not to eat “too much” fat or fiber, and that a low-fat diet is better. The first part of the sentence should warrant a pause (red flag words – “too much”), and that should put a lot of skepticism on any advice that follows.
Specifically on the “low fat diet” – this is not true. A lot of outdated advice about EPI comes from historical research that no longer reflects modern treatment. In the past, low-fat diets were recommended because early enzyme formulations were not encapsulated or as effective, so people in the 1990s struggled to digest fat because the enzymes weren’t correctly working at the right time in their body. The “bandaid” fix was to eat less fat. Now that enzyme formulations are significantly improved (starting in the early 2000s, enzymes are now encapsulated so they get to the right place in our digestive system at the right time to work on the food we eat or drink), medical experts no longer recommend low-fat diets. Instead, people should eat a regular diet and adjust their enzyme intake accordingly to match that food intake, rather than the other way around (source: see section 4.6).
Think replacement of enzymes, rather than restriction of dietary intake: the “R” in PERT literally stands for replacement!
If you’re reading advice as a person with EPI (PEI), you need to have math in the back of your mind. (Sorry if you don’t like math, I’ll talk about some tools to help).
Any time people use words to indicate amounts of things, whether that’s amounts of enzymes or amounts of food (fat, protein, carbs, fiber), you need to think of specific numbers to go with these words.
And, you need to remember that everyone’s body is different, which means your body is different.
Turning words into math for pill count and enzymes for EPI
Enzyme intake should not be compared without considering multiple factors.
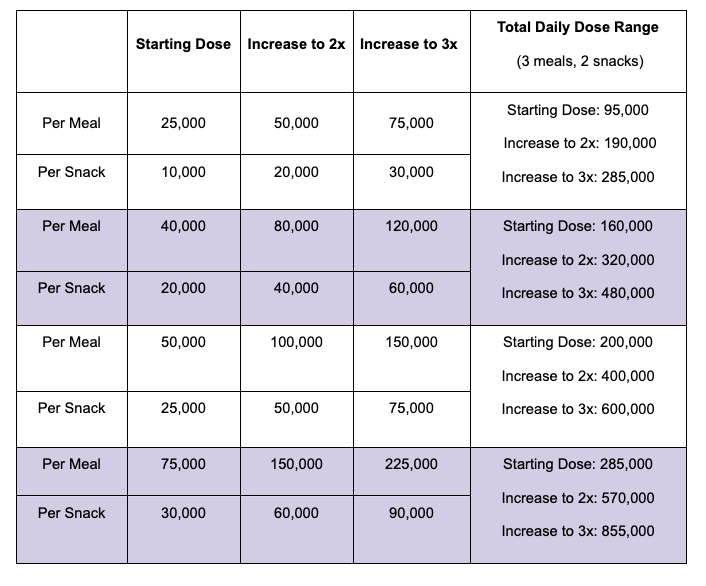
The first reason is because enzyme pills are not all the same size. Some prescription pancreatic enzyme replacement therapy (PERT) pills can be as small as 3,000 units of lipase or as large as 60,000 units of lipase. (They also contain thousands or hundreds of thousands of units of protease and amylase, to support protein and carbohydrate digestion. For this example I’ll stick to lipase, for fat digestion.)
If a person takes two enzyme pills per meal, that number alone tells us nothing. Or rather, it tells us only half of the equation!
The size of the pills matters. Someone taking two 10,000-lipase pills consumes 20,000 units per meal, while another person taking two 40,000-lipase pills is consuming 80,000 units per meal.
That is a big difference! Comparing the two total amounts of enzymes (80,000 units of lipase or 20,000 units of lipase) is a 4x difference.
And I hate to tell you this, but that’s still not the entire equation to consider. Hold on to your hat for a little more math, because…
The amount of fat consumed also matters.
Remember, enzymes are used to digest food. It’s not a magic pill where one (or two) pills will perfectly cover all food. It’s similar to insulin, where different people can need different amounts of insulin for the same amount of carbohydrates. Enzymes work the same way, where different people need different amounts of enzymes for the same amount of fat, protein, or carbohydrates.
And, people consume different amounts and types of food! Breakfast is a good example. Some people will eat cereal with milk – often that’s more carbs, a little bit of protein, and some fat. Some people will eat eggs and bacon – that’s very little carbs, a good amount of protein, and a larger amount of fat.
Let’s say you eat cereal with milk one day, and eggs and bacon the next day. Taking “two pills” might work for your cereal and milk, but not your eggs and bacon, if you’re the person with 10,000 units of lipase in your pill. However, taking “two pills” of 40,000 units of lipase might work for both meals. Or not: you may need more for the meal with higher amounts of fat and protein.
If someone eats the same quantity of fat and protein and carbs across all 3 meals, every day, they may be able to always consume the same number of pills. But for most of us, our food choices vary, and the protein and fat varies meal to meal, so it’s common to need different amounts at different meals. (If you want more details on how to figure out how much you need, given what you eat, check out this blog post with example meals and a lot more detail.)
You need to understand your baseline before making any comparisons
Everyone’s body is different, and enzyme needs vary widely depending on the amount of fat and protein consumed. What is “too much” for one person might be exactly the right amount for another, even when comparing the same exact food quantity. This variability makes it essential to understand your own baseline rather than following generic guidance. The key is finding what works for your specific needs rather than focusing on an arbitrary notion of “too much”, because “too much” needs to be compared to specific numbers that can be compared as apples to apples.
A useful analogy is heart rate. Some people have naturally higher or lower resting heart rates. If someone tells you (that’s not a doctor giving you direct medical advice) that your heart rate is too high, it’s like – what can you do about it? It’s not like you can grow your heart two sizes (like the Grinch). While fitness and activity can influence heart rate slightly, individual baseline differences remain significant. If you find yourself saying “duh, of course I’m not going to try to compare my heart rate to my spouse’s, our bodies are different”, that’s a GREAT frame of mind that you should apply to EPI, too.
(Another example is respiratory rate, where it varies person to person. If someone is having trouble breathing, the solution is not as simple as “breathe more” or “breathe less”—it depends on their normal range and underlying causes, and it takes understanding their normal range to figure out if they are breathing more or less than their normal, because their normal is what matters.)
If you have EPI, fiber (and anything else) also needs numbers
Fiber also follows this pattern. Some people caution against consuming “too much” fiber, but a baseline level is essential. “Too little” fiber can mimic EPI symptoms, leading to soft, messy stools. Finding the right amount of fiber is just as crucial as balancing fat and protein intake.
If you find yourself observing or hearing comments that you likely consume “too much” fiber – red flag check for “too much!” Similar to if you hear/see about ‘low fiber’. Low meaning what number?
You should get an estimate for how much you are consuming and contextualize it against the typical recommendations overall, evaluate whether fiber is contributing to your issues, and only then consider experimenting with it.
(For what it’s worth, you may need to adjust enzyme intake for fat/protein first before you play around with fiber, if you have EPI. Many people are given PERT prescriptions below standard guidelines, so it is common to need to increase dosing.)
For example, if you’re consuming 5 grams of fiber in a day, and the typical guidance is often for 25-30 grams (source, varies by age, gender and country so this is a ballpark)…. you are consuming less than the average person and the average recommendation.
In contrast, if you’re consuming 50+ grams of fiber? You’re consuming more than the average person/recommendation.
Understanding where you are (around the recommendation, quite a bit below, or above?) will then help you determine whether advice for ‘more’ or ‘less’ is actually appropriate in your case. Most people have no idea what you’re eating – and honestly, you may not either – so any advice for “too much”, “too little”, or “more” or “less” is completely unhelpful without these numbers in mind.
You don’t have to tell people these numbers, but you can and should know them if you want to consider evaluating whether YOU think you need more/less compared to your previous baseline.
How do you get numbers for fiber, fat, protein, and carbohydrates?
Instead of following vague “more” or “less” advice, first track your intake and outcomes.
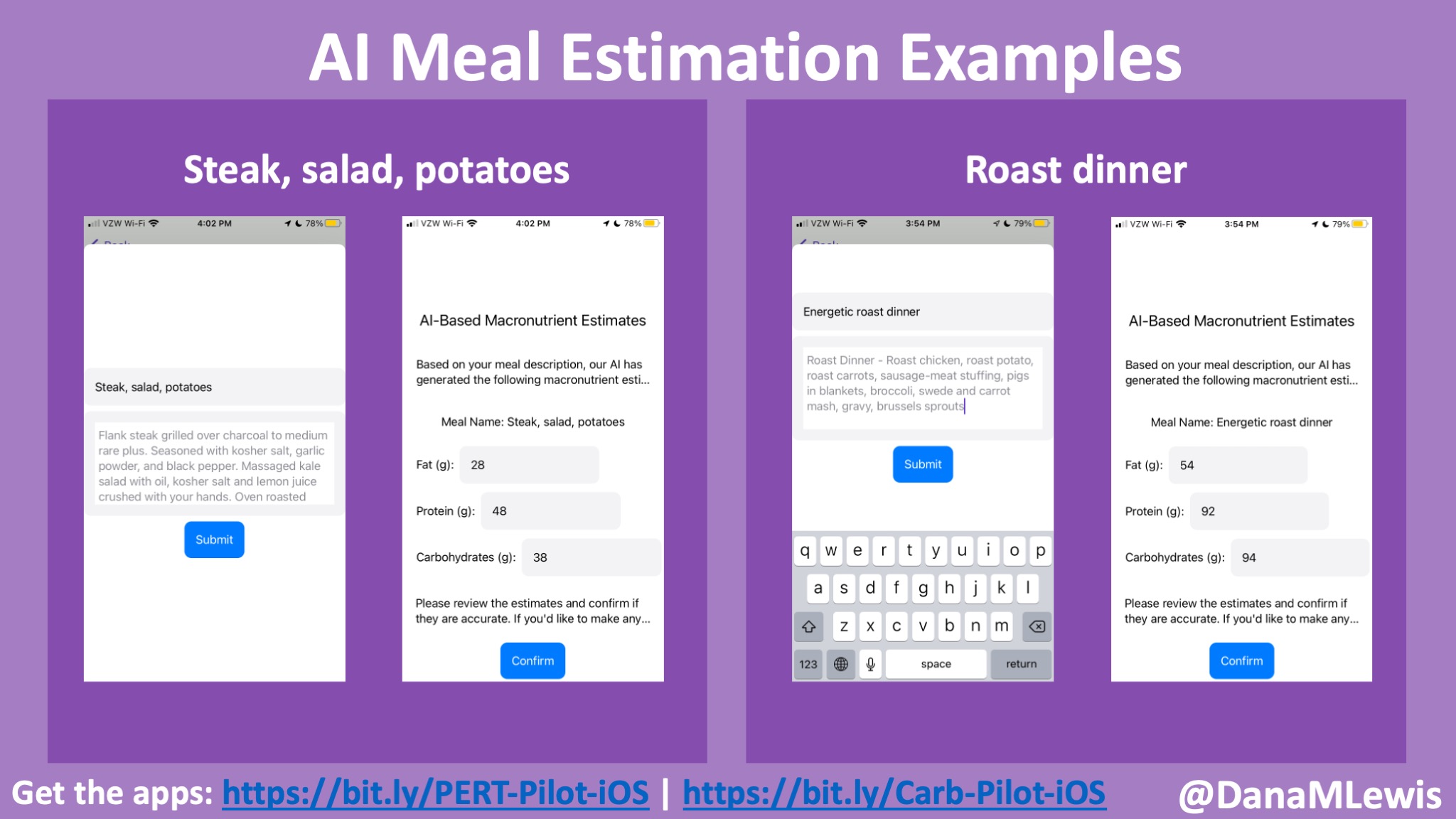
If you don’t have a good way to estimate the amount of fat, protein, carbohydrates, and/or fiber, here’s a tool you can use – this is a Custom GPT that is designed to give you back estimates of fat, protein, carbohydrates, and fiber.
You can give it a meal, or a day’s worth of meals, or several days, and have it generate estimates for you. (It’s not perfect but it’s probably better than guessing, if you’re not familiar with estimating these macronutrients).
If you don’t like or can’t access ChatGPT (it works with free accounts, if you log in), you can also take this prompt, adjust it how you like, and give it to any free LLM tool you like (Gemini, Claude, etc.):
You are a dietitian with expertise in estimating the grams of fat, protein, carbohydrate, and fiber based on a plain language meal description. For every meal description given by the user, reply with structured text for grams of fat, protein, carbohydrates, and fiber. Your response should be four numbers and their labels. Reply only with this structure: “Fat: X; Protein: Y; Carbohydrates: Z; Fiber; A”. (Replace the X, Y, Z, and A with your estimates for these macronutrients.). If there is a decimal, round to the nearest whole number. If there are no grams of any of the macronutrients, mark them as 0 rather than nil. If the result is 0 for all four variables, please reply to the user: “I am unable to parse this meal description. Please try again.”
If you are asked by the user to then summarize a day’s worth of meals that you have estimated, you are able to do so. (Or a week’s worth). Perform the basic sum calculation needed to do this addition of each macronutrient for the time period requested, based on the estimates you provided for individual meals.
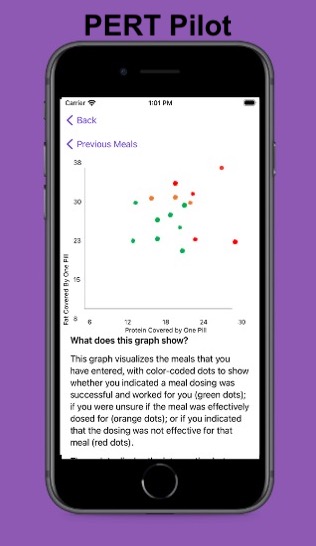
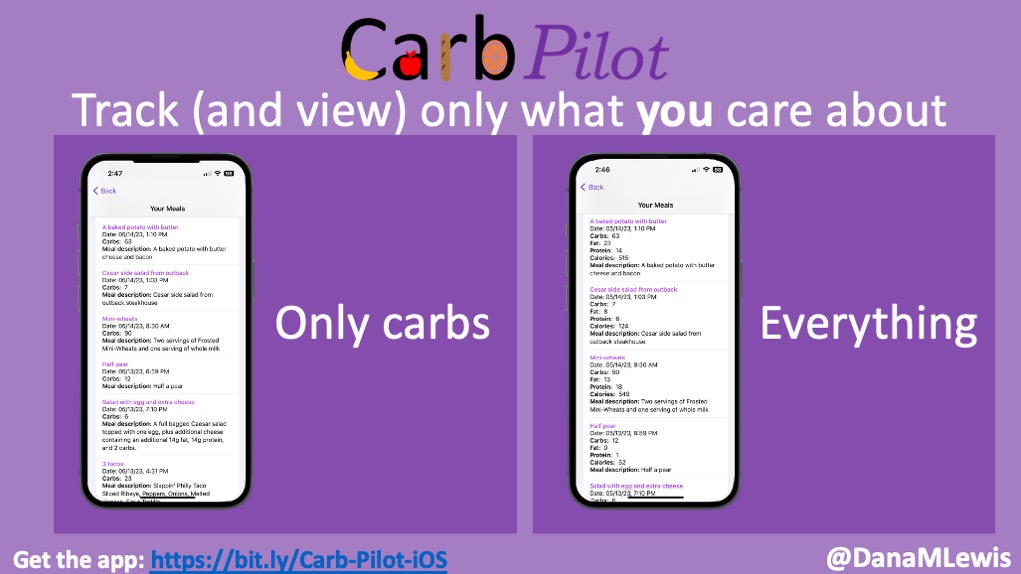
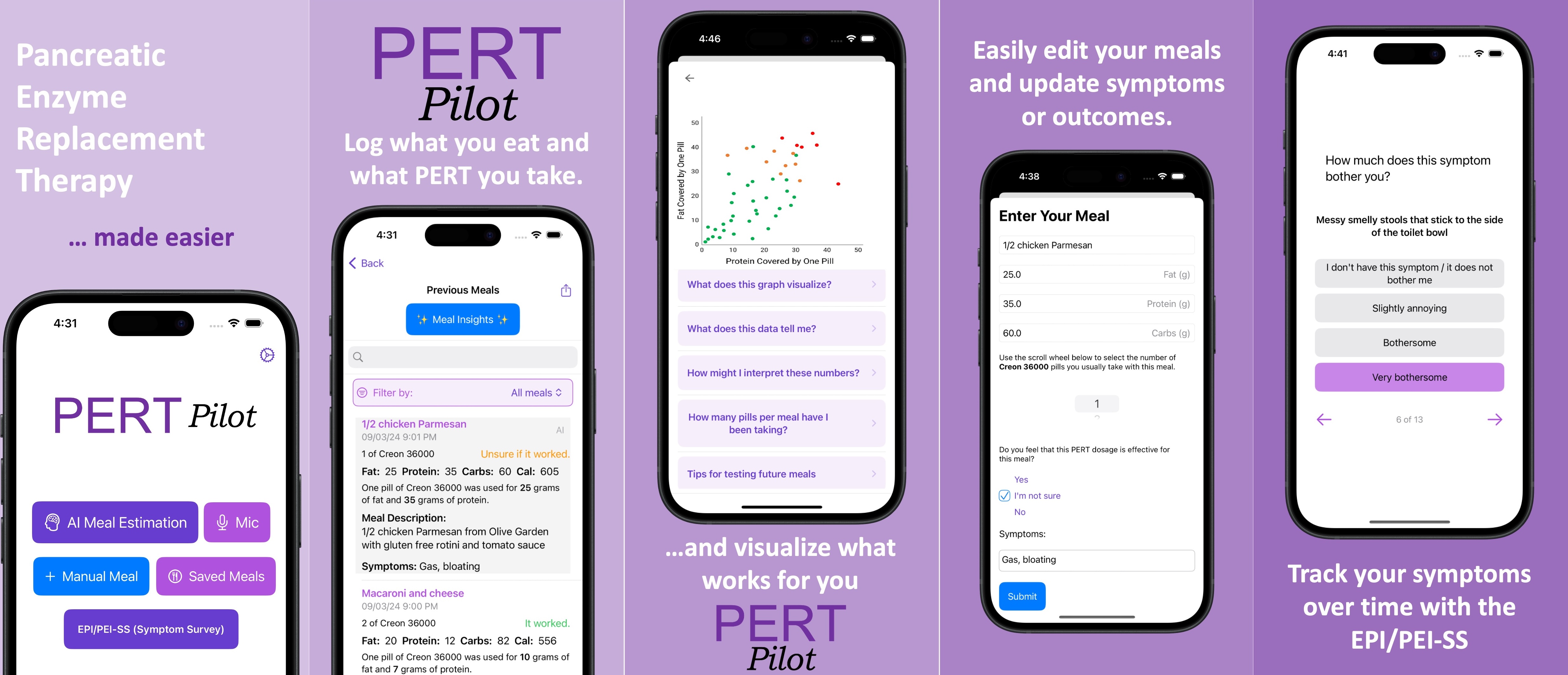
Another option is using an app like PERT Pilot. PERT Pilot is a free app for iOS (and for Android) for people with EPI that requires no login or user account information, and you can put in plain language descriptions of meals (“macaroni and cheese” or “spaghetti with meatballs”) and get back the estimates of fat, protein, and carbohydrates, and record how much enzymes you took so you can track your outcomes over time. (Android users – email me at Dana+PERTPilot@OpenAPS.org if you’d like to test the forthcoming Android version!) Note that PERT Pilot doesn’t estimate fiber, but if you want to start with fat/protein estimates, PERT Pilot is another way to get started with seeing what you typically consume. (For people without EPI, you can use Carb Pilot, another free iOS app that similarly gives estimates of macronutrients.)
—
 TL;DR: Instead of arbitrarily lowering or increasing fat or fiber in the diet, measure and estimate what you are consuming first. If you have EPI, assess fat digestion first by adjusting enzyme intake to minimize symptoms. (And then protein, especially for low fat / high protein meals, such as chicken or fish.) Only then consider fiber intake—some people may actually need more fiber rather than less than what they were consuming before if they experience mushy stools. Remember the importance of putting “more” or “less” into context with your own baseline numbers. Estimating current consumption is crucial because an already low-fiber diet may be contributing to the problem, and reducing fiber further could make things worse. Understanding your own baseline is the key.
TL;DR: Instead of arbitrarily lowering or increasing fat or fiber in the diet, measure and estimate what you are consuming first. If you have EPI, assess fat digestion first by adjusting enzyme intake to minimize symptoms. (And then protein, especially for low fat / high protein meals, such as chicken or fish.) Only then consider fiber intake—some people may actually need more fiber rather than less than what they were consuming before if they experience mushy stools. Remember the importance of putting “more” or “less” into context with your own baseline numbers. Estimating current consumption is crucial because an already low-fiber diet may be contributing to the problem, and reducing fiber further could make things worse. Understanding your own baseline is the key.
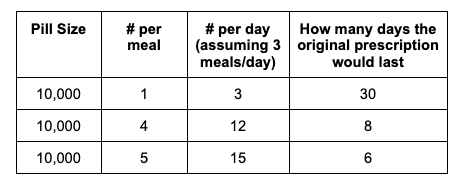
 For example, I was initially prescribed an enzyme dose that was one pill per meal (and no snacks), so I had 3 pills per day. But I quickly found myself needing two pills per meal, based on what I was typically eating. I summarized my data to my doctor, saying that I found one pill typically covered up to ~30 grams of fat per meal, but most of my meals were >30 grams of fat, so that I wanted to update my prescription to have an average of 2 pills per meal of this prescription size. I also wanted to be able to eat snacks, so I asked for 2 pills per meal, 1 per snack, which meant that my prescription increased to 8 pills per day (of the same size), to cover 2 pills x 3 meals a day (=6) plus up to 2 snacks (=2). I also had weeks of data to show that my average meal was >30 grams of fat to confirm that I need more than the amount of lipase I was originally prescribed. My doctor was happy to increase my prescription as a result, and this is what I’ve been using successfully for over a year ever since.
For example, I was initially prescribed an enzyme dose that was one pill per meal (and no snacks), so I had 3 pills per day. But I quickly found myself needing two pills per meal, based on what I was typically eating. I summarized my data to my doctor, saying that I found one pill typically covered up to ~30 grams of fat per meal, but most of my meals were >30 grams of fat, so that I wanted to update my prescription to have an average of 2 pills per meal of this prescription size. I also wanted to be able to eat snacks, so I asked for 2 pills per meal, 1 per snack, which meant that my prescription increased to 8 pills per day (of the same size), to cover 2 pills x 3 meals a day (=6) plus up to 2 snacks (=2). I also had weeks of data to show that my average meal was >30 grams of fat to confirm that I need more than the amount of lipase I was originally prescribed. My doctor was happy to increase my prescription as a result, and this is what I’ve been using successfully for over a year ever since.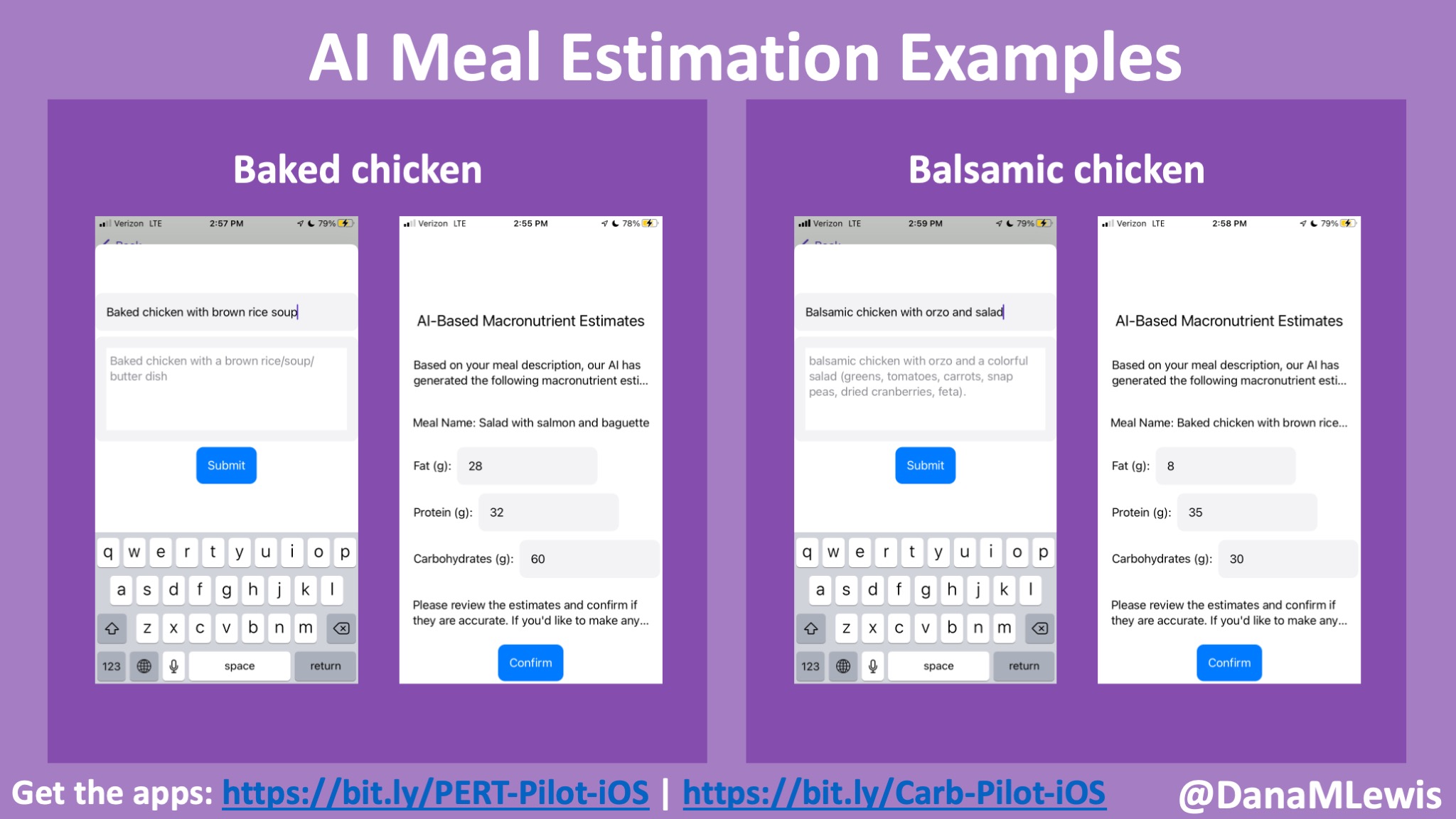


Recent Comments