As someone who’s frequently been asked to travel and give talks over the last decade or so, I’ve had an evolving calculation to determine when a trip is “worth” it. This includes assessing financial cost to me (whether accommodations and travel are paid for; whether my time being paid for or not); opportunity cost (if I do this trip, what can’t I do that I would be doing otherwise); relationship and family cost (time away from family); as well as wellness cost (such as jet lag and physical demands of travel during and after a trip).
It’s clearly not a straightforward calculation and it has changed over time. Some things can influence this calculation – for example, if someone is willing to pay for my time and indicate that they value my presence by doing so, I may factor that in as a higher signal of whether this trip might be “worth” it, among the other variables. (And I’ve written previously about all the reasons why people, including patients, should be paid for their time in giving talks and traveling for conferences, meetings, and events, and I still believe this. However, there *are* exceptions that I personally am willing to make regarding payment for my time, but those are unique to me, my situation, my choices, the type of organization or meeting, etc. and I make these exceptions on a case by case basis.)
The pandemic also changed this calculation by adding new variables.
After February 2020, I did not complete any travel for work (including giving talks, attending conferences, etc.) for the rest of the year or in 2021. I was an early voice for interventions for COVID-19 beginning in February 2020, in part because of the risk to the community around me as well as to the risk to myself as someone who has type 1 diabetes. I received a few in-person speaking invitations that I turned down directly, or encouraged them to evolve into virtual events so that I and others could participate safely.
Now, though, it’s becoming clear (sadly) that COVID-19 will be endemic, and although I am not ready to go back to in-person events, many people are, and conferences are increasingly returning and planning to return to in-person physical events moving forward.
And as a result, I see and experience a mismatch in risk tolerance and risk calculations among different groups of people.
For some people, the risk calculation is as simple as considering, “am I fully vaccinated? Then I’m good to go and attend any events and follow whatever regulation or lack of regulation exists for that conference.”
For other people, it is a more complex risk calculation. It may take into account whether they are someone with a condition or chronic illness that puts them at higher risk for severe outcomes, even with COVID-19 vaccination. It may take into account a loved one or family situation where someone close to them is at higher risk. It may take into account that there are different rates of COVID-19 cases, and different rates of vaccination, at their home location compared to the conference location. It may take into account the risk of disruption to their lives if they were to acquire COVID-19 during travel or at the conference and be forced to remain in a different city or country, sick and alone, until they were cleared to travel. That also includes the financial disruption of paying for lodging, changed travel plans, as well as any disruption to home life where childcare or other plans were upended at home while the person was stuck elsewhere.
It is, therefore, much more complicated than “am I vaccinated?” and “does the conference have a protocol?”.
There’s no straightforward answer; there may not be the same answer for everyone in the same situation. Therefore people are also likely to have different risk calculations to make and may arrive at a different decision than you might want them to make.
I hope we can all expand our awareness and recognize that different people have different situations and that the COVID-19 pandemic – still – affects all of us very differently.
As part of my pandemic “fun” (but fortunately not from COVID-19 infection, which I’ve avoided), I developed some gastrointestinal dysbiosis. Gastrointestinal dysbiosis generally means microbiome dysfunction of some kind, hypothetically caused by a loss of ‘good’ bacteria and getting out of balance with ‘bad’ bacteria. I don’t have a diagnosable disease such as IBS (that and many other things were ruled out through a variety of medical testing), but I definitely have some dysfunction going on causing varying levels of GI symptoms now for almost a year and a half. At their worst, I was waking up overnight suddenly with sharp abdominal pain out of the blue – scary! At their least annoying, it was excess gas and general abdominal discomfort after eating. It ebbed and flowed and did not seem to be traceable to any particular cause. After several months, I consulted a gastroenterologist and did an assortment of tests over the course of ~10 months, slowed down by the pandemic and my reluctance to do in-person clinical tests until I was fully vaccinated against COVID-19 (we checked for c-diff and inflammation among other blood tests, did a CT scan, and eventually did a colonoscopy and endoscopy). The test results all came back normal. Eventually, we decided on a treatment plan that involved an antibiotic to kill excess bacteria in my small intestines. That worked – for about two weeks – and then my symptoms returned. I needed another solution, and before I went back to my gastroenterologist to talk about more extreme options, I decided first to self-test a low FODMAP diet.
(As a note to those who don’t know – I have had type 1 diabetes for almost 19 years, and celiac disease for about 13 years. As a result, I’ve been 100% fastidiously gluten free for 13 years and already eating a gluten free diet. P.S. I’m not a doctor and nothing in this post or this blog is medical advice.)
What a low FODMAP diet means in simplified terms
FODMAP is an acronym for different groups of short-chain carbohydrates, or sugars, that can cause symptoms for some people when they eat them, because the small intestine absorbs them poorly. FODMAP stands for fermentable oligosaccharides, disaccharides, monosaccharides and polyols.
The FODMAP diet is often discussed in the context of IBS (one particular condition), but it can be used by people with a variety of gut dysbiosis issues, many of whom (like me) don’t necessarily have a diagnosable condition or disease.
One reason I decided to try a low FODMAP diet is because I had identified onion and garlic as potential food-related triggers or variables that correlated with some of the worst of my symptoms. I began attempting to eliminate onion and garlic (and then onion powder and garlic powder) from my diet from January 2021-May 2021. It helped, but I was still having varying levels of symptoms.
Generally, people who describe being on a low FODMAP diet are referring to the first step of a three-step or three-phase diet. The first step is eliminating the major sources of FODMAPs. Then, a careful re-introduction process takes place to “test” and see which of the groups of FODMAPs you react to, and in what amounts. With that knowledge, the third phase is then eating what you’re willing to eat based on your knowledge of what FODMAPs bother you and what you’re willing to tolerate symptom-wise.
What most people don’t realize at first is that the amount of FODMAP and type of FODMAP matter, in each of the phases.
For example, there are a lot of blog posts and lists that will describe things that are “low FODMAP”. And they are partially right, but they leave out specifications that if you eat too many of them, the FODMAP amount may be considered “high” (meaning likely to trigger symptoms). Additionally, you can eat multiple things with the same type of FODMAP and cause FODMAP stacking, meaning you cumulatively have too much of the group of FODMAP and can cause symptoms, even if you ate the “right” low FODMAP portion of each individual food. Sometimes eating the same group within a short period of time can cause stacking, and so spreading them out 3-4 hours apart (or longer) could help reduce the effect.
(P.S. If you are looking for a simplified explanation to share with family and friends, skip to the bottom of the post!)
Resources for getting started with low FODMAP diet and some pros and cons to each
There are many blogs out there that will describe FODMAPs and the process of FODMAP elimination pretty well. Many have short lists of examples of foods that are “high FODMAP” and to avoid. The challenge, as I mentioned, is that the amount of food matters and knowing the type of FODMAP it contains really helps. There are many “high FODMAP” foods that you can eat in small quantities, and it’s also possible that you can eat large quantities of “low FODMAP” foods and accidentally stack FODMAPS from the same group and cause symptoms. With this diet and process, knowledge is power (even though it is very annoying to have to read ingredient labels and super sleuth everything you eat…).
There are several lists or spreadsheets of low FODMAP foods. Here is one that I found that is freely available. It lists the ingredient, it’s “max use”, and has information about the FODMAP group. This is information pulled from the Monash app and may be out of date – same with many blog posts or online lists you might find, such as this one!
How I used many of these free lists and blog posts was to get a sense of “green” or “low FODMAP” foods. There are a few types of foods that are really “free” meaning you can eat as much as you want because they don’t contain any level of FODMAP, so they shouldn’t affect you regardless of the quantity you eat. I first made a list of these “free” foods (I’m probably pulling this “free” terminology from early-2000-era diabetes food terminology) that I actually like and want to eat. For example, for me, this was eggs, grits, carrots, baby corn, peanuts, most cheese, and popcorn. This is what I ate for the first handful of days while I was doing my research on what else would constitute a low FODMAP diet. It sounded and felt restrictive, but thankfully as I learned more I realized that I could eat a lot more things and a better diversity of things.
The next app/tool that helped was the Monash app. One caveat – it costs money. I waited a few weeks before I finally caved and paid $8 USD for it. The reason I finally decided to get it (vs using tools like that spreadsheet above and other places that have information from Monash available) is I wanted the quick visual glance the app has about whether the food is completely low FODMAP and ‘free’ to eat (e.g. carrots, eggs) or low FODMAP in certain portion sizes, or pretty much high FODMAP no matter what. Monash is a university in Australia that does most of the research and testing on FODMAPs in foods, so I decided paying for the app was a way to invest in the research that I’m clearly benefiting from.
Example from Monash’s app showing different color orders
I do have some frustrations with the Monash app, though. It only includes foods that they’ve happened to measure…which is a good amount, but not as many as I’d like. It also confusingly sometimes lists the different serving sizes in opposite order. For example, there might be a “green” overall rating, with a certain portion size indicated in green but also showing the yellow/amber “moderate” amount portion size alongside the red “high” portion size, so you can see the difference. However, sometimes they list the portion size in opposite directions. This search for bananas is a good example – the color indicators on “Banana, sugar (ripe) goes red-amber-green; the color indicators on “Banana, common (unripe)” goes green-amber, and the color indicators on “Banana, common (ripe)” goes red-amber-green again.
Their rationale for this is that standard serving size and traffic light rating will always be the first traffic light so foods may start green and go red as serving sizes increase or start red and become green with smaller servings. However, it means as a user that you have to pay close attention to the order and serving sizes and it’s not the same across the app.
You also have to pay attention to the tiny, grey text at the bottom below the individual ratings. The text isn’t the same from item to item. For example, peanuts are marked as green, no other color rating. When you click to see the details, it shows a portion size of 32 nuts (0.99 ounce), and the text indicates the portion only contains trace amounts of FODMAPs and “eat freely according to appetite”. Same for carrots, so these are what would constitute a “free” food where you don’t have to worry about FODMAP stacking.
However, when you look at pecans, it also has a green overall rating. But the serving size is 10 pecan halves (0.71 ounce) and the grey text indicates that “Large servings (40 pecan halves or 100g/3.5oz) contains moderate amounts of the Oligos-fructans and intake should be limited.”
Example of Monash’s app showing peanuts as the resultExample of Monash’s app showing pecans as the resultExample of Monash’s app showing the search result with peanuts and pecans
This means you can’t just eyeball the app and take the green overall traffic light rating, even if it just has a green overall rating and doesn’t have the additional lights (like under the bananas) indicating warnings about different portion sizes. The warnings about portion sizes may be hidden in the grey text that your brain doesn’t want to read because it assumes the text is always the same.
(The other thing I don’t love about the Monash app is that it’s language is very IBS focused. But there’s a lot of people using low FODMAP for non-IBS reasons, so you can mostly ignore that. It has other tools like a diary for symptoms and food intake and a re-introduction tracker for when you do re-challenges of FODMAPs.)
Another app resource is an app called “Spoonful”. It’s free: although you can pay something like $2.99 for a premium version, the free capabilities suit my purpose. You can scan a barcode or type and search for store-bought products, which is a great use case for me since I don’t cook a lot from scratch. It has different color coding (and you can limit your search to a color type) for whether a given food has low, moderate or high FODMAPs in one serving. It’s supposed to be dietitian-reviewed and approved. It’s good for gut-checking your interpretation of an ingredient label, but there’s a caveat that I’ve found several inconsistencies within the app (and already flagged and reported them). For example, I spotted a chip that was sour cream and onion and supposedly low (green rating) FODMAP *and* cited as officially certified as low FODMAP. Except…it has onion powder as a major ingredient and I am not sure it could be considered low FODMAP. (What I think happened is that Australia’s version of the company has a sour cream and chive chip that looks pretty similar and is certified low FODMAP, and they accidentally swapped them within the app.) I reported that one, and they were quick to fix it within days, so it is now correctly marked as high FODMAP. In another search I did, milk and milk related products are flagged in one flavor of a food (e.g. an ice cream bar), but a slightly different flavor that’s still the same ice cream doesn’t have the milk ingredients flagged and has a completely different color rating as a result with those ingredients not flagged (in the same quantities). A third type of error I have found is that you can scan a barcode of a product, and the labeled ingredients listed in the app do not match the ingredients currently on the package – it’s pulling from a stored list of ingredients that could be outdated. So as a user, you have to eyeball and make sure the app listed ingredients matches the ingredients on the product in your hand, then compare any potential FODMAP-containing ingredients that are either flagged in the app or might be in your hand but not listed on the app, if those ingredient labels differ.
Hypothetically these are medium or small errors, but given the number of errors like that where they inconsistently flag ingredients across the same type of food item that result in variable color ratings, I would not rely just on their color rating and instead double check the ingredients yourself (including comparing them to the version you are holding in your hand). If you’re as sensitive to FODMAPs as I am, it’s worth double checking and thinking it through each time.
Additionally, the Spoonful app (as of August 2021) only supports one diet filter search at a time. Thankfully, I’ve had celiac forever and am comfortable knowing how to also determine if something is gluten free or not. So it’s not a big deal for me to “just” use the low FODMAP search to see what’s FODMAP-y or not, with the above caveats. But low FODMAP does not mean gluten free, even though some wheat-related items are high FODMAP, so do not use anything that’s low FODMAP as an indicator that it’s celiac-safe!
As another way of checking things out, it’s always helpful to google “Ingredient name FODMAP” or “Food name FODMAP” – often there are blog posts discussing the food type, or Reddit or similar forum posts discussing individuals’ experiences with that ingredient or food type.
However, one more important thing to keep in mind: it may be “low FODMAP” or “no FODMAP”, and it can still cause symptoms. Everyone is different, and that’s the point of needing to re-challenge each group to determine what groups bother you, and in what quantities. Additionally, some no-FODMAP foods or ingredients could be bothersome, and it has nothing to do with FODMAPs. For example, I noticed Crystal Light was bothering me last year and stopped drinking it. After I did the first phase of low FODMAP (the elimination phase) for a few weeks, I decided to test Crystal Light since it’s theoretically not containing FODMAP ingredients. However, it definitely caused symptoms that weren’t attributable to anything else, so it’s on my “don’t drink” list, just like onion soup would be, even though Crystal Light isn’t considered to have FODMAPs.
So how exactly do you do the different FODMAP diet phases?
Most everything I read online said the first phase, the elimination phase where you eat 100% low FODMAP, should be around 2-6 weeks. Another piece of data was that many dietitians recommend having 5-7 symptom-free days before starting food re-challenges (e.g. the second or next phase).
If you’re like me, you might get accidentally FODMAP’ed, as I call it, or experience FODMAP stacking by accident within your first few weeks as you work out the correct portion sizes of things and when to eat them. My rule of thumb was aiming for 2 weeks overall on the elimination/first phase, but also going for several days without symptoms so I had a “clean slate”, so to speak, before starting the challenges. I am lucky, relatively speaking, that I don’t have the major symptoms that most people with IBS who do FODMAP seem to experience – I don’t have diarrhea or constipation or that spectrum to deal with. My symptoms are usually noticeable immediately or within 12 hours, but they also resolve pretty quickly, so I can see the correlation between what I eat and the results fairly easily. As a result, I went a little more than 2 weeks attempting to do full low FODMAP elimination, had an extra few days added on due to some accidental FODMAP stacking, before I began my first “challenge” food.
The challenge foods should be ones that only contain one of the FODMAP groups. If you pick something that has multiple FODMAP groups, it’ll be hard to tell which FODMAP you’re reacting to or if it’s the stacking effect. I started with lactose (because I’m pretty confident already that I’m not lactose intolerant and it’s not an issue group for me) because it’s an easy one to start and cross off my list. The others I’ve personally decided to use as my test foods are cashews (Fructan+GOS); Apple (Fructose+Sorbitol); Raisins (Fructan: veggie & fruits); Almonds (GOS); Honey (Fructose); Sweet Potato (Mannitol); and Peach (Sorbitol).
Because I have celiac disease, I am of course skipping wheat bread and wheat pasta (Fructan: grain foods). I’m also skipping the separate fructan test for onions and garlic because I know I react to those and have already reverse-tested eliminating those in the past year. I might eventually test onion powder and garlic powder, but I’m de-prioritizing those to be after I test most of the others.
(The Monash app in the reintroduction section has several foods recommended for each group and the amounts for each, so that’s a good resource for selecting some of the challenge foods).
Two schools of thought for re-challenging: you can do day 1, 2, and 3 in a row with the increasing amount prescribed, or you can do every other day with a “washout” (e.g. fully low FODMAP) day in between. If you have moderate to major symptoms, you stop and have 3 washout days before you proceed with the next test. It’s up to you to decide what symptoms are tolerable and whether you proceed or cross that group off your list (for now). You can always come back and re-challenge or re-test groups or food at any time.
Finally, the third phase is what you get to when you’ve done all your testing and have an idea of what FODMAP groups are irritants or triggers, which foods as a result you want to avoid or continue to experiment with. Ideally, you arrive at a more diverse diet than the full elimination stage of low FODMAP. (Again, I’m not a doctor or dietitian, and I’m DIY-ing my low FODMAP experience, and these are all the conclusions I’ve arrived at after copious reading online and in the medical literature.)
What do you tell family and friends about the low FODMAP diet?
It depends, especially on what your lifestyle is and what stage of the diet that you are at (and also if you’re in a global pandemic which limits your eating-out options).
Because this experience has been during a global pandemic, I am no longer eating out at restaurants (to avoid being unmasked around strangers) which made things easier in the sense that I didn’t have to try to figure out low FODMAP restaurant options. But it was harder because I couldn’t even get gluten free takeout or delivery food anymore, and now have to make all my food myself. For the few social food situations I had with my in-laws (we are all fully vaccinated and use antigen testing to make sure we aren’t infectious on the days we visit in person), I have mostly decided to take my own food. I’ve stashed a few things in the freezer and pantry at their house to be able to make a meal and just let everyone else do takeout without me, so that we can all still sit down together for a meal. I have described what I’m doing and what it entails (such as avoiding onion and garlic and only eating particular things in particular amounts), but it’s hard to describe to most people at a high level because of the complexity of the types of foods (it seems random unless you think about the biochemistry) and the quantities. It makes me nostalgic for explaining only celiac to people, because “gluten free” is a much smaller category of ingredients to watch for and avoid, compared to FODMAPs and FODMAP quantity specifics. That being said, already being gluten free means I’m experienced at reading ingredient labels and have a head start on excluding some of the major FODMAP groups (fructan grain foods are usually gluten) and don’t have to (well, don’t get to) re-test those.
A friend recently said (because she’s amazing) that she wanted to read up on what a low FODMAP diet means, and I couldn’t find a good high level simple article to send to her, so I had to type up an explanation. So what I have summarized to her and family and other friends is this:
I have GI dysbiosis where I react to a lot of what I’m eating. I’m experimenting with a low FODMAP diet, which starts with a partial elimination diet to restrict the types of FODMAPs that I eat. FODMAPs are certain types of carbs that don’t digest well. During this stage, I’m avoiding things like onion, garlic, certain sweeteners, many fruits, and more. Even small amounts of these ingredients can make me feel bad, just like gluten, although they cause shorter term symptoms. What I can eat freely are plain meat and protein including eggs; vegetables like cucumbers, carrots, potatoes, and baby corn; and cheese, among other things. I need to check the ingredients on everything I eat, even things that we know are already gluten free.
Eventually, I will begin to “test” my response to the FODMAP foods. I’ll still be carefully managing what I eat while I do these tests so that I have a “clean slate” to see how my body responds to the type and quantity of each food. My hope is to be able to add some of the food groups back into my diet, but it may be only restricted amounts. It will be several months before I progress through all the tests.
I can use your support – I’m looking for low FODMAP alternatives to foods like X, Y, and Z, so if you’d like to help, in addition to listening to me vent, you could help me research some store-bought or homemade alternatives to these.
(One reason I add the “I can use your support” aspect for some people, which is obviously optional – I learned from being gluten free with celiac that having friends and family aware of what it takes to eat and find safe gluten-free options really cut down on the emotional labor required to find and suggest food every time. People try to be nice and let me offer gluten free options for eating out, but that means I have to do a lot of research every time. Having family members put the “Find Me Gluten Free” app on their phone and teaching them how to do basic searches so they could offer up suggestions, too, made a big difference. I won’t ask everyone for help re: FODMAP but for certain family members, they really can make a difference in doing some of the searching for low FODMAP alternatives to certain things that I haven’t been able to find yet! For me, this is things like finding a low FODMAP steak sauce that I could buy. I still haven’t found one. Thankfully, there’s also brands like Fody where I buy a lot of sauces (BBQ sauce, spaghetti sauce, ketchup) and salad dressings – plus now they have tasty BBQ chips that are also gluten free, and meal delivery services like Epicured that I’ve tried. Note – I am not sponsored or paid by either of those brands, I shell out my own money for them!)
Example fill in the blank script to customize to help you explain your FODMAP experience to family and firends
—
At the end of the day, the one thing you need to know about FODMAP is that everyone is different. Literally, you are a scientific experiment of one. What works for someone else doesn’t necessarily work for you. You know you, and you get to decide what level of symptoms you are willing to tolerate – or not – in response to different quantities of food. Whether it’s IBS, small intestinal bacterial overgrowth (SIBO), some other condition, or general gastrointestinal dysbiosis, a low FODMAP diet may be one option that you can try and see if it helps you feel better. In diabetes, we often say “YDMV”, meaning ‘your diabetes may vary’. In the landscape of GI-related stuff, I think it’s “YFWV”, meaning “your FODMAP experience will vary.”
2020. What a year. We’ve been social distancing since late February and being very careful in terms of minimizing interactions even with family, for months. We haven’t traveled, we haven’t gone out to eat, and we basically only go out to get exercise (with a mask when it’s on hiking trails/around anyone) or Scott goes to the grocery store (n95 masked). We’ve been working on CoEpi (see CoEpi.org – an open source exposure notification app based on symptom reports) and staying on top of the scientific literature around COVID-19, regarding NPIs like distancing and masking; at-home diagnostics like temperature and pulse oximetry monitoring, prophylactics and treatments like zinc, quercetine, and even MMR vaccines; and the impact of ventilation and air quality on COVID-19 transmission and susceptibility.
And we live in Washington, so the focus on air quality got very real very quickly during this year’s wildfire season, where we had wildfires across the state of Washington, then got pummeled for over a week with hazardous levels of wildfire smoke coming up from Oregon and California to cover our existing smoke layer. But, one of our DIY air quality hacks for COVID-19 gave us a head start on air quality improvements for smoke-laden air, which I’ll describe below.
Here are various things we’ve gotten and have been using in our personal attempts to thwart COVID-19:
Finger pulse oximeter.
Just about any cheap pulse oximeter you can find is fine. The goal is to get an idea of your normal baseline oxygen rates. If you dip low, that might be a reason to go to urgent care or the ER or at least talk to your doctor about it. For me, I am typically 98-99% (mine doesn’t read higher than 99%), and my personal plan would be to talk to a healthcare provider if I was sick and started dropping below 94%.
Thermometer
Use any thermometer that you’ll actually use. I have previously used a no-touch thermometer that could read foreheads but found it varied widely and inconsistently, so I went back to an under the tongue thermometer and took my temperature for several months at different times to figure out my baselines. If sick or you have a suspected exposure, it’s good to be checking at different times of the day (people often have lower temps in the morning than in the evening, so knowing your daily differences may help you evaluate if you’re elevated for you or not).
Note: women with menstrual cycles may have changes related to this; such as lower baseline temps at the start of the cycle and having a temperature upswing around or after the mid-point in their cycle. But not all do. Also, certain medications or birth controls can impact basal temperatures, so be aware of that.
Originally, n95 masks with outlet valves.
Note: n95 masks with valves cannot be used by medical professionals, because the valves make them less effective for protecting others. (So don’t freak out at people who had a box of valved n95 masks from previous wildfire smoke seasons, as we did. Ahem.)
We had a box we bought after previous years’ wildfire smoke, and they work well for us (in low-risk non-medical settings) for repeated use. They’re Scott’s go-to choice. If you’re in a setting where the outlet valve matters (indoors in a doctor’s/medical setting, or on a plane), you can easily pop a surgical/procedure mask over the valve to block the valve to protect others from your exhaust, while still getting good n95-level protection for yourself.
They were out of stock since February, but given the focus on n95 without valves for medical PPE, there have been a few boxes of n95 masks with outlet valves showing up online at silly prices ($7 per mask or so). But, kn95’s are a cheaper per mask option that are generally more available – see below.
(June 2021 note – they are back to reasonable prices, in the $1-2 range per mask on Amazon, and available again.)
kn95 masks.
kn95 masks are a different standard than US-rated n95; but they both block 95% of tiny (0.3 micron) particles. For non-medical usage, we consider them equivalent. But like n95, the fit is key.
We originally bought these kn95s, but the ear loops were quite big on me. (See below for options if this is the case on any you get.) They aren’t as hardy as the n95s with valves (above); the straps have broken off, tearing the mask, after about 4-5 long wears. That’s still worth it for them being $2-3 each (depending on how many you buy at a time) for me, but I’d always pack a spare mask (of any kind) just in case.
Option one to adjust ear loops: I loop them over my ponytail, making them head loops. This has been my favorite kn95 option because I get a great fit and a tight seal with this method.
Option two to adjust ear loops: tie knots in the ear loops
Option three to adjust ear loops: use things like this to tighten the ear loops
We also got a set of these kn95s. They don’t fit quite as well in terms of a tight face fit, but these actually work as ear loops (as designed), and I was able to wear this inside the house on the worst day of air quality.
Box fan with a filter to reduce COVID-19 particles in the air:
We read this story about using an existing AC air furnace filter on a box fan to help reduce the number of COVID-19 particles in the air. We already had a box fan, so we took one of our spare 20×20 filters and popped it on. I’m allergic to dust, cats (which we just got), trees, grass, etc, so I knew it would also help with regular allergens. There are different levels of filter – all the way up to HEPA filters – but we had MERV 12 so that’s what we used.
Phone/object UV sanitizer
We got a PhoneSoap Pro (in lavender, but there are other colors). Phones are germy, and being able to pop the phone in (plus keys or any other objects like credit cards or insurance cards that might have been handled by another human) to disinfect has been nice to have.
The Pro is done sanitizing in 5 minutes, vs the regular one takes 10 minutes. It’s not quite 2x the price as the non-pro, but I’ve found it to be worthwhile because otherwise, I would be impatient to get my phone back out. I usually pop my phone in it when I get home from my walk, and by the time I’m done washing my hands and all the steps of getting home, the phone is about or already done being sanitized.
Bonus (but not as useful to everyone as the above, and pricey): Oura ring
Scott and I also both got Oura rings. They are pricey, but every morning when we wake up we can see our lowest resting heart rate (RHR), heart rate variability (HRV), temperature deviations, and respiratory rate (RR). There have been studies showing that HRV, RHR, overnight temperature, and RR changes happen early in COVID-19 and other infections, which can give an early warning sign that you might be getting sick with something. That can be a good early warning sign (before you get to the point of being symptomatic and highly infectious) that you need to mask up and work from home/social distance/not interact with other people if you can help it. I find the data soothing, as I am used to using a lot of diabetes data on a daily and real-time basis (see also: invented an open source artificial pancreas). Due to price and level of interest in self-tracking data, this may not be a great tool for everyone.
Note this doesn’t tell you your temperature in real time, or present absolute values, but it’s helpful to see, and get warnings about, any concerning trends in your body temperature data. I’ve seen several anecdotal reports of this being used for early detection of COVID-19 infection and various types of relapses experienced by long-haulers.
And here are some things we’ve added to battle air quality during wildfire smoke season:
We were already running a box fan with a filter (see above for more details) for COVID-19 and allergen reduction; so we kept running it on high speed for smoke reduction.
Basic steps: get box fan, get a filter, and duct tape or strap it on. Doesn’t have to be cute, but it will help.
I run this on high speed during the day in my bedroom, and then on low speed overnight or sleep with earplugs in.
We already had a small air purifier for allergens, which we also kept running on high. This one hangs out in our guest bedroom/my office.
We caved and got a new, bigger air purifier, since we expect future years to be equally and unfortunately as smoky. This is the new air purifier we got. (Scott chose the 280i version that claims to cover 279 sq. ft.). It’s expensive, but given how miserable I was even inside the house with decent air quality thanks to my box fan and filter, little purifier, and our A/C filtered air… I consider it to be worth the investment.
We plugged it in and validated that with our A/C-filtered air combined with my little air purifier and the box fan with filter running on high, we already had ‘good’ air quality (but not excellent). We also stuck it out in the hallway to see what the hallway air quality was running – around 125 ug/m^3 – yikes. Turns out that was almost as high as the outside air, which is I’ve had to wear a kn95 mask even to walk hallway laps, and why my eyes are irritated.
Check your other filters while you’re on air quality monitoring alert. We found our A/C intake duct vent had not had the air filter changed since we moved in over a year ago… and turns out it’s a non-standard size and had a hand-cut stuffed in there, so we ordered a correctly sized one for the vent, and taped a different one over the outside in the interim.
The other thing to fight the smoke is having n95 with valves or kn95 masks to wear when we have to go outside, or if it gets particularly bad inside. Our previous strategy was to have several on hand for wildfire season, and we’ll continue to do this. (See above in the COVID-19 section for descriptions in more detail about different kinds of masks we’ve tried.)
2022 update: I got a mini personal air purifier to try for travel (to help reduce risk of COVID-19 in addition to all other precautions like staying masked on planes and indoor spaces), but it also turned out to be beneficial inside during the worst of our 2022 wildfire smoke season. I had a slightly scratchy throat even with two box fans and two different air purifiers inside; but keeping this individual one plugged in and pointed at my face overnight eliminated me waking up with a scratchy throat. That’s great for wildfire smoke, and also shows that there is some efficacy to this fan for it’s intended purpose, which is improving air around my face during travel in inside spaces for COVID-19 and other disease prevention.
—
Wildfires, their smoke, and COVID-19 combined is a bit of a mess for our health. Stay inside when you can, wear masks when you’re around other people outside your household that you have to share air with, wash your hands, and good luck.
tl;dr – A new book out for kids explaining the basics of automated insulin delivery, using the analogy of scuba diving to explain how the system makes small changes in insulin delivery to manage glucose levels! Watch the narrated video free online, and if you find the analogy useful, it’s available in book form as both a physical, print book as well as on Kindle via Amazon.—-
A few weeks ago I was thinking about what the basic things that I wanted people to know about automated insulin delivery. A good portion of the general public – and even many family members of people with diabetes – thinks that a traditional insulin pump does what an automated insulin delivery system does: adjusting insulin delivery based on continuous glucose monitor (CGM) data. But a traditional pump doesn’t necessarily know about the CGM data and isn’t equipped with the algorithm to make those decisions and changes to insulin delivery, so the person with diabetes is doing a LOT of invisible labor to try to manage glucose levels constantly 24/7/365. That’s why an automated insulin delivery system is so useful, and why I’ve been using a DIY system for more than 5 years. Now, though, we’re (finally) starting to see commercial systems come to market that does the basic functionality similar to what OpenAPS could do five years ago. I want more people to have access to these systems and use them as best as they can be used to give people the best outcomes diabetes-wise and the best quality of life they can possibly have. Helping explain to more people how this technology works is one way I can help do this, and thus an idea was born for another book to explain the basics of automated insulin delivery systems.
I started with a basic sketch of an idea to run it by Scott and a few other people to test the idea. I’m not much for drawing, so it was a *very* rough sketch. But the analogy seemed to resonate, so I moved on to mocking up a basic version on the computer. (I went down a rabbit hole because I thought it would be neat to make an animated video for people to see and share online, to accompany the book. But I don’t know how to illustrate on the computer, let alone animate, so I tried an open source illustration program called Synfig, then several other illustrator programs that were open source to do the basic design to import into Synfig to animate, but then realized what I had in mind was so simple that basic transitions and animations in PowerPoint would suffice for my animated video.) PowerPoint is also how I’ve made my other children’s books for self-publishing, so it was easy to do a widescreen, video design version and then modify a version for the print size book of choice (I chose an 8.5×8.5 to make it easiest to hold and read).
I went from a paper and pencil sketch on July 18 to mocking up the video animation and designing the print book and requesting printed proofs on July 23. The printed proofs were a bit slow to ship compared to usual (probably something to do with a global pandemic), and arrived on August 4. I reviewed, made a few small changes, and hit ‘publish’ the same day, and Amazon reviewed and approved both the Kindle version and the print version, which are now available today (August 5, 2020) online. It took less than 3 weeks to go from idea to printed book available for shipping worldwide! (I am sharing all these details to hopefully encourage someone else to self-publish if they have an idea for a book they’d like to see available in the world – feel free to reach out if you have any questions about self publishing!)
Also, if you’re looking for something to do with your kids (or have your kids do), I also made some of the scuba diving designs into a coloring sheet – check them out here (downloads as a PDF).
In previous years (see 2019 and 2018), I mentioned sharing content from ADA Scientific Sessions (this year it’s #ADA2020) with those not physically present at the conference. This year, NO ONE is present at the event, and we’re all virtual! Even more reason to share content from the conference.
I contributed to and co-authored two different posters at Scientific Sessions this year:
“Multi-Timescale Interactions of Glucose and Insulin in Type 1 Diabetes Reveal Benefits of Hybrid Closed Loop Systems“ (poster 99-LB) along with Azure Grant and Lance Kriegsfeld, PhD.
“Do-It-Yourself Artificial Pancreas Systems for Type 1 Diabetes Reduce Hyperglycemia Without Increasing Hypoglycemia” (poster 988-P in category 12-D Clinical Therapeutics/New Technology—Insulin Delivery Systems), alongside Jennifer Zabinsky, MD MEng, Haley Howell, MSHI, Alireza Ghezavati, MD, Andrew Nguyen, PhD, and Jenise Wong, MD PhD.
And, while not a poster at ADA, I also presented the “AID-IRL” study funded by DiabetesMine at #DData20, held in conjunction with Scientific Sessions. A summary of the study is also included in this post.
—
First up, the biological rhythms poster, “Multi-Timescale Interactions of Glucose and Insulin in Type 1 Diabetes Reveal Benefits of Hybrid Closed Loop Systems” (poster 99-LB). (Twitter thread summary of this poster here.)
Building off our work as detailed last year, Azure, Lance, and I have been exploring the biological rhythms in individuals living with type 1 diabetes. Why? It’s not been done before, and we now have the capabilities thanks to technology (pumps, CGM, and closed loops) to better understand how glucose and insulin dynamics may be similar or different than those without diabetes.
Background:
Blood glucose and insulin exhibit coupled biological rhythms at multiple timescales, including hours (ultradian, UR) and the day (circadian, CR) in individuals without diabetes. The presence and stability of these rhythms are associated with healthy glucose control in individuals without diabetes. (See right, adapted from Mejean et al., 1988).
However, biological rhythms in longitudinal (e.g., months to years) data sets of glucose and insulin outputs have not been mapped in a wide population of people with Type 1 Diabetes (PWT1D). It is not known how glucose and insulin rhythms compare between T1D and non-T1D individuals. It is also unknown if rhythms in T1D are affected by type of therapy, such as Sensor Augmented Pump (SAP) vs. Hybrid Closed Loop (HCL). As HCL systems permit feedback from a CGM to automatically adjust insulin delivery, we hypothesized that rhythmicity and glycemia would exhibit improvements in HCL users compared to SAP users. We describe longitudinal temporal structure in glucose and insulin delivery rate of individuals with T1D using SAP or HCL systems in comparison to glucose levels from a subset of individuals without diabetes.
Data collection and analysis:
We assessed stability and amplitude of normalized continuous glucose and insulin rate oscillations using the continuous wavelet transformation and wavelet coherence. Data came from 16 non-T1D individuals (CGM only, >2 weeks per individual) from the Quantified Self CGM dataset and 200 (n = 100 HCL, n = 100 SAP; >3 months per individual) individuals from the Tidepool Big Data Donation Project. Morlet wavelets were used for all analyses. Data were analyzed and plotted using Matlab 2020a and Python 3 in conjunction with in-house code for wavelet decomposition modified from the “Jlab” toolbox, from code developed by Dr. Tanya Leise (Leise 2013), and from the Wavelet Coherence toolkit by Dr. Xu Cui. Linear regression was used to generate correlations, and paired t-tests were used to compare AUC for wavelet and wavelet coherences by group (df=100). Stats used 1 point per individual per day.
Wavelets Assess Glucose and Insulin Rhythms and Interactions
Morlet wavelets (A) estimate rhythmic strength in glucose or insulin data at each minute in time (a combination of signal amplitude and oscillation stability) by assessing the fit of a wavelet stretched in window and in the x and y dimensions to a signal (B). The output (C) is a matrix of wavelet power, periodicity, and time (days). Transform of example HCL data illustrate the presence of predominantly circadian power in glucose, and predominantly 1-6 h ultradian power in insulin. Color map indicates wavelet power (synonymous with Y axis height). Wavelet coherence (D) enables assessment of rhythmic interactions between glucose and insulin; here, glucose and insulin rhythms are highly correlated at the 3-6 (ultradian) and 24 (circadian) hour timescales.
Results:
Hybrid Closed Loop Systems Reduce Hyperglycemia
A) Proportional counts* of glucose distributions of all individuals with T1D using SAP (n=100) and HCL (n=100) systems. SAP system users exhibit a broader, right shifted distribution in comparison to individuals using HCL systems, indicating greater hyperglycemia (>7.8 mmol/L). Hypoglycemic events (<4mmol/L) comprised <5% of all data points for either T1D dataset.
B) Proportional counts* of non-T1D glucose distributions. Although limited in number, our dataset from people without diabetes exhibits a tighter blood glucose distribution, with the vast majority of values falling in euglycemic range (n=16 non-T1D individuals).
C) Median distributions for each dataset.
*Counts are scaled such that each individual contributes the same proportion of total data per bin.
HCL Improves Correlation of Glucose-Insulin Level & Rhythm
SAP users exhibit uncorrelated glucose and insulin levels (A) (r2 =3.3*10-5; p=0.341) and uncorrelated URs of glucose and insulin (B) (r2 =1.17*10-3; p=0.165). Glucose and its rhythms take a wide spectrum of values for each of the standard doses of insulin rates provided by the pump, leading to the striped appearance (B). By contrast, Hybrid Closed Loop users exhibit correlated glucose and insulin levels (C) (r2 =0.02; p=7.63*10-16), and correlated ultradian rhythms of glucose and insulin (D) (r2 =-0.13; p=5.22*10-38). Overlays (E,F).
A) Circadian (blue) and 3-6 hour ultradian (maroon) coherence of glucose and insulin in HCL (solid) and SAP (dotted) users. Transparent shading indicates standard deviation. Although both HCL and SAP individuals have lower coherence than would be expected in a non-T1D individual, HCL CR and UR coherence are significantly greater than SAP CR and UR coherence (paired t-test p= 1.51*10-7 t=-5.77 and p= 5.01*10-14 t=-9.19, respectively). This brings HCL users’ glucose and insulin closer to the canonical non-T1D phenotype than SAP users’.
B) Additionally, the amplitude of HCL users’ glucose CRs and URs (solid) is closer (smaller) to that of non-T1D (dashed) individuals than are SAP glucose rhythms (dotted). SAP CR and UR amplitude is significantly higher than that of HCL or non-T1D (T-test,1,98, p= 47*10-17 and p= 5.95*10-20, respectively), but HCL CR amplitude is not significantly different from non-T1D CR amplitude (p=0.61).
Together, HCL users are more similar than SAP users to the canonical Non-T1D phenotype in A) rhythmic interaction between glucose and insulin and B) glucose rhythmic amplitude.
Conclusions and Future Directions
T1D and non-T1D individuals exhibit different relative stabilities of within-a-day rhythms and daily rhythms in blood glucose, and T1D glucose and insulin delivery rhythmic patterns differ by insulin delivery system.
Hybrid Closed Looping is Associated With:
Lower incidence of hyperglycemia
Greater correlation between glucose level and insulin delivery rate
Greater correlation between ultradian glucose and ultradian insulin delivery rhythms
Greater degree of circadian and ultradian coherence between glucose and insulin delivery rate than in SAP system use
Lower amplitude swings at the circadian and ultradian timescale
These preliminary results suggest that HCL recapitulates non-diabetes glucose-insulin dynamics to a greater degree than SAP. However, pump model, bolusing data, looping algorithms and insulin type likely all affect rhythmic structure and will need to be further differentiated. Future work will determine if stability of rhythmic structure is associated with greater time in range, which will help determine if bolstering of within-a-day and daily rhythmic structure is truly beneficial to PWT1D. Acknowledgements:
Thanks to all of the individuals who donated their data as part of the Tidepool Big Data Donation Project, as well as the OpenAPS Data Commons, from which data is also being used in other areas of this study. This study is supported by JDRF (1-SRA-2019-821-S-B).
(You can download a full PDF copy of the poster here.)
—
Next is “Do-It-Yourself Artificial Pancreas Systems for Type 1 Diabetes Reduce Hyperglycemia Without Increasing Hypoglycemia” (poster 988-P in category 12-D Clinical Therapeutics/New Technology—Insulin Delivery Systems), which I co-authored alongside Jennifer Zabinsky, MD MEng, Haley Howell, MSHI, Alireza Ghezavati, MD, Andrew Nguyen, PhD, and Jenise Wong, MD PhD. There is a Twitter thread summarizing this poster here.
This was a retrospective double cohort study that evaluated data from the OpenAPS Data Commons (data ranged from 2017-2019) and compared it to conventional sensor-augmented pump (SAP) therapy from the Tidepool Big Data Donation Project.
Methods:
From the OpenAPS Data Commons, one month of CGM data (with more than 70% of the month spent using CGM), as long as they were >1 year of living with T1D, was used. People could be using any type of DIYAPS (OpenAPS, Loop, or AndroidAPS) and there were no age restrictions.
A random age-matched sample from the Tidepool Big Data Donation Project of people with type 1 diabetes with SAP was selected.
The primary outcome assessed was percent of CGM data <70 mg/dL.
The secondary outcomes assessed were # of hypoglycemic events per month (15 minutes or more <70 mg/dL); percent of time in range (70-180mg/dL); percent of time above range (>180mg/dL), mean CGM values, and coefficient of variation.
Demographics:
From Table 1, this shows the age of participants was not statistically different between the DIYAPS and SAP cohorts. Similarly, the age at T1D diagnosis or time since T1D diagnosis did not differ.
Table 2 shows the additional characteristics of the DIYAPS cohort, which included data shared by a parent/caregiver for their child with T1D. DIYAPS use was an average of 7 months, at the time of the month of CGM used for the study. The self-reported HbA1c in DIYAPS was 6.4%.
Results:
Figure 1 shows the comparison in outcomes based on CGM data between the two groups. Asterisks (*) indicate statistical significance.
There was no statistically significant difference in % of CGM values below 70mg/dL between the groups in this data set sampled.
DIYAPS users had higher percent in target range and lower percent in hyperglycemic range, compared to the SAP users.
Table 3 shows the secondary outcomes.
There was no statistically significant difference in the average number of hypoglycemic events per month between the 2 groups.
The mean CGM glucose value was lower for the DIYAPS group, but the coefficient of variation did not differ between groups.
Conclusions:
Users of DIYAPS (from this month of sampled data) had a comparable amount of hypoglycemia to those using SAP.
Mean CGM glucose and frequency of hyperglycemia were lower in the DIYAPS group.
Percent of CGM values in target range (70-180mg/dL) was significantly greater for DIYAPS users.
This shows a benefit in DIYAPS in reducing hyperglycemia without compromising a low occurrence of hypoglycemia.
Finally, my presentation at this year’s D-Data conference (#DData20). The study I presented, called AID-IRL, was funded by Diabetes Mine. You can see a Twitter thread summarizing my AID-IRL presentation here.
I did semi-structured phone interviews with 7 users of commercial AID systems in the last few months. The study was funded by DiabetesMine – both for my time in conducting the study, as well as funding for study participants. Study participants received $50 for their participation. I sought a mix of longer-time and newer AID users, using a mix of systems. Control-IQ (4) and 670G (2) users were interviewed; as well as (1) a CamAPS FX user since it was approved in the UK during the time of the study.
Based on the interviews, I coded their feedback for each of the different themes of the study depending on whether they saw improvements (or did not have issues); had no changes but were satisfied, or neutral experiences; or saw negative impact/experience. For each participant, I reviewed their experience and what they were happy with or frustrated by.
Here are some of the details for each participant.
1 – A parent of a child using Control-IQ (off-label), with 30% increase in TIR with no increased hypoglycemia. They spend less time correcting than before; less time thinking about diabetes; and “get solid uninterrupted sleep for the first time since diagnosis”. They wish they had remote bolusing, more system information available in remote monitoring on phones. They miss using the system during the 2 hour CGM warmup, and found the system dealt well with growth spurt hormones but not as well with underestimated meals.
2 – An adult male with T1D who previously used DIYAPS saw 5-10% decrease in TIR (but it’s on par with other participants’ TIR) with Control-IQ, and is very pleased by the all-in-one convenience of his commercial system.He misses autosensitivity (a short-term learning feature of how insulin needs may very from base settings) from DIYAPS and has stopped eating breakfast, since he found it couldn’t manage that well. He is doing more manual corrections than he was before.
5 – An adult female with LADA started, stopped, and started using Control-IQ, getting the same TIR that she had before on Basal-IQ. It took artificially inflating settings to achieve these similar results. She likes peace of mind to sleep while the system prevents hypoglycemia. She is frustrated by ‘too high’ target; not having low prevention if she disables Control-IQ; and how much she had to inflate settings to achieve her outcomes. It’s hard to know how much insulin the system gives each hour (she still produces some of own insulin).
7 – An adult female with T1D who frequently has to take steroids for other reasons, causing increased BGs. With Control-IQ, she sees 70% increase in TIR overall and increased TIR overnight, and found it does a ‘decent job keeping up’ with steroid-induced highs. She also wants to run ‘tighter’ and have an adjustable target, and does not ever run in sleep mode so that she can always get the bolus corrections that are more likely to bring her closer to target.
3 – An adult male with T1D using 670G for 3 years didn’t observe any changes to A1c or TIR, but is pleased with his outcomes, especially with the ability to handle his activity levels by using the higher activity target. He is frustrated by the CGM and is woken up 1-2x a week to calibrate overnight. He wishes he could still have low glucose suspend even if he’s kicked out of automode due to calibration issues. He also commented on post-meal highs and more manual interventions.
6 – Another adult male user with 670G was originally diagnosed with T2 (now considered T1) with a very high total daily insulin use that was able to decrease significantly when switching to AID. He’s happy with increased TIR and less hypo, plus decreased TDD. Due to #COVID19, he did virtually training but would have preferred in-person. He has 4-5 alerts/day and is woken up every other night due to BG alarms or calibration. He does not like the time it takes to charge CGM transmitter, in addition to sensor warmup.
4 – The last participant is an adult male with T1 who previously used DIYAPS but was able to test-drive the CamAPS FX. He saw no TIR change to DIYAPS (which pleased him) and thought the learning curve was easy – but he had to learn the system and let it learn him. He experienced ‘too much’ hypoglycemia (~7% <70mg/dL, 2x his previous), and found it challenging to not have visibility of IOB. He also found the in-app CGM alarms annoying. He noted the system may work better for people with regular routines.
You can see a summary of the participants’ experiences via this chart. Overall, most cited increased or same TIR. Some individuals saw reduced hypos, but a few saw increases. Post-meal highs were commonly mentioned.
Those newer to CGM have a noticeable learning curve and were more likely to comment on number of alarms and system alerts they saw. The 670G users were more likely to describe connection/troubleshooting issues and CGM calibration issues, both of which impacted sleep.
This view highlights those who more recently adopted AID systems. One noted their learning experience was ‘eased’ by “lurking” in the DIY community, and previously participating in an AID study. One felt the learning curve was high. Another struggled with CGM.
Both previous DIYAPS users who were using commercial AID systems referenced the convenience factor of commercial systems. One DIYAPS saw decreased TIR, and has also altered his behaviors accordingly, while the other saw no change to TIR but had increased hypo’s.
Companies building AID systems for PWDs should consider that the onboarding and learning curve may vary for individuals, especially those newer to CGM. Many want better displays of IOB and the ability to adjust targets. Remote bolusing and remote monitoring is highly desired by all, regardless of age. Post-prandial was frequently mentioned as the weak point in glycemic control of commercial AID systems. Even with ‘ideal’ TIR, many commercial users still are doing frequent manual corrections outside of mealtimes.This is an area of improvement for commercial AID to further reduce the burden of managing diabetes.
Note – all studies have their limitations. This was a small deep-dive study that is not necessarily representative, due to the design and small sample size. Timing of system availability influenced the ability to have new/longer time users.
Thank you to all of the participants of the study for sharing their feedback about their experiences with AID-IRL!
(You can download a PDF of my slides from the AID-IRL study here.)
—
Have questions about any of my posters or presentations? You can always reach me via email at Dana@OpenAPS.org.
Tl;dr – I wrote a book about artificial pancreas systems / hybrid and fully closed loop systems / automated insulin delivery systems! It’s out today – you can buy a print copy on Amazon; a Kindle copy on Amazon; check out all the content on the web or your phone here; or download a PDF if you prefer.
A few months ago, I saw someone share a link to one of my old blog posts with someone else on Facebook. Quite old in fact – I had written it 5+ years ago! But the content was and is still relevant today.
It made me wonder – how could we as a diabetes community, who have been innovating and exploring new diabetes technology such as closed loop/artificial pancreas systems (APS), package up some of this knowledge and share it with people who are newer to APS? And while yes, much of this is tucked into the documentation for DIY closed loop systems, not everyone will choose a DIY closed loop system and also therefore may not see or find this information. And with regards to some of the things I’ve written here on DIYPS.org, not everyone will be lucky enough to have the right combination of search terms to end up on a particular post to answer their question.
Thus, the idea for a book was born. I wanted to take much of what I’ve been writing here, sharing on Facebook and Twitter, and seeing others discuss as well, and put it together in one place to be a good starting place for someone to learn about APS in general. My hope is that it’s more accessible for people who don’t know what “DIY” or “open source” diabetes is, and it’s findable by people who also don’t know or don’t consider themselves to be part of the “diabetes online community”.
Is it perfect? Absolutely not! But, like most of the things in the DIY community…the book is open source. Seriously. Here’s the repository on Github! If you see a typo or have suggestions of content to add, you can make a PR (pull request) or log an issue with content recommendations. (There’s instructions on the book page here with how to do either of those things!) I plan to make rolling updates to it, so you can see on the change log page what’s changed between major versions.)
It’s the first book out there that I know of on APS, but it won’t be the only one. I hope this inspires or moves more people to share their knowledge, through blogs or podcasts or future books, with the rest of our community and loved ones who want and need to learn more about managing type 1 diabetes.
“I will immediately recommend this book not just to people looking to use a DIY closed loop system, but also to anybody looking to improve their grasp on the management of type 1 diabetes, whether patient, caregiver, or healthcare provider.”
– Aaron Neinstein, MD Endocrinologist, UCSF
And as always, I’m happy to share what I’ve learned about the self-publishing process, too. I previously used CreateSpace for my children’s books, which got merged with Amazon’s Kindle Direct Publishing (KDP), and there was a learning curve for KDP for both doing the print version and doing the Kindle version. I didn’t get paid to write this book – and I didn’t write it for a profit. Like my children’s books, I plan to use any proceeds to donate copies to libraries and hospitals, and send any remaining funds to Life For A Child to help ensure as many kids as possible have access to insulin, BG monitoring supplies, and education.
I’m incredibly grateful for many people for helping out with and contributing to this book. You can see the full acknowledgement section with my immense thanks to the many reviewers of early versions of the book! And ditto for the people who shared their stories and experiences with APS. But special thanks go in particular to Scott for thorough first editing and overall support of every project I bring up out of the blue; to Tim Gunn for beautiful cover design of the book; and to Aaron Kowalski to be kind enough to write this amazing foreword.
As I wrote in a previous post with much more detail (see here), I fell off a mountain and broke my ankle in three places, then managed to break a bone in my 5th toe on the other foot. This meant that my right ankle was in a hard cast for 6 weeks and I was 100% non-weight bearing…but this was challenging because the foot meant to be my stable base for crutching or knee scootering was often pretty wobbly and in a lot of pain.
This post is a follow up with more detailed tips and lessons learned of things that were helpful in living with a leg cast, as well as what the return to weight bearing was really like. I couldn’t find a lot of good information about the transition to weight bearing was really like, so this is my take on information I was looking for and would have appreciated before and during the weight bearing progression process. (And if you’re looking for diabetes-specific stuff, it’s in the last section!) Dealing with lack of energy and fatigue
First, it’s worth noting something major about a fractured bone, and *especially* true if it’s a big bone fracture like some of mine were: it takes a lot of healing, which means a lot of energy going to the healing and not much energy left for every day living. I was constantly exhausted – and surprised by this fatigue – pretty much throughout this process. It made sense in the early days (say weeks 1-2 after fracture), but was frustrating to me how little I had energy to do even in the 4-6 weeks after my fracture.
But, then it got worse. Returning to weight bearing took *even more* energy. For example, on the first day of partial weight bearing, I was tasked with putting 25 lbs of weight on my foot in the walking boot. First by placing my foot on the scale and getting reliable with being able to put the right amount of weight on the boot; then by standing and repeating with the scale; then taking a few steps (with the crutches taking the rest of my weight) and re-calibrating with the scale until I was confident in that weight. With weight bearing progression, you’re supposed to spend up to an hour a day working on this.
I took to heart what my ortho said about not progressing fast if you only do 5-10 minute chunks, so after the first day, I tried to always do 10-15 minute chunks at a minimum, with a longer chunk wherever possible as permitted by pain and my energy levels.
But the first few days were really, really tough. It was hard to switch to a new weight every two days – because this meant readjusting how I was stepping/walking, and how much weight and where I placed my crutches. I started with a blister on my right palm, which turned into a squished nerve that made my right hand go numb, and ultimately damaged some tendons in my right wrist, too. This made it painful to use the crutches or even drive my knee scooter when I wasn’t focusing on weight bearing. So I had a lot of pain and suffering in the WB progression process that probably contributed to how fatigued I was overall.
So one of my biggest pieces of advice for anyone with broken bones is to expect your energy to take a(nother) dip for the first few weeks after you start returning to weight-bearing (or return to normal activity outside your cast). It’s a *lot* of work to regain strength in atrophied muscles while still also doing the internal healing on the broken bones!
Tips to deal with so much fatigue as you return to weight bearing:
Some of the tips and things I figured out for being non-weight bearing and sitting around with a hard cast came in handy for the weight-bearing progression fatigue, too.
I got a shower bench (this is the one I got) so that it was easy to sit down on and swing my legs over into the shower/bathtub. Once I was out of my hard cast, I still can’t weight bear without the boot, so I still need a sitting shower/bath solution while I return to weight bearing. I also removed the back after a while, so it was easier to sit in either direction depending on preference (washing hair/not) without having to ask Scott to remove the back and re-attach it on the other side.
Speaking of showers, I put a toothbrush and toothpaste in the shower so I can also brush my teeth there while seated.
I still keep most of my toiletries in the bedside table (or you could have a caddy by the bedside) so I can brush my hair, take my contacts out or put them in, wipe my face (facewipes instead of having to stand at the sink to wash my face), etc. from the bed.
I am taking ibuprofen 4x a day, and I get tired of opening the bottle. So I dumped a pile of ibuprofen on my bedside table to make it easy to reach and remember to take first thing in the morning or at night. (There are no kids or pets in my household; keep safety in mind if you have kids etc in your household – this solution may not work for you).
The one time I tended to forget to proactively take my medication was mid-day, so I added a recurring calendar event to my calendar saying “take ibuprofen if you haven’t 2x a day” around 2pm, which would be the latest I would take my second round, even if I woke up later in the day and my first dose was later in the morning. This has helped me remember multiple times, especially on weekends or times when I’m away from my desk or bed where I would have the meds visible as a reminder.
Pre-mix protein powder (this is what I chose) into the beverage of choice in advance, and keep it in individual containers so it’s easy to get and take (and if I’m really tired, round tupperware containers that have measurement lines make it easy to measure liquid into, put the lid on to shake it up, and drink out of without having to find another cup). I had Scott do this several days in advance when he went on a trip, and we kept doing it in advance even after he got home.
I kept using my portable desk for working, taking video calls propped up in the bed with pillows behind me, and also laying the surface flat to eat meals from when I was too tired to get out of the bed.
Other advice for the return to weight-bearing:
If you’re like me, you’ll switch back to weight-bearing accompanied by getting out of your hard cast and getting a walking boot of some sort. If you can, ask your ortho/doc in advance what kind of boot they’ll put you in. It’s often cheaper to get the boot yourself. Perfect example: my ortho didn’t tell me what kind of boot I would need, and I looked at various boots online and saw they ranged $50-100 on Amazon. At my appointment he asked if I brought a boot and since I didn’t, they’d provide one..and the paperwork I signed stated the price would be $427 (::choking::) if the insurance didn’t cover it. Insurance negotiated down to $152 for me to pay out of pocket for since I haven’t hit my deductible…which is still 2-3x more than retail cost. UGH. So, if you can, buy your walking boot via retail. (Same goes for purchasing a knee scooter (here’s the one I got) – it may be cheaper to buy it new through Amazon/elsewhere than getting a medical purchase that goes through insurance and/or trying to do a rental.)
You’ll also probably end up with a boot with lots of velcro straps. When you undo your boot, fold back the strap on itself so it doesn’t stick to the boot, another strap, your clothes, etc.
Other equipment that has come in handy:
Get multiple ankle braces. I had a slightly structured ankle brace with hard sides that made me feel safer the first few nights sleeping out of the cast, and it was often easier to go from the bed to the bathroom on my knee scooter or crutches with the ankle brace(s) instead of re-putting on my walking boot and taking it off again for a shower. (I transitioned to sleeping in a lighter ankle brace after a week or so, but still used the structured brace inside the waterproof cast bag for swimming laps to help protect my ankle.)
An ice pack with a strap to put around your ankle/broken joint. I had gotten this ice pack for my knee last fall, and strap it and another ice pack to my ankle to get full joint coverage.
Wide leg athletic pants…ideally ones that you can put on/off without having to take your boot off. (Women should note I found better athletic pants for this purpose in the men’s athletic section at Target..but be aware a lot of the modern men’s style have tapered legs so make sure to watch out for those and have enough width to get over your boot). Taking off the boot is exhausting with so many velcro straps, so any time I can get dressed or undressed without having to remove the boot if I am not otherwise removing the boot is a win.
Look online for your state’s rules for a temporary handicap parking pass, and take the paperwork to your first ortho appointment to get filled out. Also, make sure to note where the places are that you can drop off the paperwork in person (in Seattle it was not the same as the DMV offices!), or otherwise be aware of the time frame for mailing those in and receiving the pass. The handicap parking placard has been helpful for encouraging me to get out of the house more to go to the store or go to a restaurant when otherwise I’m too exhausted to do anything.
A new shiny notebook for writing down your daily activities and what you did. If you’re not a notebook type person, use an app or note on your phone. But despite being mostly digital, I liked having a small notebook by the bed to list my daily activities and check the box on them to emphasize the activities I was doing and the progress I was making. At the beginning, it was helpful for keeping track of all the new things I needed to do; in the middle, it was useful for emphasizing the progress I was making; and at the end it felt really good to see the light of the end of the tunnel of a few pages/days left toward being fully weight bearing.
Other tips for getting used to a walking boot and transitioning to weight bearing:
Don’t be surprised if you have pain in new areas when you move from a hard cast to a walking boot. (Remember you’ll be moving your leg or limbs in different ways than they’ve been accustomed to).
My ortho told me the goal of weight bearing progression is to understand the difference between discomfort (lasts a few minutes) and pain (lasts a few hours). You’re likely going to be in discomfort when doing weight bearing progression – that’s normal. Pain (i.e. sharp pain) is not normal, and you should take a break or back down to a previous weight (follow your protocol) if you have it. I was lucky – the only few times I had pain was from trying to press down forcefully on the scale when seated, rather than standing on the scale and naturally letting my weight on my leg. I didn’t end up plateauing at any weight, and was able to follow my protocol of 25lb weight bearing added every 2 days and get to full weight bearing with no delays.
If you have a watch with a stopwatch feature, use it. It’s hard to keep track of actual time spent walking (especially at first when 90 seconds feels like 6 minutes) with just a normal watch/clock. You could also use your smartphone’s timer feature. But tracking the time and pausing when you pause or take a break helps make sure you’re accurately tracking toward your hour of walking.
The process wasn’t without discomfort – physical and emotional. Putting weight on my leg was scary, and every new weight day was hard as I dealt with the fear and processing of the discomfort, as well as learning how to step and walk and do my crutches in a new way yet again.
But what I learned is that the first 5 minutes of every new weight day ALWAYS sucked. Once I recognized this, I set the goal to always tough out a 15 minute session after I calibrated on the scale by walking slowly around my apartment. (I put my headphones in to listen to music while I did it). As long as there was only discomfort and not pain, I didn’t stop until after 15 minutes of slow walking with that weight and also re-calibrated on the scale during and after to make sure I was in the right ballpark.
I had to spend the first half hour or so working on my weight bearing by myself. I couldn’t talk on the phone or talk with Scott while I did it; it required a lot of concentration. (The only thing I could do is listen to music, because I’m used to running with music). So distractions did not help when I got started, but toward the end of the hour I could handle and appreciate distractions. Same for day 2 of a weight – having distractions or a task to do (e.g. walk from A to B, or walking while my nephew was on his scooter) helped pass the time and get me to complete my hour or more of weight-bearing work.
Be careful with your hands and wrists. Blisters are common, and I managed to both squish a nerve (which caused me to have a numb side of my hand and be unable to type for several days) and also pull or damage tendons on both sides of my wrists. I was torn between choosing to delay my weight bearing progression work, but also recognizing that the sooner I got to full weight bearing the sooner I could completely ditch my crutches and be done hurting my hands. So I chose to continue, but in some cases shortened my chunks of WB walking down to 15 minutes wherever possible to reduce the pain and pressure on my hands.
You’ll likely also be doing range of motion exercises. At first, it’s scary how jerky your motions may be and how little your muscles and tendons respond to your brain’s commands. One thing I did was take a video on day 1 showing me pointing and stretching my ankle, and doing my ABC’s with my foot. Then every week or so when I was feeling down and frustrated about how my ankle wasn’t fully mobile yet, I’d take another video and watch the old one to compare. I was able to see progress every few days in terms of being able to point my foot more, and wider motions for doing the ABC’s with my foot.
Also remember, once you’re weight bearing and working toward getting rid of your crutches, you can use things like strollers or grocery carts to help you balance (and also kill some of your weight bearing time!) without crutches. The practice will make it easier for re-learning your posture and gaining confidence in walking without crutches.
Don’t you usually talk about diabetes stuff on this blog? 😉
(If anyone finds this post in the future mainly for ankle fracture and weight bearing transition/progression tips, you can ignore this part!)
It was common for my first few days of progressive weight bearing to have a small pain/stress rise in my BGs. It wasn’t much, but 20-30 points was an obvious stress response as I did the first few 15 minutes of weight bearing practice. The following days didn’t see this, so my body was obviously getting used to the stress of weight bearing again.
However, on the flip side, the first week of weight bearing progression also caused several lows. The hour of walking was the equivalent of any new activity where I usually have several hours later delayed sensitivity to insulin out of nowhere, and my blood sugars “go whoosh” – dropping far more than they normally would. I had two nights in a row in the first week where I woke up 2-3 hours after I went to sleep and needed to eat some carbs. This normally happens maybe once every few months (if that) now as an OpenAPS user, so it was obviously associated with this new surge of physical activity and hard work that I was doing for the weight bearing.
Overall, while I was 100% non-weight bearing, I was eating slightly (but not much) lower carb and slightly less processed food than I usually do. But not always. One day I ended up having 205+ grams of carbs for me (quite a bit more than my average). However, thanks to #OpenAPS, I still managed to have a 100% in range day (80-150 mg/dL). Similarly on a travel day soon after, I ate a lot less (<50g carb) and also had a great day where OpenAPS took care of any surges and dips automatically – and more importantly, without any extra work and energy on my part. Having OpenAPS during the broken bone recovery has been a HUGE benefit, not only for keeping my BGs in range so much of the time for optimal healing, but also for significantly reducing the amount of work and cognitive burden it takes to stay alive with type 1 diabetes in general. I barely had energy to eat and do my hour of weight bearing each day, let alone anything else. Thankfully good BGs didn’t fall by the wayside, but without this tech it certainly would have.
And finally the pep talk I gave myself every day during weight bearing progression work:
This is short-term and necessary discomfort and suffering on the way to weight bearing. It sucks, but you can and will do it. You have to do it. If you need to take a break, take a break. If you need to do something else to get yourself pumped up and motivated to do your weight bearing, it’s ok to do that. But you’ll get there. Slowly, but surely. You’ve got this!
Proof that I did get there:
—
Best of luck and lots of support and encouragement to anyone who’s working their way to weight bearing after an injury, and many thanks to everyone who’s supported me and cheered me on virtually along the way!
2021 update – see this post about (finally) running the marathon that I had signed up for before I broke my ankle!
This is a polite, and seemingly innocuous question. However, it’s one of my least favorite questions taken at face value. Why?
Well, this question is often a proxy for some of the following questions:
How well are *you* doing with DIY closed loop technology?
How well could *I* possibly do with DIY closed loop technology?
What’s possible to achieve in real-world life with type 1 diabetes?
But if I answered this question directly with “X.x%”, it leaves out so much crucial information. Such as:
What my BG targets are
Because with DIY closed loop tech like OpenAPS, you can choose and set your own target.
(That’s also one of the reasons why the 2018 OpenAPS Outcomes Study is fascinating to me, because people usually set high, conservative targets to start and then gradually lower them as they get comfortable. However, we didn’t have a way to retrospectively sleuth out targets, so those are results are even with the amalgamation of people’s targets being at any point they wanted at any time.)
What type of lifestyle I live
I don’t consider myself to eat particularly “high” or “low” carb. (And don’t start at me about why you choose to eat X amount of carbs – you do you! and YDMV) Someone who *is* eating a lot higher or lower carb diet compared to mine, though, may have a different experience than me.
Someone who is not doing exercise or activity may also have a different experience then me with variability in BGs. Sometimes I’m super active, climbing mountains (and falling off of them..more detail about that here) and running marathons and swimming or scuba diving, and sometimes I’m not. That activity is not so much about “being healthy”, but a point about how exercise and activity can actually make it a lot harder to manage BGs, both due to the volatility of the activity on insulin sensitivity etc.; but also because of the factor of going on/off of insulin for a period of time (because my pump is not waterproof).
I use most of the advanced settings, such as “superMicroBoluses” (aka SMB – read more about how it works here); with a higher than default “maxSMBBasalMinutes”; and I also use all of the advanced exercise settings so that targets also nudge sensitivity in addition to autosensitivity picking up any changes after exercise and other sensitivity-change-inducing activities or events. I also get Pushover alerts to tell me if I need any carbs (and how many), if I’m dropping faster and expected to go below my target, even with zero temping all the way down.
What my behavioral choices are
Timing of insulin matters. As I learned almost 5 years ago (wow), the impact of insulin timing compared to food *really* matters. Some people still are able to do and manage well with “pre-bolusing”. I don’t (as explained there in the previous link). But “eating soon” mode does help a lot for managing post-meal spikes (see here a quick and easy visual for how to do “eating soon”). However, I don’t do “eating soon” regularly like I used to. In part, because I’m now on a slightly-faster insulin that peaks in 45 minutes. I still get better outcomes when I do an eating-soon, sure, but behaviorally it’s less necessary.
(The exceptions being if I’m not looping for some reason, such as I’m in the middle of switching CGM sensors and don’t have CGM data to loop off of.)
These settings and choices are all crucial information to understanding the X.x% of A1c.
Diabetes isn’t just the average blood glucose value. It’s not just the standard deviation or coefficient of variation or % time in range or how much BG fluctuates.
Diabetes impacts so much of our daily life and requires so much cognitive burden for us, and our loved ones. That’s part of the reasons I appreciate so much Sulka & his family being candid about how their A1C didn’t change, but the amount of work required to achieve it did (way fewer manual corrections). And ditto for Jason & the Wittmer family for sharing about the change in the number of school nurse visits before/after using OpenAPS. (See both of their stories in this post)
For me, my quality of life metric has always been first about sleep: can I sleep safely and with peace of mind at night? Yes. Then – how long can I safely sleep? (The answer: a lot. Yay!) But over time, my metrics have also evolved to consider how I can cut down (like Sulka) on the amount of work it takes to achieve my ideal outcomes, and find a happy balance there.
As I mentioned in this podcast recently, other than changing my pump site (here’s how I change mine) and soaking and swapping my CGM sensors (psst – soak your sensor!), I usually only take a few diabetes-related actions a day. They’re usually on my watch, pressing a button to either enable a temp target or entering carbs when I sit down to eat.
That’s a huge reduction in physical work, as well as amount of time spent thinking/planning/doing diabetes-related things. And when life happens – because I get the flu or the norovirus or I fall off a mountain and break my ankle – I don’t worry about diabetes any more.
So when I’m asked about A1c, my answer is not a simple “X.x%”. (And not just for the reason I’m annoyed by how much judging and shaming goes on around A1c, although that influences it, too.) I usually remind people that I first started with an “open loop” for a year, and that dropped my A1c by X%. And then I closed the loop, which reduced my A1c further. And we made OpenAPS even better over the last four years, which reduced it further. And then I completely stopped bolusing! And got less lows…and kept the same A1c.
And then I ask them what they’d really like to know. If it’s a fellow person with diabetes or a loved one, we talk about what problems they might be having or what areas they’d like to improve or what behaviors they’d like to change, if any. That’s usually way more effective than hearing “X.x%” of an A1c, and them wondering silently how to get there or what to do differently if someone wants to change things. (Or for clinicians who ask me, it turns into a discussion about choices and behaviors and tradeoffs that patients may choose to make.)
Remember, your diabetes may (and will) vary (aka, YDMV). Your lifestyle, the phase of life you’re in, your priorities, your body and health, and your choices will ALL be different than mine. That’s not bad in any way: that’s just the way it is. The behaviors I choose and the work I’m willing to do (or not do) to achieve *my* goals (and what my goals are), will be different than what you choose for yours.
And that’s therefore why A1c is not “enough” to me as a metric and something that we should compare people on, even though A1c is the “same” for everyone: because the work, time spent, behavioral tradeoffs, and goals related to it will all vary.
In January, Scott and I planned and went on a three day hiking trip in New Zealand. NZ is famous for “tramping” and “trekking”, and since we were in the country for a conference (you can see my talk at LinuxConfAU here!), we decided to give it a try. This was my first true “backpacking” type trip where you carry all your stuff on your back; and the first multi-day hiking experience. You could either rent a cot in a hut and carry all your food and cooking utensils and bedding on your back; or you could pay to hike with a company who has a lodge you can stay at (with hot showers and amazing food) and also has guides who hike with your pack. They had me at “gluten free food” and “hot showers”, so I convinced Scott that was the way we should do our Routeburn Track hike!
I planned ahead well for the hike; they gave us a packing list of recommended things to carry and bring. I learned from a friend in NZ, Martin, who had gone trekking a few weeks prior: his pack went over a cliff and was lost – yikes! Therefore, I planned one set of supplies in baggies and put them in both Scott & my pack just in case something happened to one of our packs, we’d still be completely covered.
Day 1 of the hike was awesome – it was overcast and felt like hiking in Seattle, but the scenery and wildlife were still great to experience. Since it was raining off and on, the waterfalls were spectacular.
Day 2 also started awesome – it was a breathtakingly clear morning with blue skies and sunshine as we hiked up above the tree line and over a mountain ridge, along the valley, and onward toward the lunch spot. I was feeling great and enjoying my hike – this was one of my all-time favorite places to hike in terms of the view of the valley and lake that we hiked from; and the mountain views on the other side of the ridge once we topped the mountain and crossed over.
However, about 30 min from the lunch shelter (and about 300 feet of elevation to go), I noticed the lady hiking in front of us decided to sit and slide down a particularly large and angled rock on the trail. I approached the rock planning to stop and assess my plan before continuing on. Before I even decided what to do, I somehow slipped and vaulted (for lack of a better word) left and off the trail…and down the slope. I flipped over multiple times and knew I had to grab something to stop my flight and be able to save myself from going all the way off the mountain slope. I amazingly only ended up about 10 feet off the trail, clinging to a giant bush/fern-like plant.
I had to be pulled back up to the trail by Scott and another hiker who came running after hearing my yell for help as I went down the mountain. (Scott came down off the trail few feet, and had to hold onto the hand of another hiker with one hand while pulling me up with the other, just like in the movies. It’s not a lot of fun to be at the end of the human chain, though!) At that point, I knew I had injured my right ankle and could only use my left foot/leg and right knee to try to climb back up to the trail while they pulled on my backpack. We got me back on to the trail and over to a rock to rest. We waited a few minutes for the back-of-the-pack guides who showed up and taped around my ankle and boot to see if I could walk on it – they thought it was sprained. I could flex, but couldn’t really put weight on it without excruciatingly sharp pain on the right side. I’d never sprained my foot before or broken any bones in my life, so I was frustrated by how painful the ‘sprain’ was. I had an overwhelming wave of nausea that I knew was in response to the pain, too, so at one point I had to sit there and lean back with my eyes closed while everyone else talked around me.
The guides wanted to see if we could get to a nearby river to ice my leg in. I used my poles as pseudo-crutches in front of me, with my arms bent at 90 degree angles, and with Scott behind me to check my balance, would crutch and hop on one leg. It wasn’t like regular crutching, though, where you can press your weight down on your arms and hands. It was really an act of placing the poles slightly forward for balance and then hopping up and forward, pressing off my left leg. My left leg was quickly exhausted and cramping from the effort of hopping forward with my entire body weight. It was also complicated by the rain making things more slippery; and of course; this is a mountain trail with rocks and boulders of different sizes. What I didn’t even notice walking normally on two feet became incredibly frustrating for figuring out when and how to jump up onto a small rock; or around to the side; etc.
“Lucky” for me (eye roll), we happened to be in an ascending section of the trail with quite a few large rocky sections, and there was no way I could hop up the uneven rocks on foot. So instead, I chose to crawl up and over those sections on my hands and knees. Then I would get up at the top and hop again through the “flatter” gravel and rock sections, then crawl again. It was slow and exhausting, and painful when I would get up one one leg again and start hopping again. I was in the most physical pain I’d ever been in my life.
After about a very slow and painful quarter of a mile, and as rain was dripping down more steadily, the guides decided I wouldn’t make it the remaining 300ft of elevation/30 minute (normal) hike to the lunch spot. They radioed for a medevac helicopter to come pick me up. I was incredibly upset and disappointed that I had ruined our hike… but also knew I absolutely wouldn’t even make it to the lunch shelter. I remember saying “I feel so stupid!” to Scott.
The helicopter came in a surprisingly quick amount of time, and they let out one of the EMT’s nearby and then flew over to a hill across from the trail. The EMT saw that I was decently clothed and covered (I had 3/4 length running pants on; a rain jacket and hood; and had a second rain jacket to cover my legs against the rain and wind) and did a verbal status check to confirm I was decent enough for them to lift me off the mountain. They weren’t able to land safely anywhere nearby on the trail because it was so steep and narrow; so they put me in a “sack” that went around my back and looped over my arms and between my legs, and was hooked on to the EMT’s harness. Scott and the guide stood back, while the helicopter came back and lowered the winch. I was winched up from there. However, the EMT had told me once we got up to the helicopter that the team inside would pull me straight back. And that didn’t happen, which was slightly more terrifying because we started flying away from the mountain while still *outside* the helicopter. It turns out the helicopter had unloaded a stretcher and supplies on the nearby hill, and so we were lowered down – with me and the EMT still perched outside the skids – to the hillside there, so the team could then gather the supplies & then load me in so I could sit on the stretcher.
The other terrifying factor about being evacuated off the mountain was that due to the weather that was blowing in hours ahead of schedule, and the “we have to winch you off the mountain” aspect: they couldn’t take Scott with us. So I had to start making plans & preparing myself for going to the hospital by myself in a foreign country. I was terrified about my BGs & diabetes & how I know hospitals don’t always know what to do with people with T1D, let alone someone on a (DIY) closed loop. I tried to tamp down on my worries & make some plans while we waited for the helicopter, so Scott would know I was okay-ish and worry slightly less about me. But at that point, we knew he would have to finish the day’s hike (another 3-4 hours); spend the night; and hike down the next day as planned in order to meet up with me at the hospital.
As we lifted off in the helicopter, I handed the EMT my phone, where I had made a note with my name, age, medical information (T1D & celiac), and the situation about my ankle. He loved it, because he could just write down my information on the accident forms without yelling over the headset. Once he gave me my phone back, a few minutes later we passed back into an area with signal, and I was able to send text messages for the first time in 2 days.
I sent one to my mom, as carefully worded as I could possibly do:
“Slipped off the trail. Hurt ankle. BGs ok. In a helicopter to the hospital in Queenstown. Just got signal in helicopter. Don’t freak out. Will text or call later. Love you”
It had all the key information – something happened; here’s where I’m heading; BGs are fine; pleeeeeeeease don’t freak out.
I also sent a text to Scott’s dad, Howard, who’s an ER doc, with a tad different description:
“Slipped and flipped off the trail. Possible ankle fracture or serious sprain. Being medevac’d off in a helicopter. BGs are fine. But please stand by for any calls in case I need medical advice. Just got signal in the chopper. Scott is still on the trail until tomorrow so I am solo.”
I was quite nervous when we arrived at the hospital. I haven’t been in an ER since high school (when I was dehydrated from a virus). I’ve heard horror stories about T1D & hospitals. However, most of my fears related to T1D were completely unfounded. When I arrived, the EMT did some more paperwork, I talked briefly to a nurse, and then was left alone for quite a while (maybe an hour). Other than mentioning T1D (and that my BGs were fine) and celiac to the nurse, no one ever asked about my BGs throughout the rest of the time in the ER. Which was fine with me. What my BGs had actually done was rise steadily from about 120 up to 160, then stayed there flat. That’s a bit high, but given I was trying to manage pain and sort out my situation, I was comfortable being slightly elevated in case I crashed/dropped later when the adrenaline came down. I just let OpenAPS keep plugging away.
The first thing that was done in the ER about an hour after I arrived was wheeling me to go get an x-ray. It was quick and not too painful. I remember vividly that the radiologist came back out and and said “yes, your ankle is definitely broken. In two places.” I started at her and thought an expletive or two. But for some reason, that made me feel a lot better: my pain and the experience I had on the mountain was not totally disproportionate to the injury. I relaxed a lot then, and could feel a lot of the stress ebbing away. My BGs started a slow sloping drop down almost immediately, and ended up going from 160 down to 90 where I leveled out nicely and stayed for the next few hours.
After I was wheeled back to my area of the ER, the ER doc showed up. He started asking, “So I heard you hopped and climbed off the mountain?” and then followed up by saying yes, my ankle was broken…in three places.
Me: “WHAT? Did you say ::three::?”
The ER doc said he had already consulted ortho who confirmed I would need surgery. However, it didn’t have to be that night (halleluljah), and they usually waited ’til swelling went down to operate, so I had a choice of doing it in NZ or going home and doing it there. He asked when I was planning to leave: this was Sunday evening now; and we planned to fly out Wednesday morning. I asked if there were any downsides to waiting to do surgery at home; any risk to my long-term health? He said no, because they usually wait ~10 days for the swelling to go down to operate. So I could wait in NZ (me: uhhh, no) or fly home and see someone locally. I was absolutely thrilled I wouldn’t need to operate then and there, and without Scott. I asked for more details so I could get my FIL’s opinion (he concurred, coming home was reasonable), and then confirmed that I liked the plan to cast me; send me on my way; and let me get surgery at home.
It took them another 2 hours to get me to the procedure room and start my cast. This was a small, 6-bed ER. When they finally started my cast, the ER doc had his hands on my ankle holding it up…and another nurse rushed in warning that a critical patient was in route, 5 minutes out. The ER doc and the other nurse looked at each other, said “we can do this by then”, and literally casted me in 2 minutes and were wheeling me out in the third minute! It was a tad amusing. I was taken back to x-ray where they confirmed that the cast was done with my ankle in a good position. After that, I just needed my cast to be split so I could accommodate swelling for the long plane rides home; get my prescriptions for pain med; get crutches; and go home.
All that sounds fast, but due to the critical patient that had come in, it took another two hours. They finally came and split my cast (which is done by using the cast cutter to cut a line, then another line, then pull out the strip in between), sold me my crutches, and wrote my prescriptions. The ER doc handed me my script, and I asked if the first rx had acetaminophen (because it would mess up my G4). He said it did, so he scribbled that out and prescribed ibuprofen instead. The nurse then got & apologized for “having to sell me” crutches. New Zealand has a public health policy where they cover everything in an accident for foreigners: I didn’t have to pay for the medevac (!!), the ER visit (!!), the x-rays (!!), the cast …nothing. Just the crutches (which they normally lend for free to NZ but obviously I was taking these home). Then I was on my way.
Thankfully, the company we hiked with had of course radioed into Queenstown, and the operations manager had called the ER and left a message to give to me with his phone number. A few hours prior, when I found out I’d be casted & released that night, I had been texting my mom & had her call the hotel Scott & I were staying at the next (Monday) night to see if they had a room that (Sunday) night that I could check into. The hiking company guy offered to drive me wherever, so he came to pick me up. I had texted him to keep him posted on my progress/timeline of release (nice and vague and unhelpful for the most part). But I also asked as soon as we got in contact if he could radio a message to the lodge & tell Scott that: a) my ankle was broken; b) I was ok; c) I’d be at the hotel when he got in the next day and not to rush, I was ok. The guy said he could do me one better: when he came to pick me up, he’d bring the phone so I could ::call: and talk to Scott directly. (I almost cried with relief, there, at the idea of getting to talk to Scott so he wouldn’t be beside himself worrying for 22 hours). I did get to talk to Scott for about a minute and tell him everything directly, and convince him not to hike out himself in the morning, but stick with the group and the normal transport method back to Queenstown, and just come meet me at the hotel when he got back around 4pm the next day. He agreed.
(What I didn’t find out until later is that Scott had considered doing the rest of the hike completely that night. Two things ended up dissuading him: one was the fact that a guide would have had to go with him and then hike all the way back to the lodge that night. The other was the fact that he talked to me and I would be out of the hospital by the time he arrived; so since I said I was fine alone at the hotel, he’d wait until the next day.)
So, I was taken to the hotel and got help getting up to the hotel room and had ice delivered along with extra pillows to prop up, and our bags brought in. Thankfully, on the mountain, the EMT had agreed to winch my backpack up with me. This was huge, because I noted earlier, I had a full set of supplies in my backpack, and all we had to do on the mountain was grab an extra international adapter and my charger cords out of Scott’s bag and toss it into mine. That made it easy to just pull what I needed that night (my rig; charger cords & adapter; a snack) out of the top of my bag from my perch on the bed. I plugged in my rig; made sure I was looping, took my pain meds, and went to sleep.
Amazingly, although you’re probably not any more surprised than I am at this point, my BGs stayed perfectly in range all night. Seriously: after that lowering from 160 once I relaxed and let some of the stress go? No lows. No highs. Perfectly in range. The pain/inflammation and my lack of eating didn’t throw me out of range at all. The day of the fall, all I ate was breakfast (8am); didn’t eat lunch and didn’t bother doing anything until 11pm when I had a beef jerky stick for some protein and half a granola bar (10g carbs). For the next two and a half weeks now, I’ve had no lows, and very few highs.
The one other high BG I really had was on Sunday after we got home (we got back on Wednesday). It happened after my crutch hit the door coming back to my bedroom from the bathroom, and I did such a good job hopping on my left foot and protecting my casted right foot, that I managed to break the smallest toe on my left foot. I pretty immediately knew that it was broken based on the pain; then my BG slowly rose from 110 up to 160; and then I started to have the same “shadow” bruising spread around my foot from the base of the toe. Scott wasn’t sure; when I had fallen off the trail I had yelled “help!” and “I think I broke my foot!”. I didn’t say it out loud this time; just thought it. Again, after some ibuprofen and icing and resting, within an hour my BG started coming back down slowly to below 100 mg/dL.
On Tuesday, I went to the orthopedic surgeon and confirmed: my left toe is definitely broken. My right ankle is definitely broken: the trimalleolar fracture diagnosis from NZ was confirmed. However, given that none of the ligaments were damaged, and the ankle was in a decent position, the ortho said there’s a good chance I can avoid surgery and heal in place inside a cast. The plan was to take off my split, plaster-based cast they did in NZ and give me a proper cast. We’d follow up in 10 days and confirm via x-ray that everything was going well. I asked how likely surgery would still be with this plan; and he said 20%. Well, given that I was assuming 100% before, that was huge progress! He also told me I shouldn’t travel within 4 weeks of the injury, which unfortunately means I had to cancel my trip to Berlin for ATTD later in February. It may or may not mean I have to cancel another trip; I’ll have to wait and see after the next follow up appointment, depending on whether or not I need surgery.
Up until this point, I had been fairly quiet (for me) on social media. I hadn’t posted the pictures of our hike; I didn’t talk about my fall or the trip home. One friend had texted and said “I wondered if you fell off the face of the earth!” to which I responded “uhhh…well…about that…I ::only:: fell off a mountain! Not earth!” Ha. Part of the reason was not knowing whether or not I would be able to travel as planned, and wanting to be courteous to informing the conferences who invited me to speak about the situation & what it meant for me being able to attend/not. Once I had done that, I was able to start posting & sharing with everyone what had happened.
For those who follow my airport travels and wondered just how long I was in NZ…I’m actually home now, and have been home for almost a week. I skipped on the last airport reporting.
To be perfectly honest, it’s one thing to have a broken limb and a cast and have to use crutches. It’s an entirely other ball of wax to have a broken toe on the foot that’s supposed to be your source of strength & balance. The ortho gave me a post-op surgical shoe to wear on my left foot to try to help, but it hurt so bad that I can’t use my knee scooter to move easily without my left foot burning from the pain. Thankfully, Scott’s parents’ neighbor also had a motorized sit-scooter that we borrowed. However, due to the snowpocalypse that hit Seattle, I’ve not been able to leave the house since Thursday. We haven’t been able to drive anywhere, or walk/scooter anywhere, in days. I’m not quite stir crazy yet; but; I’ll be really looking forward to the sidewalks being snow-free and hopefully lake-free (from all the melting snow) later in the week so I can get out again. I also picked up a cold somewhere, so I for the most part have been stationary in bed for the last week, propping up my feet and using endless boxes of Kleenex.
▪️Trimalleolar fracture in the right ankle. ▪️Fracture of the smallest toe on my left foot. ▪️And now a cold is kicking in. 🤧
OpenAPS, as you can see, has done an excellent job responding to the changes in my insulin needs from being 100% sedentary. (Really – think trips to the bathroom and that’s it.) In addition to the increased resistance from my cold and being sedentary, there’s one other new factor I’ve been dealing with. I asked my ortho about nutrition, and he wants me to get 1g of protein per kg of body weight, plus 1000mg/day of calcium. He suggested getting the extra protein via a powder, instead of calories (e.g. eating extra food). I found a zero-carb, gluten free powder that’s 25g of protein per scoop, and have been trying it with chocolate milk (which is 13g of carb and 10g of protein).
(I'm mixing it with lactose-free chocolate milk that's lower carb (13g carbs per 1 cup) than regular; and the vanilla flavor I got is a tad on the sweet side 😑..it's tolerable now that it mixes in by shaking, but looking forward to trying the unflavored version in a few days).
I’ve been drinking that 2x a day. Interestingly, previous to my injury, unless I was eating a 100% no carb meal (such as eggs and bacon for breakfast), I didn’t need to bolus/account for protein. However, even though I’m entering carbs for chocolate milk (15), I was seeing a spike up to 150 mg/dL after drinking it. I tried entering 30g for the next time (13g of milk; plus about 50% for the 25+10g worth of protein), and that worked better and only resulted in a 10 mg/dL rise in response to it. But even a handful of nuts’ worth of protein, especially on days where I’m hardly eating anything, have a much stronger effect on my BGs. This could be because my body is adjusting to me eating a lot less (I don’t have much appetite); adjusting to the much-higher-protein diet overall; and/or responding to the 100% sedentary pattern of my body now.
Thankfully, it’s not been a big deal, and OpenAPS does such a good job tamping down on the other noise-based factors: it’s nice that my biggest problems are brief rises to 160 or 170 mg/dL (that then come back down on their own). My 7-day and 30-day BG averages have stayed the same; and my % time in range for 80-160 has stayed the same, even with what feels like a few extra protein-related blips, and even when some days I eat hardly anything and some days I manage 2-3 meals.
So to summarize a ridiculously long post:
When I break bones, my BGs rise up (due to inflammation and/or the stress/other hormonal reaction) up to 160 mg/dL until I relax, when they’ll come back down. Otherwise, broken bones don’t really phase OpenAPS.
Ditto for lack of movement and changes in activity patterns not phasing OpenAPS.
The biggest “challenge” has been adjusting to the 3x amount of protein I’m getting as a dietary change.
I have a trimalleolar fracture; and that’s about 7% of ankle fractures. I read a lot of blog posts about people needing surgery & the recovery from it taking a long time. I’m not sure I won’t need surgery; but I’m hoping I won’t need it. If so, here’s one data point for a trimalleolar fracture being non-surgical – I’ll update more later with full recovery timelines & details. Also, here is a Twitter thread where I’m tracking some of the most helpful things for life with crutches.
Don’t break your littlest toe – it can hurt more than larger fractures if you have to walk on it!
A huge thank you goes to my parents and Scott’s parents; our siblings on both sides for being incredibly supportive and helpful as well; and Scott himself who has been waiting on me (literally hand and foot) and taking most excellent care of me.
Current status:
Broken ankle: ✅✅🔲🔲🔲🔲 (2 weeks down in the hard casts!)
Broken toe: ✅🔲🔲🔲 (1 week down) @scottleibrand: ✅ has not fled house ✅still being amazingly kind and helpful and thoughtful ✅ still an absolute keeper! 💜
It’s hard to express the magnitude of how much closed looping can improve a person with diabetes’ life, especially to someone who doesn’t have diabetes or live closely with someone that does. There are so many benefits – and so many way beyond the typically studied “A1c improvement” and “increased time in range”. Sure, those happen (and in case you haven’t seen it, see some of the outcomes from various international studies looking at DIY closed loop outcomes). But everything else…it’s hard to explain all of the magic that happens in real life, that’s made so much richer by having technology that for the most part keeps diabetes out of the way, and more importantly: off the top of your mind.
Personally, my first and most obvious benefit, and the whole reason I started DIYing in the first place, was to have the peace of mind to sleep safely at night. Objective achieved, immediately. Then over time, I got the improvements in A1c and time in range, plus reduction in time spent doing diabetes ‘stuff’ and time spent thinking about my own diabetes. The artificial pancreas ‘rigs’ got smaller. We improved the algorithm, to the point where it can handle the chaos that is everything from menstrual cycle to having the flu or norovirus.
More recently, in the past ~17 months, I’ve achieved an ultimate level of not doing much diabetes work that I never thought was possible: with the help of faster insulin and things like SMB’s (improved algorithm enhancements in OpenAPS), I’ve been able do a simple meal announcement by pressing a button on my watch or phone..and not having to bolus. Not worrying about precise carb counts. Not worrying about specific timing of insulin activity. Not worrying about post-meal lows. Not worrying about lots of exercise. And the results are pretty incredible to me:
But I remember early on when we had announced that we had figured out how to close the loop. We got a lot of push back saying, well, that’s good for you – but will it work for anyone else? And I remember thinking about how if it helped one other person sleep safely at night..it would be worth the amount of work it would take to open source it. Even if we didn’t know how well it would work for other people, we had a feeling it might work for some people. And that for even a few people who it might work for, it was worth doing. Would DIY end up working for everyone, or being something that everyone would want to do? Maybe not, and definitely not. We wouldn’t necessarily change the world for everyone by open sourcing an APS, but that could help change the world for someone else, and we thought that was (and still is) worth doing. After all, the ripple effect may help ultimately change the world for everyone else in ways we couldn’t predict or expect.
This has become true in more ways than one.
That ‘one other person’ turned into a few..then dozen..hundreds..and now probably thousand(s) around the world using various DIY closed loop systems.
And in addition to more people being able to choose to access different DIY systems with more pumps of choice, CGMs of choice, and algorithm of choice, we’ve also seen the ripple effect in the way the world works, too. There is now, thankfully, at least one company who is evaluating open source code; running simulations with it; and where it is out-performing their original algorithm or code components, utilizing that knowledge to improve their system. They’re also giving back to the open source diabetes community, too. Hopefully more companies will take this approach & bring better products more quickly to the market. When they are ready to submit said products, we know at least U.S. regulators at the FDA are ready to quickly review and work with companies to get better tools on the market. That’s a huge change from years ago, when there was a lot of finger pointing and what felt like a lot of delay preventing newer technology from reaching the market. The other change I’m seeing is in diabetes research, where researchers are increasingly working directly with patients from the start and designing better studies around the things that actually matter to people with diabetes, including analyzing the impact and outcomes of open source technology.
After five years of open source diabetes work, and specifically four years of DIY closed looping, it finally feels like the ripples are ultimately helping achieve the vision we had at the start of OpenAPS, articulated in the conclusion of the OpenAPS Reference Design:
Is there still more work to do? Absolutely.
Even as more commercial APS roll out, it takes too long for these to reach many countries. And in most parts of the world, it’s still insanely hard and/or expensive to get insulin (which is one of the reasons Scott and I support Life For A Child to help get insulin, supplies, and education to as many children as possible in countries where otherwise they wouldn’t be able to access it – more on that here.). And even when APS are “approved” commercially, that doesn’t mean they’ll be affordable or accessible, even with health insurance. So I expect our work to continue, not only to support ongoing improvements with DIY systems directly; but also with encouraging and running studies to generalize knowledge from DIY systems; hopefully seeing DIY systems approved to work with existing interoperable devices; helping any company that will listen to improve their systems, both in terms of algorithms but also in terms of usability; helping regulators to see both what’s possible as well as what’s needed to successfully using these types of system in the real world. I don’t see this work ending for years to come – not until the day where every person with diabetes in every country has access to basic diabetes supplies, and the ability to choose to use – or not – the best technology that we know is possible.
But even so, after four years of DIY closed looping, I’m incredibly thankful for the quality of life that has been made possible by OpenAPS and the community around it. And I’m thankful for the community for sharing their stories of what they’ve accomplished or done while using DIY closed loop systems. It’s incredible to see people sharing stories of how they are achieving their best outcomes after 45 years of diabetes; or people posting from Antartica; or after running marathons; or after a successful and healthy pregnancy where they used their DIY closed loop throughout; or after they’ve seen the swelling in their eyes go done; etc.
The stories of the real-life impacts of this type of technology are some of the best ripple effects that I never want to forget.
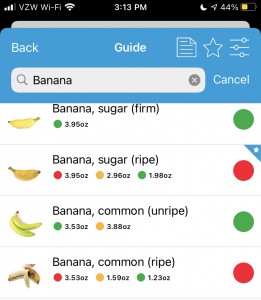
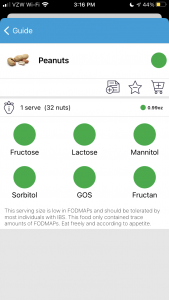
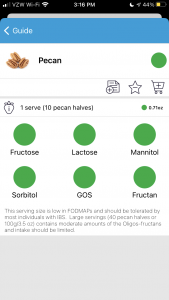
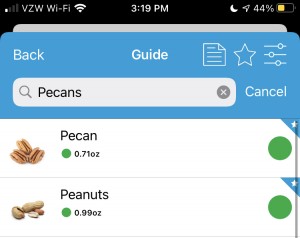
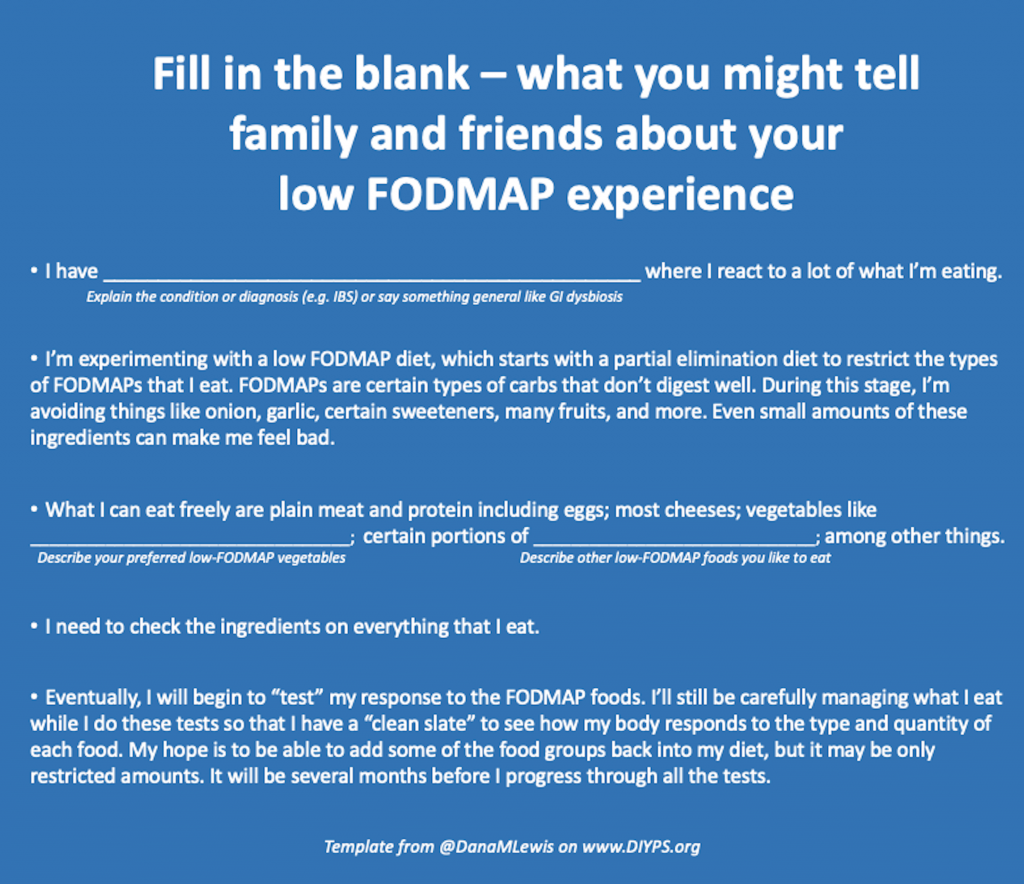

 I started with a basic sketch of an idea to run it by Scott and a few other people to test the idea. I’m not much for drawing, so it was a *very* rough sketch. But the analogy seemed to resonate, so I moved on to mocking up a basic version on the computer. (I went down a rabbit hole because I thought it would be neat to make an animated video for people to see and share online, to accompany the book. But I don’t know how to illustrate on the computer, let alone animate, so I tried an open source illustration program called Synfig, then several other illustrator programs that were open source to do the basic design to import into Synfig to animate, but then realized what I had in mind was so simple that basic transitions and animations in PowerPoint would suffice for my animated video.) PowerPoint is also
I started with a basic sketch of an idea to run it by Scott and a few other people to test the idea. I’m not much for drawing, so it was a *very* rough sketch. But the analogy seemed to resonate, so I moved on to mocking up a basic version on the computer. (I went down a rabbit hole because I thought it would be neat to make an animated video for people to see and share online, to accompany the book. But I don’t know how to illustrate on the computer, let alone animate, so I tried an open source illustration program called Synfig, then several other illustrator programs that were open source to do the basic design to import into Synfig to animate, but then realized what I had in mind was so simple that basic transitions and animations in PowerPoint would suffice for my animated video.) PowerPoint is also 


 Blood glucose and insulin exhibit coupled biological rhythms at multiple timescales, including hours (ultradian, UR) and the day (circadian, CR) in individuals without diabetes. The presence and stability of these rhythms are associated with healthy glucose control in individuals without diabetes. (See right, adapted from
Blood glucose and insulin exhibit coupled biological rhythms at multiple timescales, including hours (ultradian, UR) and the day (circadian, CR) in individuals without diabetes. The presence and stability of these rhythms are associated with healthy glucose control in individuals without diabetes. (See right, adapted from 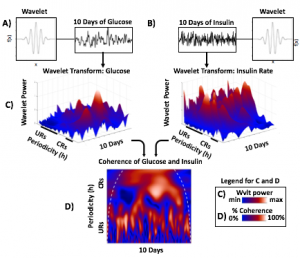
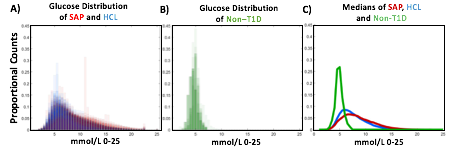
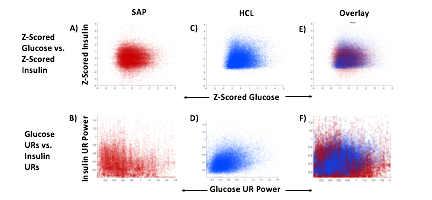
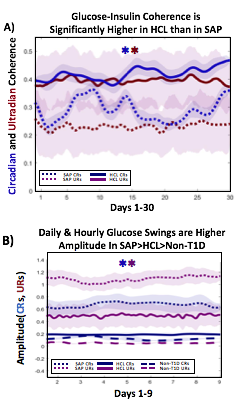 A) Circadian (blue) and 3-6 hour ultradian (maroon) coherence of glucose and insulin in HCL (solid) and SAP (dotted) users. Transparent shading indicates standard deviation. Although both HCL and SAP individuals have lower coherence than would be expected in a non-T1D individual, HCL CR and UR coherence are significantly greater than SAP CR and UR coherence (paired t-test p= 1.51*10-7 t=-5.77 and p= 5.01*10-14 t=-9.19, respectively). This brings HCL users’ glucose and insulin closer to the canonical non-T1D phenotype than SAP users’.
A) Circadian (blue) and 3-6 hour ultradian (maroon) coherence of glucose and insulin in HCL (solid) and SAP (dotted) users. Transparent shading indicates standard deviation. Although both HCL and SAP individuals have lower coherence than would be expected in a non-T1D individual, HCL CR and UR coherence are significantly greater than SAP CR and UR coherence (paired t-test p= 1.51*10-7 t=-5.77 and p= 5.01*10-14 t=-9.19, respectively). This brings HCL users’ glucose and insulin closer to the canonical non-T1D phenotype than SAP users’.
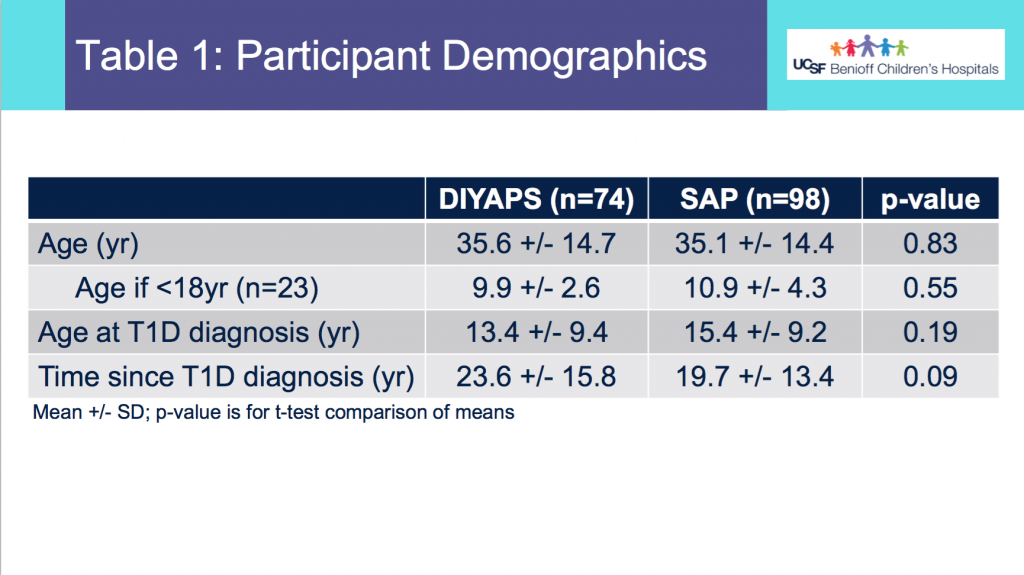
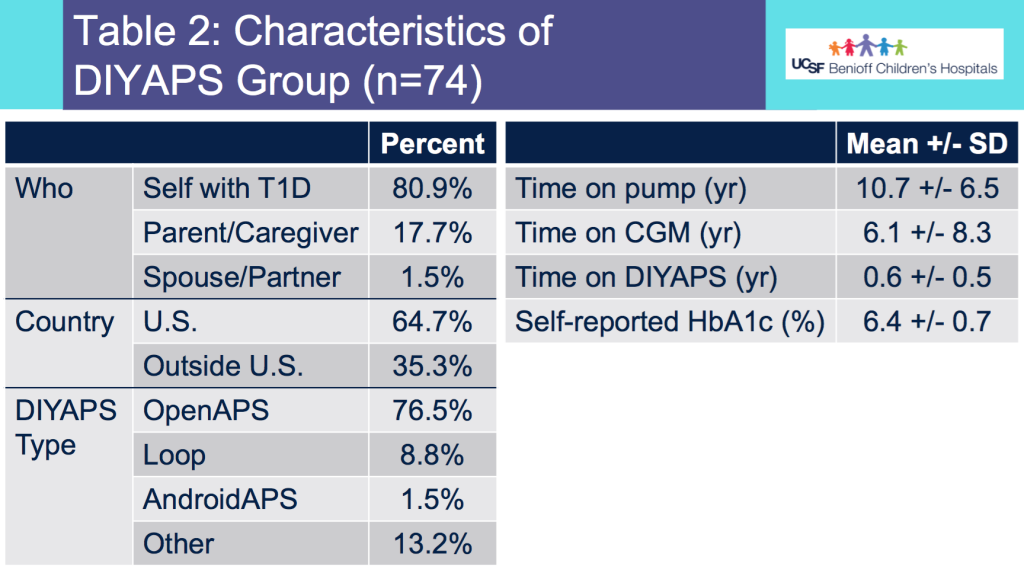
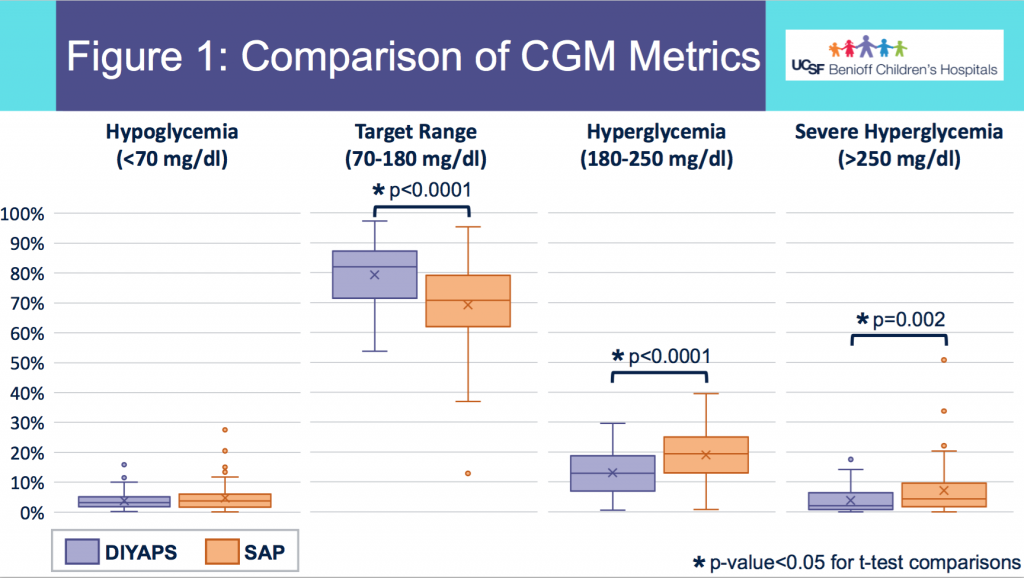
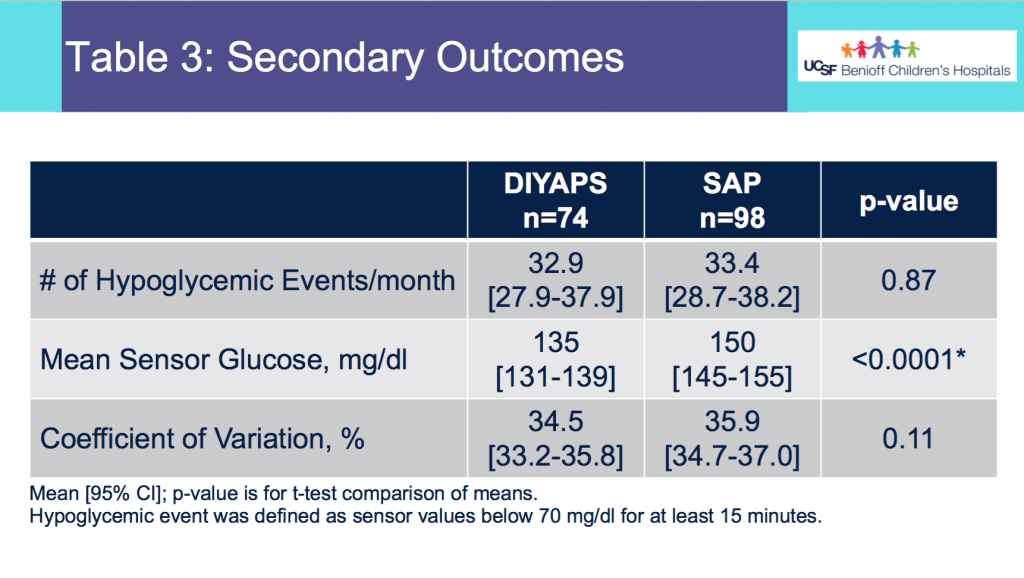
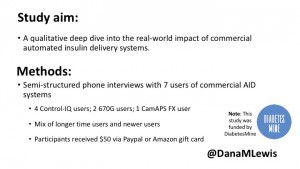
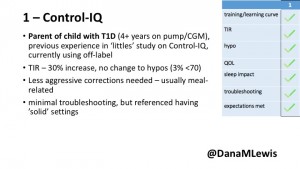
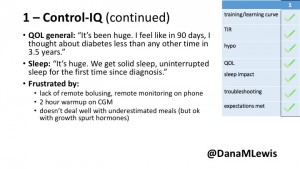 1 – A parent of a child using Control-IQ (off-label), with 30% increase in TIR with no increased hypoglycemia. They spend less time correcting than before; less time thinking about diabetes; and “get solid uninterrupted sleep for the first time since diagnosis”. They wish they had remote bolusing, more system information available in remote monitoring on phones. They miss using the system during the 2 hour CGM warmup, and found the system dealt well with growth spurt hormones but not as well with underestimated meals.
1 – A parent of a child using Control-IQ (off-label), with 30% increase in TIR with no increased hypoglycemia. They spend less time correcting than before; less time thinking about diabetes; and “get solid uninterrupted sleep for the first time since diagnosis”. They wish they had remote bolusing, more system information available in remote monitoring on phones. They miss using the system during the 2 hour CGM warmup, and found the system dealt well with growth spurt hormones but not as well with underestimated meals.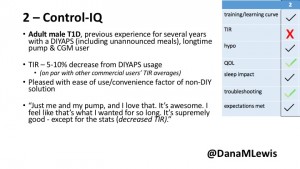
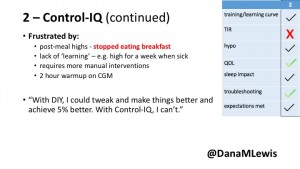 2 – An adult male with T1D who previously used DIYAPS saw 5-10% decrease in TIR (but it’s on par with other participants’ TIR) with Control-IQ, and is very pleased by the all-in-one convenience of his commercial system.He misses autosensitivity (a short-term learning feature of how insulin needs may very from base settings) from DIYAPS and has stopped eating breakfast, since he found it couldn’t manage that well. He is doing more manual corrections than he was before.
2 – An adult male with T1D who previously used DIYAPS saw 5-10% decrease in TIR (but it’s on par with other participants’ TIR) with Control-IQ, and is very pleased by the all-in-one convenience of his commercial system.He misses autosensitivity (a short-term learning feature of how insulin needs may very from base settings) from DIYAPS and has stopped eating breakfast, since he found it couldn’t manage that well. He is doing more manual corrections than he was before.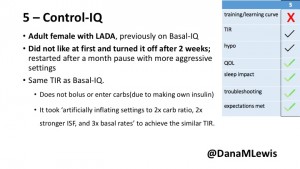
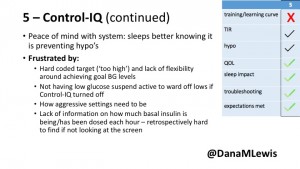 5 – An adult female with LADA started, stopped, and started using Control-IQ, getting the same TIR that she had before on Basal-IQ. It took artificially inflating settings to achieve these similar results. She likes peace of mind to sleep while the system prevents hypoglycemia. She is frustrated by ‘too high’ target; not having low prevention if she disables Control-IQ; and how much she had to inflate settings to achieve her outcomes. It’s hard to know how much insulin the system gives each hour (she still produces some of own insulin).
5 – An adult female with LADA started, stopped, and started using Control-IQ, getting the same TIR that she had before on Basal-IQ. It took artificially inflating settings to achieve these similar results. She likes peace of mind to sleep while the system prevents hypoglycemia. She is frustrated by ‘too high’ target; not having low prevention if she disables Control-IQ; and how much she had to inflate settings to achieve her outcomes. It’s hard to know how much insulin the system gives each hour (she still produces some of own insulin).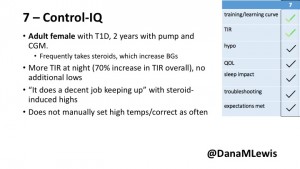
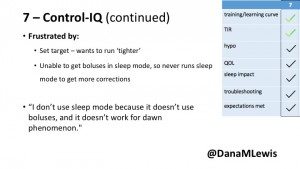 7 – An adult female with T1D who frequently has to take steroids for other reasons, causing increased BGs. With Control-IQ, she sees 70% increase in TIR overall and increased TIR overnight, and found it does a ‘decent job keeping up’ with steroid-induced highs. She also wants to run ‘tighter’ and have an adjustable target, and does not ever run in sleep mode so that she can always get the bolus corrections that are more likely to bring her closer to target.
7 – An adult female with T1D who frequently has to take steroids for other reasons, causing increased BGs. With Control-IQ, she sees 70% increase in TIR overall and increased TIR overnight, and found it does a ‘decent job keeping up’ with steroid-induced highs. She also wants to run ‘tighter’ and have an adjustable target, and does not ever run in sleep mode so that she can always get the bolus corrections that are more likely to bring her closer to target.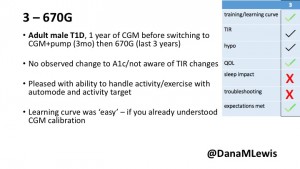
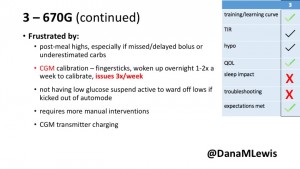 3 – An adult male with T1D using 670G for 3 years didn’t observe any changes to A1c or TIR, but is pleased with his outcomes, especially with the ability to handle his activity levels by using the higher activity target. He is frustrated by the CGM and is woken up 1-2x a week to calibrate overnight. He wishes he could still have low glucose suspend even if he’s kicked out of automode due to calibration issues. He also commented on post-meal highs and more manual interventions.
3 – An adult male with T1D using 670G for 3 years didn’t observe any changes to A1c or TIR, but is pleased with his outcomes, especially with the ability to handle his activity levels by using the higher activity target. He is frustrated by the CGM and is woken up 1-2x a week to calibrate overnight. He wishes he could still have low glucose suspend even if he’s kicked out of automode due to calibration issues. He also commented on post-meal highs and more manual interventions.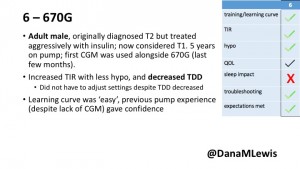
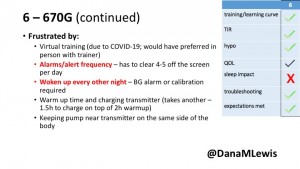 6 – Another adult male user with 670G was originally diagnosed with T2 (now considered T1) with a very high total daily insulin use that was able to decrease significantly when switching to AID. He’s happy with increased TIR and less hypo, plus decreased TDD. Due to #COVID19, he did virtually training but would have preferred in-person. He has 4-5 alerts/day and is woken up every other night due to BG alarms or calibration. He does not like the time it takes to charge CGM transmitter, in addition to sensor warmup.
6 – Another adult male user with 670G was originally diagnosed with T2 (now considered T1) with a very high total daily insulin use that was able to decrease significantly when switching to AID. He’s happy with increased TIR and less hypo, plus decreased TDD. Due to #COVID19, he did virtually training but would have preferred in-person. He has 4-5 alerts/day and is woken up every other night due to BG alarms or calibration. He does not like the time it takes to charge CGM transmitter, in addition to sensor warmup.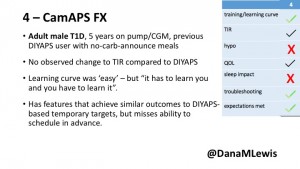
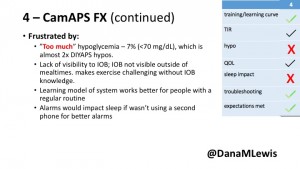 4 – The last participant is an adult male with T1 who previously used DIYAPS but was able to test-drive the CamAPS FX. He saw no TIR change to DIYAPS (which pleased him) and thought the learning curve was easy – but he had to learn the system and let it learn him. He experienced ‘too much’ hypoglycemia (~7% <70mg/dL, 2x his previous), and found it challenging to not have visibility of IOB. He also found the in-app CGM alarms annoying. He noted the system may work better for people with regular routines.
4 – The last participant is an adult male with T1 who previously used DIYAPS but was able to test-drive the CamAPS FX. He saw no TIR change to DIYAPS (which pleased him) and thought the learning curve was easy – but he had to learn the system and let it learn him. He experienced ‘too much’ hypoglycemia (~7% <70mg/dL, 2x his previous), and found it challenging to not have visibility of IOB. He also found the in-app CGM alarms annoying. He noted the system may work better for people with regular routines.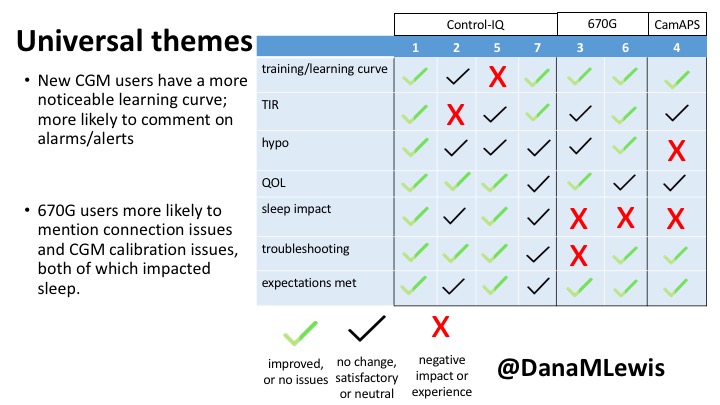
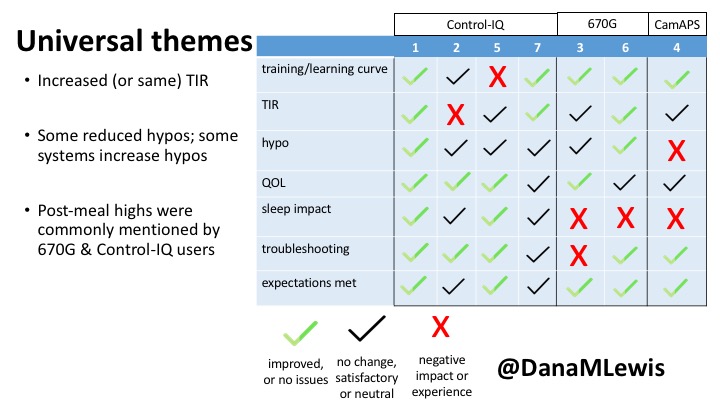
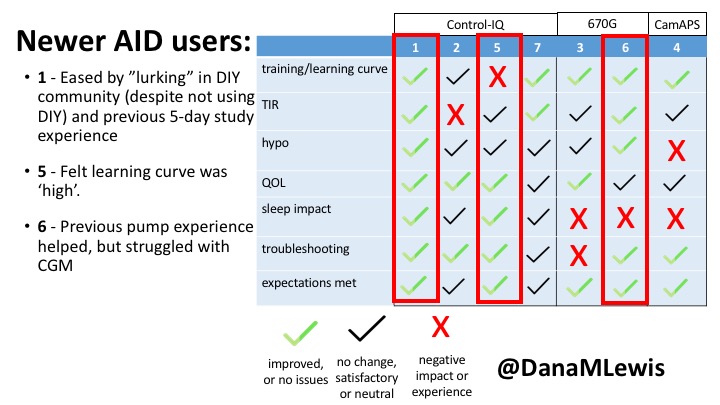
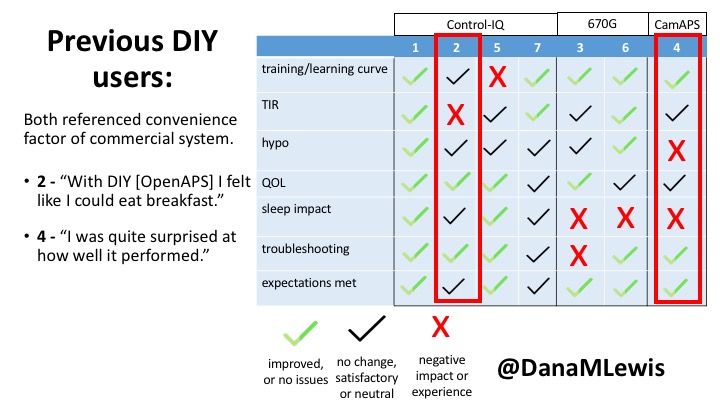

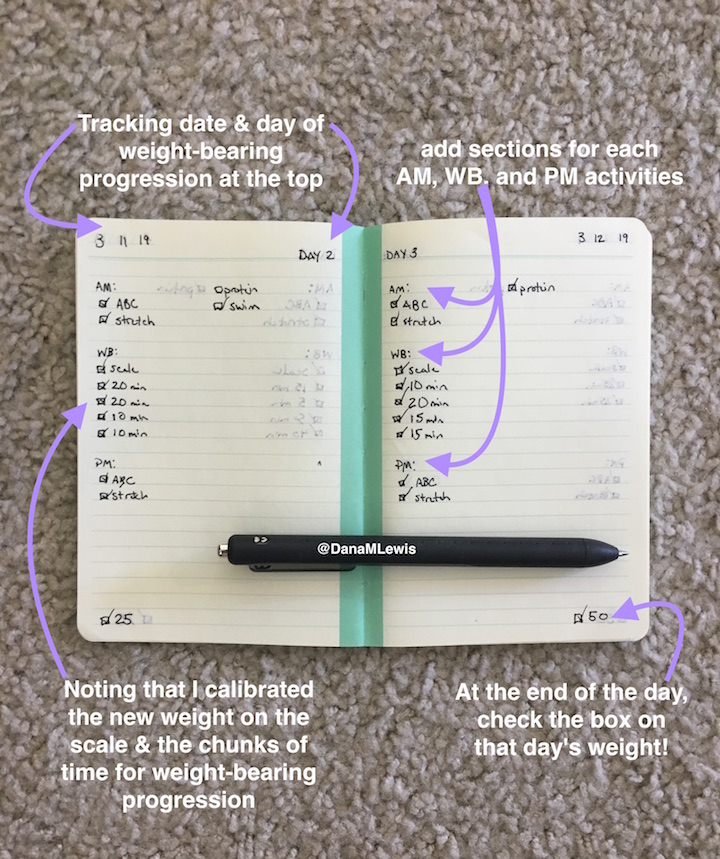

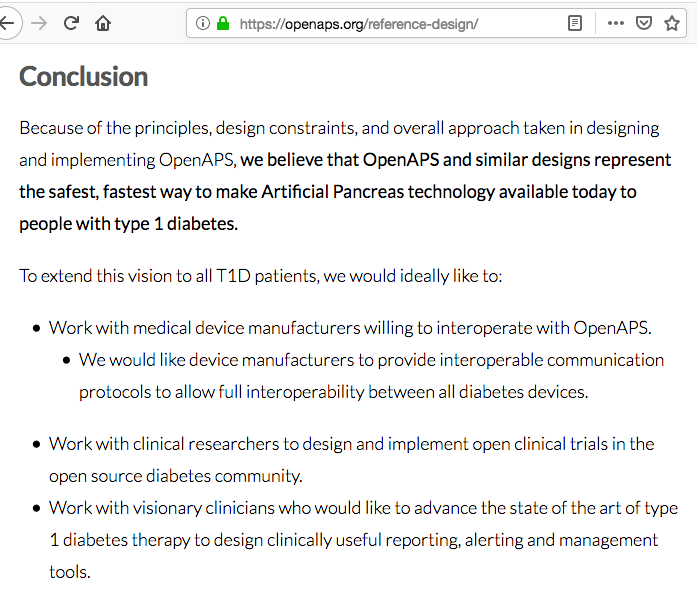
Recent Comments