One of the most common questions I have been asked over the last 8 years is whether or not we are submitting OpenAPS to the FDA for regulatory approval.
This question is a big red herring.
Regulatory approval is often seen and discussed as the one path for authenticating and validating safety and efficacy.
It’s not the only way.
It’s only one way.
—
As background, you need to understand what OpenAPS is. We took an already-approved insulin pump that I already had, a continuous glucose monitor (CGM) that I already had, and found a way to read data from those devices and also to use the already-built commands in the pump to send back instructions to automate insulin delivery via the decision-making algorithm that we created. The OpenAPS algorithm was the core innovation, along with the realization that this already-approved pump had those capabilities built in. We used various off the shelf hardware (mini-computers and radio communication boards) to interoperate with my already approved medical devices. There was novelty in how we put all the pieces together, though the innovation was the algorithm itself.
The caveat, though, is that although the pump I was using was regulatory-approved and on the market, which is how I already had it, it had later been recalled after researchers, the manufacturer, and the FDA realized that you could use the already-built commands in the pump’s infrastructure. So these pumps, while not causing harm to anyone and no cases of harm have ever been recorded, were no longer being sold. It wasn’t a big deal to the company; it was a voluntary recall, and people like me often chose to keep our pumps if we were not concerned about this potential risk.
We had figured out how to interoperate with these other devices. We could have taken our system to the FDA. But because we were using already-off-the-market pumps, there was no way the FDA would approve it. And at the time (circa 2014), there was no vision or pathway for interoperable devices, so they didn’t have the infrastructure to approve “just” an automated insulin delivery algorithm. (That changed many years later and they now have infrastructure for reviewing interoperable pumps, CGM, and algorithms which they call controllers).
The other relevant fact is that the FDA has jurisdiction based on the commerce clause in the US Constitution: Congress used its authority to authorize the FDA to regulate interstate commerce in food, drugs, and medical devices. So if you’re intending to be a commercial entity and sell products, you must submit for regulatory approval.
But if you’re not going to sell products…
This is the other aspect that many people don’t seem to understand. All roads do not lead to regulatory approval because not everyone wants to create a company and spend 5+ years dedicating all their time to it. That’s what we would have had to do in order to have a company to try to pursue regulatory approval.
And the key point is: given such a strict regulatory environment, we (speaking for Dana and Scott) did not want to commercialize anything. Therefore there was no point in submitting for regulatory approval. Regardless of whether or not the FDA was likely to approve given the situation at the time, we did not want to create a company, spend years of our life dealing with regulatory and compliance issues full time, and maybe eventually get permission to sell a thing (that we didn’t care about selling).
The aspect of regulatory approval is a red herring in the story of the understanding of OpenAPS and the impact it is having and could have.
Yes, we could have created a company. But then we would not have been able to spend the thousands of hours that we spent improving the system we made open source and helping thousands of individuals who were able to use the algorithm and subsequent systems with a variety of pumps, CGMs, and mobile devices as an open source automated insulin delivery system. We intentionally chose this path to not commercialize and thus not to pursue regulatory approval.
—
As a result of our work (and others from the community), the ecosystem has now changed.
Time has also passed: it’s been 8 years since I first automated insulin delivery for myself!
The commercial players have brought multiple commercial AIDs to market now, too.
We created OpenAPS when there was NO commercial option at the time. Now there are a few commercial options.
But it is also an important note that I, and many thousands of other people, are still choosing to use open source AID systems.
Why?
This is another aspect of the red herring of regulatory approval.
Just because something is approved does not mean it’s available to order.
If it’s available to order (and not all countries have approved AID systems!), it doesn’t mean it’s accessible or affordable.
Insurance companies are still fighting against covering pumps and CGMs as standalone devices. New commercial AID systems are even more expensive, and the insurance companies are fighting against coverage for them, too. So just because someone wants an AID and has one approved in their country doesn’t mean that they will be able to access and/or afford it. Many people with diabetes struggle with the cost of insulin, or the cost of CGM and/or their insulin pump.
Sometimes providers refuse to prescribe devices, based on preconceived notions (and biases) about who might do “well” with new therapies based on past outcomes with different therapies.
For some, open source AID is still the most accessible and affordable option.
And in some places, it is still the ONLY option available to automate insulin delivery.
(And in most places, open source AID is still the most advanced, flexible, and customizable option.)
—
Understanding the many reasons why someone might choose to use open source automated insulin delivery folds back into the understanding of how someone chooses to use open source automated insulin delivery.
It is tied to the understanding that manual insulin delivery – where someone makes all the decisions themselves and injects or presses buttons manually to deliver insulin – is inherently risky.
This net risk reduction is important to contextualize.
Without automated insulin delivery, people overdose or underdose on insulin multiple times a day, causing adverse effects and bad outcomes and decreasing their quality of life. Even when they’re doing everything right, this is inevitable because the timing of insulin is so challenging to manage alongside dozens of other variables that at every decision point play a role in influencing the glucose outcomes.
With open source automated insulin delivery, it is not a single point-in-time decision to use the system.
Every moment, every day, people are actively choosing to use their open source automated insulin delivery system because it is better than the alternative of managing diabetes manually without automated insulin delivery.
It is a conscious choice that people make every single day. They could otherwise choose to not use the automated components and “fall back” to manual diabetes care at any moment of the day or night if they so choose. But most don’t, because it is safer and the outcomes are better with automated insulin delivery.
Each individual’s actions to use open source AID on an ongoing basis are data points on the increased safety and efficacy.
—
However, this paradigm of patient-generated data and patient choice as data contributing toward safety and efficacy is new. There are not many, if any, other examples of patient-developed technology that does not go down the commercial path, so there are not a lot of comparisons for open source AID systems.
Yet still, there was concern around safety because the healthcare world didn’t know how to assess these patient-generated data points of choice to use this system because it was better than the alternative every single day.
No surprises here, though. I’ve been using this system for more than 8 years, and seeing thousands of others choose the OpenAPS algorithm on an ongoing, daily basis for similar reasons.
—
So today, it is possible that someone could take an open source AID system using the OpenAPS algorithm to the FDA for regulatory approval. It won’t likely be me, though.
Why not? The same reasons apply from 8 years ago: I am not a company, I don’t want to create a company to be able to sell things to end users. The path to regulatory approval primarily matters for those who want to sell commercial products to end users.
Also, regulatory approval (if someone got the OpenAPS algorithm in an open source AID or a different algorithm in an open source AID) does not mean it will be commercially available, even if it will be approved.
It requires a company that has pumps and CGMs it can sell alongside the AID system OR commercial partnerships ready to go that are able to sell all of the interoperable, approved components to interoperate with the AID system.
So regulatory approval of an AID system (algorithm/mobile controller design) without a commercial partnership plan ready to go is not very meaningful to people with diabetes in and of itself. It sounds cool, but will it actually do anything? In and of itself, no.
Thus, the red herring.
Might it be meaningful eventually? Yes, possibly, especially if we collectively have insurers to get over themselves and provide coverage for AID systems given that AID systems all massively improve short-term and long-term outcomes for people with diabetes.
But as I said earlier, regulatory approval does necessitate access nor affordability, so an approved system that’s not available and affordable to people is not a system that can be used by many.
We have a long way to go before commercial AID systems are widely accessible and affordable, let alone available in every single country for people with diabetes worldwide.
Therefore, regulatory approval is only one piece of this puzzle.
And it is not the only way to assess safety and efficacy.
—
The bigger picture this has shown me over the years is that while systems are created to reduce harm toward people – and this is valid and good – there have been tendencies to convert to the assumption that therefore the systems are the only way to achieve the goal of harm reduction or to assess safety and efficacy.
They aren’t the only way.
As explained above, FDA approval is one method of creating a rubber stamp as a shorthand for “is this considered to be safe and effective”.
That’s also legally necessary for companies to use if they want to sell products. For situations that aren’t selling products, it’s not the only way to assess safety and efficacy, which we have shown with OpenAPS.
With open source automated insulin delivery systems, individuals have access to every line of code and can test and choose for themselves, not just once, but every single day, whether they consider it to be safer and more effective for them than manual insulin dosing. Instead of blindly trusting a company, they get the choice to evaluate what they’re using in a different way – if they so choose.
—
So any questions around seeking regulatory approval are red herrings.
A different question might be: What’s the future of the OpenAPS algorithm?
The answer is written in our OpenAPS plain language reference design that we posted in February of 2015. We detailed our vision for individuals like us, researchers, and companies to be able to use it in the future.
And that’s how it’s being used today, by 1) people like me; and 2) in research, to improve what we can learn about diabetes itself and improve AID; and 3) by companies, one of whom has already incorporated parts of our safety design as part of a safety layer in their ML-based AID system and has CE mark approval and is being sold and used by thousands of people in Europe.
It’s possible that someone will take it for regulatory approval; but that’s not necessary for the thousands of people already using it. That may or may not make it more available for thousands more (see earlier caveats about needing commercial partnerships to be able to interoperate with pumps and CGMs).
And regardless, it is still being used to change the world for thousands of people and help us learn and understand new things about the physiology of diabetes because of the way it was designed.
That’s how it’s been used and that’s the future of how it will continue to be used.
I’ve been taking thyroid medication for a few months now. It surprised me how quickly I saw some symptom resolution. As I wrote previously, I started taking thyroid medication and planned to get more lab work at the 8 week mark.
The theory is that thyroid medication influences the production of new thyroid hormones but not the stored thyroid hormones; thus, since it takes around 6 weeks for you to replace your stores of thyroid hormones, you usually get blood work no sooner than 6 weeks after making a change to thyroid medication.
I had noted, though, that some of my symptoms included changes in my heart rate (HR). This was both my overnight resting HR and how my HR felt during the day. I had hypothesized:
Given I have a clear impact to my heart rate, I’m hypothesizing that I might see changes to the trend in my heart rate data sooner than 6 weeks – 2 months, so that’ll be interesting to track!
I ended up being prescribed a 5mg dose. Thinking about it, given my T3 and T4 were well within range, that made sense. I started taking it in early August.
What it felt like to start taking antithyroid medication for the first time:
For context, my primary most bothersome symptoms were eye symptoms (eyelid swelling, sometimes getting a red patchy dry area outside the outer corner of my eye, eye pressure that made me not want to wear my contacts); increased resting overnight HR and higher HR during periods of rest during the day; and possibly mood and energy impacts.
Within a week (!) of starting the antithyroid medication, my overnight HR began lowering. This can be influenced by other factors like exercise etc., but it was also accompanied by fewer days with higher heart rate while I was sitting and relaxing! I definitely felt a noticeable improvement within a week of my heart rate-related symptoms.
My eyelid swelling went away toward the end of the first week. Then after 3 or so days, it came back again for a few days, then went away for 12 days. It came back for several days, went away for another 6 days. Came back, then…nothing! I went weeks without eyelid swelling and none of the other eye-related symptoms that typically ebbed and flowed alongside the eyelid swelling. HOORAY!
It’s unclear how much my mood and energy were directly effected by the wonky thyroid antibody levels compared to being a correlation with the symptoms themselves. (I was also resuming ultramarathon training during this time period, following the recovery of my broken toe.) However, I definitely was feeling more energetic and less grumpy, as noticed by my husband as well.
What is interesting to me is that my symptoms were changed within a week. They often talk in the medical literature about not knowing exactly how the thyroid medication works. In my case, it’s worth noting again for context that I had subclinical hyperthyroidism (in range T3 and T4 but below range TSH) and Graves’ disease (several thyroid antibodies well above range) with correlated eye symptoms. The theory is that the eye symptoms are influenced by the thyroid antibody levels, not the thyroid levels (T3 and T4) themselves. So although the thyroid medication influences the production of new thyroid hormones and it takes 6 weeks to replace your store of thyroid hormones; my working hypothesis is that the symptoms driven by TSH and thyroid antibodies are influenced by the production of those (rather than the stores) and that is why I see a change to my symptoms within a week or so of starting thyroid medication.
I went for repeat lab work at 8 weeks, and I was pretty confident that I would have improved antibody and TSH levels. I wasn’t sure if my T3 and T4 would drop below range or not. The lab work came back in and… I was right! TSH was back to normal range (HOORAY), T3 and T4 were slightly lower than the previous numbers but still nicely in the middle of the range. Yay! However, my TSI (thyroid stimulating immunoglobulin) was still well above range, and slightly higher than last time. Boo, that was disappointing, because there are some studies (example) showing that out of range TSI can be a predictor for those with Graves’ disease for the need to continue antithyroid medication in the future.
As I wrote in my last post:
I am managing my expectations that managing my thyroid antibody and hormone levels will be an ongoing thing that I get to do along with managing insulin and blood sugars and managing pancreatic enzymes. We’ll see!
The TSI was a pointer that although I had reduced all of my symptoms (hooray) and my T3 and T4 were within range, I would probably need ongoing medication to keep things in range.
However, as a result of the lab work, my provider suggested dropping down to 2.5mg dose, to see if that would manage my thyroid successfully without pushing me over to hypothyroidism (low T3 and T4) levels, which can be a risk of taking too much antithyroid medication. He suggested switching to 2.5mg, and repeating lab work in 3 months or if I felt unwell.
I agreed that it was worth trying, but I was a little nervous about reducing my dose, because my T3 and T4 were still well within the middle of normal. And, I had an upcoming very long ultramarathon. Given that with the start of thyroid medication I saw symptoms change within a week, and I was two weeks out from my ultra, I decided to wait until after the ultramarathon so I could more easily monitor and assess any symptoms separately from the taper and ultra experience.
Recovery from my ultramarathon was going surprisingly well, enough so that I felt ready to switch the medication levels pretty soon after my ultra. I started taking the 2.5mg dose (by cutting the 5mg dose in half, as I had some remaining and it was easier than ordering a changed prescription to 2.5mg).
I carefully watched and saw some slight changes to my HR within the first week. But, I was also recovering from an ultramarathon, and that can also influence HR. Again, I was looking at both the overnight resting HR and noting any periods of time during the day where I was resting when my HR was high (for me). I had two days where it did feel high during the day, but the following days I didn’t observe it again, so I chalked that up to maybe being related to ultramarathon recovery.
But a little over a week and my right eye started feeling gunky. I had just been to the eye doctor for my annual exam and all was well and my eye didn’t look red or irritated. I didn’t think much of it. But a few days after that, I had rubbed my right eyelid and realized it felt poofy. I felt my left eyelid in comparison, and the right was definitely swollen in comparison. Looking in the mirror, I could see the swollen eyelid pushing down the corner of my right eye. Just like it had done before I started thyroid medications. Ugh. So eye symptoms were back. A few days later, I also woke up feeling like my eyes hurt and they needed lubrication (eye drops) as soon as I opened my eyes. That, too, had been a hallmark of my eye symptoms from last October onward.
The plan had been to wait until 3 months after this medication change to repeat labs. I’m going to try to wait until the 6-8 week mark again, so we can see what the 2.5mg does to my T3 and T4 levels alongside my TSH. But, my prediction for this next round of lab work is that T3 and T4 will go up (maybe back to the higher end but likely still within range; although the possibility to fully go above range), and that my TSH will have dropped back down below range, because the symptom pattern I am starting to have mimics the symptom pattern I had for months prior to starting the 5mg thyroid medication.
Why only wait 6-8 weeks, when my provider suggested 3 months?
These symptoms are bothersome. The eyelid swelling thankfully subsided somewhat after 4 days (after the point where it got noticeable enough for my husband to also see it compressing my outer corner of my eye, which means anyone would be able to visibly see it), but I’m watching it to see if it returns with a cyclical pattern the way it went away previously, expecting it to likely return to constant every day eye swelling. Since it influences my vision slightly (because the eyelid is pushed down by the swelling), that impacts my quality of life enough to take action sooner. If it gets really bad, I might discuss with my provider and get labs even sooner, but I’m going to try to tough it out to 6-8 weeks to get a full picture of data of how the 2.5mg impacted all of my levels and also see what pattern of symptoms return when, because it will be interesting to compare the symptom levels at 5mg (essentially all gone within 1-2 weeks) and at 2.5mg compared to my original, pre-thyroid medication symptom levels and patterns.
But depending on those labs, I predict that I will return to taking the 5mg dose, and hopefully my symptoms will go away completely and stay away. Then it’ll be a future decision on if/when to try titrating down again; possibly guided by the TSI level, since the TSI was still above range when we had switched me to 2.5mg (despite the change in TSH back to range).
The good news is, though, that in future I should be able to use the 1-2 weeks of symptom data to determine whether a change in dose is working for me or not, instead of having to wait a full 6-8 weeks, because my symptoms seem to be driven by the TSH and antibody levels, rather than out of range T3 and T4 levels (because they were and are still in the middle of the goal range).
I also discussed this with my eye doctor. You’ll note from my previous post that I was very concerned about the eye impacts and symptoms, so I had asked my eye doctor if she’s still comfortable treating me (she is), and we talked about what things would cause me to get a referral to a specialist. So far my symptoms don’t seem on track for that; it would be my eyes protruding from the socket and having pressure that would possibly need surgery. Disappointingly, she confirmed that there’s really no treatment for the symptoms since they’re caused by the antibody levels. There’s no anti-swelling stuff to put on my eyelid to help. Instead, the goal is to manage the antibody levels so they don’t cause the symptoms. (Which is everything I’m talking about doing above, including likely returning to the 5mg dose given that my eye symptoms resumed on the 2.5mg dose).
—
In summary, I think it is worth noting for anyone with Graves’ disease (whether or not they have subclinical or actual hyperthyroidism) that it is possible to see symptom changes within a week or two of starting or changing your thyroid medication. I can’t find anything in the literature tracking symptom resolution on anything shorter than a 6 week time period, but maybe in the future someone will design a study to capture some of the real-world data and/or run a prospective study to capture this data and see how prevalent this is for symptoms to resolve on a much shorter time frame, for those of us whose symptoms are driven not by thyroid levels themselves (T3 and T4) but for the TSH and TSI and other thyroid antibodies (TPO etc).
If you do start thyroid medication, it’s worth logging your symptoms as soon as possible, ideally before you start your medication, or if it’s too late for that, start logging them afterward. You can then use that as a comparison in the future for if you reduce, increase, or are directed to stop taking your medication, so you can see changes in the length of time it takes to develop or reduce symptoms and whether the patterns of symptoms change over time.
What do you see when you see (or think of) diabetes?
—
In my house, I see small piles of low treatments (for hypoglycemia) in every place that I hang out. On my desk next to my computer. In my bedside table. On the counter next to the door where I grab them before heading out for a run or a walk. On the edge of the bathtub in my shower, because low blood sugars happen everywhere.
Sometimes, one of my nephews spots them in a translucent pocket on my shorts. His brain sees candy at first, not a medical treatment. Which is fine – he’s young. He’s learning that for Aunt Dana, they’re not “candy” or a “treat” – they’re a medical treatment.
All of the nieces and nephews have learned or are learning that Aunt Dana has “robot parts”, which is how they see my pump clipped to my pocket or waist band or the hard lump (CGM sensor) they feel or see on my arm.
—
What I hope people see, though, is that diabetes is not a death sentence. Thanks to improvements in insulin, insulin delivery, and blood glucose measuring, it’s no longer visibly tied to possible complications of diabetes, like amputations, kidney dialysis, or loss of vision. That is what I saw when I was diagnosed with diabetes in 2002, and what was presented to me.
I hope instead that people see people with diabetes like me living our lives, running 82 mile ultramarathons (for those of us who wish to do that), experiencing pregnancy (for those who wish to do that), achieving our career goals, living life in whatever ways we want to live our lives. Just like everyone else.
—
It’s worth noting that when typing this, autocorrect in my first sentence suggested “treat” instead of “treatment”.
So computers learn that. And that’s what they see.
When I was testing Stable Diffusion (an open source AI tool for generating images) recently, I learned about a site “Lexica” that shows you what other people have generated with similar key words. I thought it would be interesting to get ideas for better images to visualize concepts in posts about diabetes, so I searched diabetes.
I should’ve known better. Humans say and think “diabetes” in response to seeing pictures of carbohydrates, so that’s what computers learn.
AI doesn’t know any better because humans haven’t taught themselves any better.
Sadly, “insulin pump” as a key word is disheartening in a different way.
There are so few existing visuals and images of people with insulin pumps that the visual images generated by AI are a mix of weird hybrid old school computer components and blood glucose monitors or other medical devices.
“Hypoglycemia” mostly generates cartoons in foreign languages or made up languages that I’m guessing are jokes by people without diabetes about having low blood sugar and using it as an excuse for various things. “Hyperglycemia” brings a mix of the hypoglycemia-style cartoons and the diabetes-style images of carbs and how the AI thinks people with diabetes all look.
I’ve noticed this with AI-writing tools, too. AI is good at completing your sentence or writing a few sentences based on well known concepts and topics that already exist today. It’s not yet good at helping you write content about new concepts or building on existing content.
It’s trained on the content of today and the past, which means all of the biases, stereotypes, and stigmatizing content that aren’t good today are also extrapolated into our future with AI.
I don’t have all the answers or solutions (I wish I did), but I want to flag this as a problem. We can’t expect AI to do better trained on what we have and do today, because what we do today (stigmatize, stereotype, and harm people living with chronic diseases) is not ok and not good enough.
We need to change today and train AI with different inputs in order to get different outputs.
That starts with us changing our behavior today. As I wrote a few days ago, please speak up when you see chronic diseases being used as a “joke” and when we see people being stereotyped or when we see racism occurring.
It’s hard, it’s uncomfortable – both to speak up, and to be corrected.
I’ve been corrected before, on verbal patterns and phrases I learned from society that I didn’t realize were harmful and stigmatizing to other people.
I’m working on learning to say “I’m sorry, you’re right, and let me learn from this” and trying to do better in the future, living up to my statement that I’m going to learn from that moment.
It can absolutely be done. It desperately needs to be done, by all of us.
We can course-correct, whether it’s in a one on one conversation, something we see in a small social network in social media, or even in a large room at a conference.
I still remember and appreciate greatly when I flagged that a diabetes joke was made at a conference on stage over four years ago. Upon hearing the joke, I noted that half the room laughed; and that it wasn’t ok. So I spoke up on Twitter, because I was live tweeting from the conference. I didn’t think much would come from it. But it did. Amazingly, it did.
John Wilbanks saw my tweet, realized it wasn’t ok, and instead of tweeting support or agreement (which also would have been great), took an amazing, colossally huge and unexpected step. He literally got up from his seat, went to the microphone, and interrupted the panel that had moved on to other topics. He called out the fact that diabetes was used as a joke a few minutes prior and that it wasn’t ok.
He put on a master class for how to speak up and how to use his power to intervene.
It was incredibly powerful because although the “joke” had gone over most people’s heads and they didn’t think it was a big deal, he brought attention to the fact that it had happened, was hurtful and harmful, and created a moment for reflection for the entire room of hundreds of people.
We need more of this.
When someone flags that they are being stereotyped, stigmatized, being discriminated against – we need to speak up. We need to support them.
It matters not just for today (although it matters incredibly much for today, too) but also for the future.
AI (artificial intelligence) learns from what we teach it, much like our children learn from what we teach and show them. I don’t have kids, but I know what I do and how I behave matters to my nieces and nephews and how they see the future.
We need to understand that AI is learning from what we are doing today, and what we do today matters. It should be enough to want to not be racist, discriminating, stereotyping, and harmful to other people today. But it’s not enough.
The loudest voices are often the ones establishing “normal” for our culture, our children, and the AI systems that may be running much of the world before our children graduate college. We need to speak up to help shape the conversation today, because what we are doing today is teaching our children, our technology, and is what we’ll get in the future, ten-fold.
And I want the future to look different and be better, for all of us.
I have a favor to ask of you, especially you as a person who is not living with diabetes.
—
On day 1 of diabetes awareness month 2022 (also known as today), I saw a tweet. Someone posted a picture of some snacks and asked what people thought it was.
Like clockwork, one of the replies was “Diabetes”.
The original tweet’s author replied with a laughing emoji.
I saw it, sighed, and clicked away.
Then I clicked back to it. And typed: Diabetes “jokes” aren’t funny.
Later, I checked and the author deleted their laughing emoji tweet. The original “Diabetes” tweet still stands.
—
I’ve lived with type 1 diabetes now for more than 20 years.
It’s not because of what I ate as a kid. It has nothing to do with what I ate before or what I eat now.
Most cases of diabetes, in fact, are not the direct result of individual behavior (such as what we choose to eat), and result from a complicated combination of genetics, immune system shenanigans, and numerous factors outside of people’s control (such as the environment in which they live). Diet changes can sometimes delay the onset of type 2 diabetes, but diet is never the sole cause of it, and usually not even the dominant factor.
Diabetes is no one’s fault, just like getting cancer is no one’s fault.
But unlike cancer or asthma or numerous other life-altering chronic diseases, diabetes is a punchline in society.
It’s treated as something you can judge and shame other people for. It was 20 years ago and it is today.
Literally, today.
Probably hundreds if not thousands of times, people are out there making diabetes jokes.
So here’s where the favor comes in that I’d like you to do for me, especially those of you reading this who don’t have diabetes, when you see someone making a diabetes “joke”.
Speak up. Say something. Anything. Don’t look away.
Say, “please stop” or “Diabetes “jokes” aren’t funny” or “Why are you stigmatizing people?”
Because these are in fact stigmatizing comments. It impacts us in ways you can’t imagine, from our day to day lives (people trying to restrict our food or tell us what we can eat) all the way to the fact that these pervasive, stigmatizing attitudes are so internalized, even by healthcare professionals, that they actively cause harm when we seek healthcare in the healthcare system.
So please, say something. Advocate for and with us. Be our allies. Speak up, and give us a break. We don’t get a break from diabetes. We sometimes get burnt out from advocating for ourselves and keeping ourselves alive. That is a lot of work, as is advocating. But it would be great if we got a break from the “jokes” that aren’t jokes.
That’s something you can do for diabetes awareness month, and every month, that will make a meaningful difference for people living with all types of diabetes.
(Thanks.)
– (PS – For what it’s worth, those snacks being tweeted about were actually for running an ultramarathon, which takes a lot of snacks. And people with diabetes, like me, can eat snacks and run an 82 mile ultramarathon.)
Sometime in the last year, I decided I wanted to run 100 miles. In part, because I wanted to tackle the complex challenge and problem-solving that is even figuring out how to do it.
My situation as an ultrarunner is slightly atypical: I have type 1 diabetes and need to closely manage insulin levels and glucose levels while running; I have celiac disease so I can only eat 100% gluten free things; and I have exocrine pancreatic insufficiency (EPI) so I need to swallow enzymes with everything that I eat, including when I run. It’s a logistical cornucopia of challenges…which is in part why I wanted to do it. It wouldn’t be half as rewarding if it were easy? Or something like that.
But mainly, I wanted to prove to myself that I can do hard things, even things that most people think I can’t do. No, I can’t produce my own insulin, but I can locomote for 100 miles at one time despite this and the other challenges I have to deal with along the way.
Plus, there’s the “normal” ultrarunning challenges of fueling, hydrating, managing electrolytes, keeping your feet from becoming a ball of blisters, etc.
Ultrarunning is a sport where it generally doesn’t matter how fast you go, and the farther the distance the more of an equalizer it is. I’m a slow runner, and I had trained at an easy slow pace that I planned to run during my race (self-organized). Not having the pressure of time cutoffs would help. I was also curious whether running so slow at the start would possibly help me maintain a more even pace split across the entire run, and whether I could ultimately achieve a reasonable time by keeping consistent slow paces, compared to many I’ve read about who go a bit too fast at the start and end up with wildly different paces at the end. Everyone hurts running an ultra no matter how much you run or walk or both and no matter how fast or slow you go, but I was hoping that more consistent pacing and effort would minimize how terrible everything felt if I could pull that off.
Background
I trained, ran a 50k in June, and resumed training and worked back up to 24 mile long runs and all was going well, until I massively broke a toe and had 6 weeks off. Then I resumed training and re-built back up to running 29 miles, ending around midnight for night-run training. At that point, I had one more long run scheduled (32-ish miles), but decided I would rather skip the last long run and push my 100 mile run up a few weeks to try to beat the impending rainy season that Seattle would eventually get.
The joke was on me. We had 6+ weeks of terrible air quality, which peaked into a two-day stretch of downright “hazardous” (ugh) air quality the two days before my run. Air quality was finally improving overnight before and the morning of my run, thanks in part to the most rain we had gotten in 128 days. Woohoo! So I got to add some wet and cold running challenges to my list of problem-solving that I’d tackle during my run.
Overall, though, my training had gone well, and I had spent enough time planning and prepping that I felt relatively confident. Mostly, confident that no matter how well or long I trained, it was going to hurt. All over. For what felt like forever, and then I still wouldn’t be anywhere near done. And confident that I had planned and prepped to the best of my ability, and that I could figure out how to tackle whatever situations I faced as they came.
How I felt before the race
Aside from having cabin fever from being inside (AQI was too hazardous to go out even with a mask), I felt fairly good in terms of running fitness. I had been tapering, my legs felt fresh, I was fueling and hydrating and everything felt fine. Unfortunately, though, while I managed to escape many taper niggles, I experienced a round of ovulation pain that I don’t get every month but was lucky enough to get this month, for the 3 days prior to my race. (I’m not sure why, but in the last few years after never experiencing ovulation pain, I have started to get ovulation pain similar to period pain and cramps and general icky feelings. My doctor isn’t concerned about it, but it’s unfun, and in this case poorly timed.) So I was a bit grumpy about going into my race in a less-than-perfect state, even though “perfect” state is an ideal and usually there is something wrong, whether it’s a taper niggle or something else.
The thing I was most pleased about was my feet. My broken toe had healed well and hadn’t been giving me any issues. However, after I broke my toe it changed my foot strike or how my feet move in my shoes in a way that caused epic blisters and then I kept getting blisters on top of blisters for several runs. I finally figured out that I needed to try something different, stopped causing new blisters, and the existing blisters healed, peeled off, and went away. So my feet were in great shape, and despite being nervous about the effect of the rain on my feet during my 100 miles, I at least was starting from a “clean slate” with healthy, non-blistered feet.
The start
I set my alarm and woke up and checked air quality. The winds and the start of the rain had blown it absolutely clear, so I was able to head out without a mask for the first time in weeks! (Last time I ran with it for all 8 hours of my long run, which is annoying when you need to fuel every 30 min.)
I wasn’t even a mile in when I had my first problem. I started with a long sleeve shirt and my rain jacket, knowing I’d warm up and want to take it off soon after I started. As I removed my arms from my rain jacket (keeping it zipped around my waist) and shuffled my arms in and out of my running vest, I suddenly felt water hit my feet and looked down. Water was gushing out of my hydration hose! I grabbed it and stuck my finger over the end: the bite valve had flown off somehow while I was getting out of my jacket. Ugh.
Luckily, though, this is where all of my planning and reading of others’ experiences had come in handy. While this had never happened to me, I had read in someone’s blog that this had happened and it took them 20 minutes to find the valve. I had a bright waistlamp and it was getting increasingly lighter outside as the sun rose, so I hoped mine would be easier to spot. I figured it was stuck in my rain jacket sleeve so I worked to check my sleeve and vest for the valve. No go. I looked around and didn’t see it. I turned and walked back a bit, looking for it on and off the trail. No luck. I finally pulled out my phone and called Scott, while still holding my finger over the hydration hose to keep it from leaking out 3 liters of water. While I talked to him and told him I probably needed him to get dressed and bike out a replacement valved to me, I turned around and walked forward again one more time. Aha! Found it. It had flown way to the left side of the trail. I replaced it and breathed a sigh of relief. It had added only 4 minutes to my first mile time.
Well, I thought: that’s one way to keep my early paces slow! I hung up with Scott, and carried on.
The first lap I was very focused on making sure my socks and shoes were in good shape. I am pretty good at gutting it out if I have blisters or foot issues, but that’s not a good strategy when you’re going to cover 99 more miles. So 6 miles into my first lap, I stopped at a bench, took my socks off, and re-lubricated my feet. Later on the way back (this first lap was an out-and-back), I stopped at mile 16 and similarly sat on a rock to re-lubricate and add lamb’s wool to reduce rubbing on the side of my foot.
Yet overall, lap 1 went well. It started raining after about 20 minutes so I ran with my rain hat and rain jacket on (I put it on after my bite valve escapades at mile 1), and intermittently put my hood over my hat and took it off when the rain picked up or lessened, respectively. But it pretty much rained the whole time. Scott met me as planned after my turnaround spot (about 12 miles in) and refilled my hydration pack and I re-packed my vest with snacks, enzymes, and electrolytes and carried on.
At the end of lap 1 (almost 24 miles), I physically felt pretty decent. I had been working to focus on the lap I was in and what I needed to do for the next lap. Nothing else. No thoughts of how many miles I would run or hours it would take. My watch had stopped itself in the rain and canceled the run (argh), so I wasn’t going to have a running total of time throughout the entire run like I wanted. But this might have been a feature, as it kept me from using my watch for that and I set a new lap/run each time I headed out so I could keep an eye on the segment pace, even though I had no idea what the overall pace time really was.
I went slow the first lap (part of why I was feeling so strong), and I took my time in between laps. I pulled off my socks and shoes. I used hand sanitizer on them to draw some of the water out, then re-lubricated and added Desitin (to continue to help draw water out of my feet and aid in preventing blisters). Then I put on a fresh pair of toe socks and added more lamb’s wool in between key toes that typically are blister-prone. At this stage I had no blisters, and other than wet soggy feet was in good shape! Sitting for 10 minutes for my sock and foot care change chilled me, though, and I was happy to start moving again and warm back up.
The middle
I headed out on lap 2, which similarly went well. This was my “triangle” shaped loop/lap. The only issue I had this lap was that it was the only section of my route where the trail crossed 3 small intersections. Two had lights but one did not. At the intersection without a light, there were no cars so I continued running across the pedestrian crossing. As I stepped out I saw a car whipping around the corner with their head turned looking for cars in the opposite direction. Not sure if they would turn in time to see me, I slammed on my physical brakes. They did turn and see me and stopped in plenty of time, so I continued across the crossing and on the trail. However, that had tweaked my right ankle and it felt sore and weak. Argh. It felt better after a few more minutes, but it intermittently (once every hour or so) would feel weak and sore throughout the rest of my run as a result.
After lap 2, I again sat to remove my socks and shoes, dry my feet, put hand sanitizer on them, re-lubricate, etc. My feet were definitely wet and wrinkly, so I added even more Desitin to my feet. It wasn’t raining super hard but it was a constant hard drizzle that was soaking through to my socks and feet even though there weren’t many puddles (yet). This time, though, I used some reusable hot packs while I sat to change shoes, so I wasn’t as chilled when I left.
Lap 3 (back to an out-and-back route) also went well, and I was starting to realize that I was in surprisingly good physical shape. My feet were intermittently a little bit sore from pounding the ground for hours, but they weren’t constantly annoying like I’ve had on some training runs. I had long surpassed my longest running distance (previously 32 miles; at the end of lap 3 I would reach 52 miles) and longest ever running time. I did develop one or two small blisters, but they didn’t bother me. Usually, I build up huge blisters and they’re a constant annoyance. During my race, maybe thanks to the Desitin etc, I only noticed the blisters (which were fairly tiny) when they popped themselves. I had one on each foot pop and sting for a minute and then not bother me again, which was pleasant! Lap 3 was also when it got dark, so I’d headed out with my double waist lamp. I have two sets of two waist lamps that we strapped to each other; I turn one on and run it out (somewhere around ~3 hours) and then turn the belt around and turn the other lamp on. This lasts me the longest laps I have, even if I was going at walking speed. It’s plenty of light for the paved trail even on the darkest nights, but because it was raining it was cloudy and the city’s light pollution reflected off the clouds so that trail itself was easy to see! So while I only saw a few stars at the end of the night in between patches of cloud, for most of the night the night-running aspects were pretty easy.
Interestingly regarding my feet, after lap 3 they were still white and wrinkly a bit, but they were definitely drying out. They were much drier than they had been after lap 2, so the combination of hand sanitizer and Desitin was working. I was pleased, and again slathered with more lubricant and Desitin before putting on fresh socks and heading back out for lap 4, which would be a repeat of my “triangle” lap.
Physically, I was mostly ok. My feet weren’t hurting. I had expected my IT bands to get tight and bother my right knee and for my hips and back to start getting sore: my left knee did intermittently hurt some, but it was like a 3/10 annoyance and came and went. Stretching my hip flexors didn’t change the tightness of my IT band, but it was also the least amount of knee pain I’ve ever had when things got tight, so it was very manageable and I didn’t stress about it. It was hard to believe that with the completion of this lap (lap 4) that I’d have finished a 100k (62 miles) and added a few miles to it!
It seemed like the triangle loop wanted to keep things interesting, though. On Lap 4, after I had turned off into the section that has the intersections and the “triangle” part of the loop, my hydration hose made a gurgling noise. I felt the back of my hydration pack, which was rock solid with ice…but no water left. Oops, I thought. I was at mile 6 out of 13. If I kept going forward on my route, it would take me an estimated 4+ miles to get back to the next water fountain. Or I could call and wake up Scott, who had just fallen asleep for his first 2 hour nap overnight (it was around 1am by now), to bring me water, but that would take him 20-30 minutes before reaching me.
It mattered that I didn’t have water. Not just in terms of thirst and hydration, but I also needed water to be able to swallow my electrolyte pills (every 45 minutes) and my fuel (every 30 minutes when I ate a snack) and the digestive enzymes I absolutely require to digest my food since I have EPI. I definitely needed water so that my hydration, fueling, electrolytes, etc. wouldn’t suffer.
I could go back, but I hated to backtrack. It would be a mile back to the previous water fountain, although I wasn’t even sure it would be turned on and working. Mentally, though, I groaned at the thought of “turning around” and finishing the loop in reverse and trying to figure out how many miles I would cut off that loop and how many I’d have to added to my very last loop to make up for it.
Luckily, I realized a better idea. Because I was on the section of the triangle running alongside a road (hence the annoying intersection crossings), the intersections are where the road turned off into various parking lots. Across the road at one of the two intersections with lights was a gas station! I could see it glowing from a quarter of a mile away. I crossed my fingers hoping it would still be open, because I could go inside and buy a bottle of water to hold me over. It was open! I crossed the intersection and went in, grabbed a liter of water, bought it, went outside, and refilled my hydration bladder under the bright lights of the gas station.
I’m wearing nitrile gloves to help keep my hands drier and warmer given the cold, endless rain.
I was pretty proud of that solution, especially because it was ~1am and I had been running for 17 hours and was able to troubleshoot and solve that problem on the fly! Without sending it, I also drafted a text to send to Scott near the end of that loop when he’d be awake, to list out which foods and gear I wanted at the next refuel, and to specify what happened and how I solved it and request that I get more water and less ice for the next loop.
(Running out of water was on my list of things I planned for in all of my preparation, so while I had low expectations of my mental capacity as the miles piled up, that likely helped because I had mentally listed out where all the available water fountains were, so I could run my loop mentally forward and backward to figure out where the closest one was. In this case it was a mile behind me; going forward it would have been 4+ miles or more than an hour away. The gas station ended up being 15 minutes from where I realized I was out of water).
Finishing lap 4 was exciting, because I only had 3 laps left to go! I had one more out and back loop, and my father-in-law was driving down in the wee hours of the morning to run part of it with me to keep me company. We hadn’t planned on that all along, but he and Scott had been texting and working it out, so Scott just told me that was the plan and I was thrilled. I was a little bit tired overall, but more energetic than I thought.
The sock change before lap 5 was disappointing, though. After lap 3, my feet had been drying out a little bit. Now after lap 4 they were wet and soft again, like they were after lap 2. The rain had been more constant. I took the time (15-20 min) I needed to dry and treat them with hand sanitizer, lubricant, Desitin, replace fresh toe socks and lambs wool and dry shoes. They weren’t hurting, so I was hoping the light rain would taper off and my feet would dry out again.
The (beginning of the) end
I headed out on to lap 5, buoyed by the thought that I only had ~4 miles ‘til I had company. The rain picked up again (argh) and as my father-in-law met me on the trail with his headlamp and rain gear, he asked if it had been raining this much the whole time. No, I said, and pointed out that it had only been raining hard in 10-20 minute chunks and this one had been going since before I met him so it should lighten up soon. He commented on how energetic and chatty I was. “You’re pretty chatty,” he said, “for 5am!” (I am well-known in both our families for NOT being a morning person). I joked about how impressive it was for me being this chatty not only at 5am but also for it being 22 hours into my run!
Unfortunately, 3 miles into the section he ran with me, it went from annoying hard drizzle to an epic mega downpour. My shoes went from damp from constant hard drizzle to super soaked from top all the way down to the insoles squishing with every step. I was frustrated, because this much rain was also making it hard to use my phone. My phone had an alarm going off every 30 minutes to remind me to fuel; I needed to pull out my phone each time and turn off the very loud alarm (it was effective!) and then open up my spreadsheet and enter what I ate and what electrolytes I took. Then I also had to pull the baggie out of my vest pocket, select out the number of enzyme pills I needed with wet and cold gloved fingers, re-seal the baggie and put it back in my vest, and get out the fuel from the other pocket of my vest and eat it. Even tired, I was managing to fuel successfully and stay on top of my schedule. I was increasingly proud of this.
But the rain and the inability to use my phone when I wanted to was starting to irritate me, in part likely because I was trying not to stress about what the volume of water was doing to my feet. They weren’t actively hurting, but I knew this much water for this long of time could be dangerous and I needed to be careful. It was still downpouring when we reached the turnaround and headed back to his car. I dropped him off at his car and carried on. I was tired, soaked, cold, but physically in great shape otherwise in terms of legs, knees, hips, back etc all holding up and not feeling like i had run ~78+ miles at that point!
I had just eaten another snack and went to press buttons on my pump to give myself some insulin for the snack. It didn’t seem to work. I have a vibration pattern so I can use the pump without seeing it; but the “enter” button was not working. I had been concerned about the volume of water my pump was going to be exposed to and mentally prepared for that, but it was SO disheartening to suddenly feel the pattern of 6+ vibrations followed by an audio beep indicating an error state had been reached on the pump. I cursed to myself, out in the rain after 24 hours of running, knowing what I would find when I pulled my pump out from under my jacket. Sure enough, “button error”, because water had gotten under the buttons and to protect itself, the pump went into a “I won’t do anything” state. That meant that the insulin I needed for my latest snack wasn’t going to happen and any future insulin wasn’t going to happen.
I pulled out my phone and started a text to Scott, explaining that I had a button error and needed him to pull out my backup pump. I told him where it was, told him to put in a new battery and program it with the basal rate that I wanted. I then sent a text saying it was raining a lot and it would be easier if he called me if he needed to talk, because it was so hard to use my phone in the rain. He read the text so I knew he was awake, so I called him and talked to him while I trudged on and he was getting dressed and packing up my replacement pump and the gear I needed for lap 6. Then we hung up and I carried on, grumbling along the way and starting to feel the physical effects of not having enough insulin for the past hour or so.
My blood glucose levels were rising, but I wasn’t worried about that. I knew once I had replacement insulin my blood sugars would come down nicely. I had prepared for this; there was a “high BG” baggie with supplies ready to go! But the combination of the 25+ hours of rain, the extra hard rain and cold temps from the last several hours, my feet starting to be bothered from the wet soaking, and then on top of it all the chemical feeling of not having insulin going in my body: it was a lot. I really focused on the physical state I was in, evaluating what I wanted to do. I knew that I could fix the cold state (switch to dry clothes; use hot packs) and my blood sugars (new replacement pump, take some inhalable insulin for a faster fix while the new pump insulin would be kicking in within an hour and fixed from there). But my feet were starting to bother me in a way that I wasn’t sure could be fixed with a 20 minute sock change.
Scott biked up to me right as I passed my favorite trail bathroom, the stalwart of my ultra, and had me turn around and head in there to be out of the rain. It was clean, big, had toilet paper, and was well lit and had the door open (wasn’t locked) all night long. I stepped inside the bathroom while Scott parked his bike by the building and whipped out the baggie with the replacement pump. I checked that no one else was in the women’s bathroom and he stepped inside, and impressively (to me) pulled out the baggie that held a garbage bag. I had packed it so I could more easily change clothes in public bathrooms by standing on it and placing my clothes on it so they wouldn’t be on the ground. He instead laid the garbage bag on top of the garbage can lid and set out my dry clothes, helped me out of my wet soaked rain jacket, hat, and shirts, and handed me my dry shirts followed by some hot packs. He gave me a giant one and told me to stuff it down my shirt, which I did. I took some inhalable insulin (which hits in about 15 minutes), then held the smaller hot packs in my hands while he was pulling out the bag with my replacement pump. I rewound and primed the pump with my existing reservoir and tubing, then reconnected it to my pump site and primed it. That problem (lack of insulin) was now solved, and I knew that my blood glucose would come back down to target over the next hour.
Next up, I could walk/run (or walk) the remaining 1.5 miles back to my normal turn around point, which was a table under a park awning that was relatively dry. I knew that I needed to be warmer and stay dry, and although I had dry clothes on now, I wasn’t sure that sitting outside even with hot packs while I tried to address my feet would warm me up. I told Scott that I wanted to go back to the house (thinking I’d walk the ~1.5 miles to the house). Then I could dry out my feet, get warm, and go back out if I wanted to continue. But I had a hunch I didn’t want to continue. My feet were feeling like they were getting to be in a not-good state from the level of water they had retained after 25 hours, despite all the excellent foot care.
I thought about it and realized that I was satisfied with running 82 miles. I was in otherwise decent physical shape and energy, I had been nailing my electrolytes and fueling and blood sugars the entire run. I had successfully run overnight; more than 24 hours; and by far (2.6x) the longest distance I had ever run. I could keep running to 100 miles (about 18 more miles), but no one cared if I did. I didn’t have to prove anything to anyone, including myself. I had planned, strategized, and executed above and beyond what I had thought was possible, both in terms of physical and mental performance. I had no major injuries, and I wanted to keep it that way. I knew I had the willpower and persistence to keep going; I was stubborn enough to do it; but as the last bit of icing on top of my ultramarathon cake, I wanted to have the mental strength to decide to stop where I was so I wouldn’t create a long-lasting injury in the last 18 miles from sheer stubbornness.
So I stopped. I told Scott I would decide for sure after I got home and dried off and warmed up, but that I was pretty sure this would be a stop and not just a pause. Rather than let me walk home in the rain, he insisted I stay in the warm dry bathroom while he biked home and got the car and brought it to the nearest trail entrance, which was about a quarter of a mile away (more good planning on my part!). Once he had gotten in the car and called me, I slowly walked out to meet him at the parking lot, reaching it right as he pulled in. The walk on my feet confirmed to me that they were done. They weren’t exceptionally blistered or injured, but I knew the cumulative water effect and soggy skin would likely lead to some damage if I continued on them. We headed home. I sat down and took off my socks and shoes and sure enough, my feet were wet, white, and very wrinkly and starting to crease. I took a hot shower then dried off, put hand sanitizer on my feet to help dry them out, and laid down with them sticking out of the covers to help them air out. Within a few hours, they had dried out, and showed me some blisters on the bottom of my right foot that were not really bad, but if I had kept going on them, the wet wrinkly tissue would’ve been very prone to more extreme damage. I reflected on the choice to stop and was still happy with my decision.
The 24 hours after I ran 82 miles
After my shower and laying down, I realized that I was (still) in great physical shape. Some parts of me were starting to stiffen up now that I had stopped, but they hadn’t bothered me at all during running. That was my hips that now hurt if I tried to lay on my side but not on my front or my back; and my thighs felt sore when I straightened and bent my legs. I had never even been tempted during my run to take pain meds because I was never overly sore and didn’t have any injuries.
(Note: you shouldn’t take NSAIDs during extreme events due to the risks of overworked kidneys having problems. I had packed Tylenol, which is acetaminophen, in case I needed it for pain management, but specifically did not pack any oral NSAIDs and warned Scott about offering me any. I did pack topical NSAID *gel* which is an extremely low quantity of NSAID compared to even one oral NSAID pill, and I used that once on my shoulder blades during the run. After my run, I waited several hours and made sure my kidneys were fine via hydration before I took any NSAID.)
It is very surprising to me that despite my longest training runs being almost a third of the distance I did, that I ended up in better physical shape at the end than I did during some training runs! This is probably in part due to going even slower (as planned) during my ultra, but I was really pleased. It might have also been due to the fact that I mentally trained for it to hurt really bad and to continue anyway. Again, lots of mental training and prep.
I ended up napping 2 hours after I got home and showered, and then was awake a few more hours and took another one hour nap. I ate several small meals throughout the day and stayed in bed to rest and not stress my feet further, then went to sleep at a normal bedtime and managed to sleep 9.5 hours through the night. Woohoo! I really wasn’t expecting that. I did wake up many times and find myself bending and flexing my knees or my ankles to help me roll over and could feel them being sore, but it wasn’t painful enough to fully wake me up or keep me from falling back to asleep within seconds, so it felt like a fully rested un-broken night of sleep.
The bottoms of my feet felt weird as they dried out, but progressively felt better and felt close to normal (normal meaning as normal as you are with a routine blister on the bottom of your forefoot) by the time I woke up the next morning (24 hours after ending my run). Everything that stiffened up in the first few hours after I stop has been gradually loosening up, so other than my forefeet still being sensitive with blisters, I’m walking around normally again.
The good, the bad, the ugly, and what I wish I had done differently
I had prepared for so much to go wrong, both those things in my control and things out of my control. And I think that’s why it actually didn’t hurt as much or go as wrong as it could have, despite all the variables in play. I nailed my pacing plan, energy levels, hydration levels, fueling intake, electrolyte intake, and enzyme intake.
I had estimated that I would need to take up to ~160 enzymes to cover my fueling. Remember that I stopped at ~25 hours (82 miles) instead of ~32 hours (100 miles) so I took less than that, but still a lot.
I consumed 50 (fifty!!!) snacks, one every 30 minutes, and swallowed multiple enzyme pills each time. I consumed at least 98 enzyme pills (!!!) in this 25 hour time period. I was concerned that my body wouldn’t be able to digest the pills or have some other issue with them, because I have never taken anywhere near this number of pills in a single day. But, it worked, and flawlessly: I had ZERO EPI-related issues and ZERO other gastrointestinal (GI) symptoms. GI symptoms are super common in ultras, even for people without things like EPI, so I’m incredibly thrilled with how well my planning and practicing paid off so I could execute my fueling plan and not have any issues.
My goal had been to take in ~250 calories per hour and ~500 mg of sodium per hour (from both the snacks every 30 min and electrolyte pills every 45 min). I use calories as my rolling metric because while most ultrarunners prioritize carbs, I’m running slower and likely more fat adapted than most people, and also need digestive enzymes no matter what I’m eating so taking small amounts of fat and protein are fine for me. Plus it makes for more interesting running snacks. So using calories as the global running metric of consumption rather than just carbs or fat etc. works for me. I nailed it, and across all 25 hours of my run I averaged 671 mg of sodium per hour and 279 calories per hour. I did have one hour where I somehow dropped low on sodium and felt it, and took an extra electrolyte pill to help catch up. It fixed the “low on sodium” feeling and I didn’t have any issues again. I had slightly more variability toward the end of the run, but that’s just due to the timing of when I logged it into my spreadsheet (due to the wet-phone issues I described earlier) and the auto-calculation on which hour it falls into; overall I still was maintaining the goal levels every hour.
(The purple dotted line is carbs, because I was curious about how that level fluctuated given that I didn’t prioritize my run snacks based on carbs at all. I generally seek <20 grams of carbs per snack but have a few that are closer to 30 grams; otherwise <10 or so grams of fat and however many grams of protein I don’t care).
How do I have all this data? I used my macronutrient spreadsheet as I went, selecting the snack I was going to eat from the drop-down list that then pre-populated the rest of the data in the sheet and updated a pivot table that summarized my rolling totals per hour. It was getting increasingly hard to use my phone in the mega downpour rain in the last few hours, which is why the timing of logging them was a little variable and the numbers look a little more bouncy each hour toward the end, but my consumption was still on time thanks to my every 30 minute phone alarms and so the logging was the only thing that varied and I was still above-goal overall although trending downward slightly.
This spreadsheet means I can also summarize my total consumption across 25 hours: I consumed an eye-popping 817 grams of carbs; 365 grams of fat; 136 grams of protein; 16,775 mg of sodium; and 6,979 total calories. That matched the 98+ enzyme pills (and 33 electrolyte pills, which are 210 mg of sodium each and reflected in the overall sodium counts), so I also swallowed >131 pills in the 25 hour time period running. Wow.
It’s common to end up in a calorie deficit due to the hours and miles that an ultra demand of your body, but my watch estimates I burned around 8,000+ calories (maybe an undercount since it stopped itself a few times), so I didn’t have as big of a deficit as I had originally predicted.
There were so many (50!) opportunities to mess up my digestion, and I didn’t mess up once. I’m really proud of that! I also had such a variety of snack types and textures that even though I was never really hungry, I ate my snacks like clock work and didn’t get major palate fatigue or get to the point that I wanted to stop chewing and needed to switch to my backup list of liquid fuel. The only time I slightly felt off was when I did a Snickers for one snack at the end of my lap and then my next snack was hot mashed potatoes – combined, that was 390 calories (one of my top two hours of calorie consumption) and felt like a little too much food, either because of the calories or the volume of mashed potatoes. It was only a minor annoyance, though, and the feeling passed within another 15 minutes and I didn’t have issues with any other combination of snacks. I did get tired of peanut butter pretzel nuggets, because they’re drier than many of my other snacks and took a lot of water to swallow. So I stopped choosing those in lieu of my other snacks and left those as emergency backups.
Looking back, I wish I could have done something differently about my feet, but I don’t think there’s anything else I could have done. I changed socks and into dry shoes at every single lap. I dried them and tried to draw out water with hand sanitizer and Desitin. I lubricated with Squirrel Nut Butter and Desitin, and overall came out with very few blisters compared to my typical shorter long runs (e.g. 25-30 miles). But we did get 0.72 inches of rain in that 24 hour period, and a lot of it was dumped onto my feet in the 4-7am time period. If I’d had a way of knowing 24 hours in advance exactly when the rain was going to let up with enough confidence to delay the run for a day, it turns out it would’ve been drier, but the forecast before I started running was for similar chances of rain all weekend. The laws of feet physics and the timing was just not good, and that was out of my control. I’ll keep researching other strategies for wet feet management, but I think I had done everything I could, did it well, and it just was what it was.
Overall, I can’t think of anything else I would have changed (other than my training, it would have been swell not to have broken my toe and been not weight bearing for 6 weeks!). Fueling, electrolytes, enzymes, blood sugars, pacing, mental game: flawless. I was even picking up the pace and still running and walking 30:90 second intervals, and I think I would have continued to pick up the pace and pushed it to the finish, estimating that I would have come in under 32 hours overall for 100 miles (around a 19 min/mi average pace overall, or a bit under that).
But I chose to stop at 82 miles, and being willing to do that was a huge mental PR, too.
So I’m pleased, proud, and thrilled to have run an 82 mile ultramarathon, and physically and mentally feel better than I would have predicted would be possible after 24 hours.
One of the things I read trying to learn about best approaches for running 100 miles (an ultramarathon) is that it’s mostly mental and logistical challenges rather than physical, because after a certain point everyone is running much farther than they’ve ever trained and what makes the difference is how well you deal with the mental and logistical challenges and problem solving when you reach those points. I took that to heart and did a lot of pre-planning for my 100 mile run attempt. You can read more about the other types of prep and decision making that went into this, but the below is a more tactical “here’s how I organized” the different things I had been thinking about for months.
Route Planning and Pace Chart
First, you either need to plan your route (self-organized) or get the course map (organized race). This enables you to start to build out a pace chart. I did this first, because it then informed fueling strategy, planning, etc.
I laid out my route (7 laps, which later turned into 8 planned laps based on re-designing my routes). I had a column for the distance of each lap/segment, then a total distance column. This was mostly to make sure I had my distance add up to > 100 miles; otherwise I don’t care about the rolling distance total. I then built out a pace sheet with what I thought my paces would be. I’m very slow and run/walk, and planned to go as slow as possible at the start to be able to finish the entire distance. So while normally my running might be 14:00-15:30 min/mile pacing, I expected to want to start around 16:00-16:30 min/mi pace and that I’d likely slow over time. As a result, I started my pace chart with a 16min/mi pace and did a 17, 18, 19, 20, and 21 min/mi pace chart for each of my segments. This enabled me to estimate the time it would take to run each lap (segment) at each given pace, and also a clock time that I would be expected to roughly finish that lap.
I also created a dynamic pacing chart that I could use to simulate different paces throughout my run. This enabled me to estimate what happens if I start fast and slow down a little or a lot and how that influences my overall time and pacing. During my run, my husband as crew updated the actual time to help estimate what my next segment time would be based on both the last segment time and overall pace. This helped him determine when he needed to set an alarm to come back out and meet me, as well as remind him where he was meeting me each time based on the route.
You’ll notice I’ve highlighted to make sure I remember to change the date when I cross over midnight, to make sure the pace chart updates accurately.
(Again, note these are simulated/fake times. The dark shading suggests when it’ll be dark, due to the time of year I’m running.)
Fuel, Enzyme, and Electrolyte Estimates
These pace charts were useful for then estimating what I’d need when. Namely, how much fuel I’d need to prepare in bags for my husband to give me for each lap. I used the slower paces for each segment and my plan of fueling every 30 min to determine how much I needed. For example, if I’m fueling every 30 minutes, my second segment is 13.06 miles and I’d probably be running around or below a 17 min/mi pace at that point, which means it’ll be 3.7 hours or so. This is 7 snacks (one every 30 minutes, and I’ll be back before the next snack time for my refill). But, if I run slower, I want to round up slightly and add a snack to that estimate, so I put in 8 needed for that lap. I did that for all laps, rounding to the next hour and/or adding 1 to the estimate.
I also estimated my electrolytes similarly. I drink water and get my sodium and electrolytes via a combination of my fuel and electrolyte pills, with taking electrolyte pills every 45 minutes. Again, I used the slower pace times and the segment time to determine how many electrolyte pills I needed for the segment and listed those out.
Then, you’ll notice I also estimated “enzyme” needs. I have exocrine pancreatic insufficiency, known as EPI, which means I have to swallow enzymes anytime I eat anything to help my body digest it. Fun, right? Especially when I’m eating every 30 minutes across a 100 mile run and how many enzymes I need to take depends on what I’m eating! I typically take two (one each of two types) over the counter enzymes for a snack; although some bigger snacks I can take 2-3. Therefore, I estimated one per snack plus a few snacks where I’d take the 2-3, and also factored in dropping a few (it happens). It adds up to ~118 enzymes but again, that’s a lot of extra added in so I don’t have to worry about running out if I drop some or eat bigger snacks. I calculated I’d probably end up consuming closer to ~80 of each type (so 160-ish total) across the 100 miles.
Deciding What I Want to Eat, When
Next, I took these snack per segment estimates and decided what I actually wanted to eat. Based on my training, I ruled out some foods and perfected my list of what I wanted to eat and had practiced.
I listed all my preferred snacks down a column, then listed out the laps/segments in the row at the top. I then started playing around with what I wanted to eat at different times. Knowing I’d probably get tired of chewing crunchy things (for me it’s not the chewing but the texture of the harder things in my mouth), I put things like my chili cheese Fritos and peanut butter pretzel nuggets toward the first few laps. Later laps got easier to chew/swallow items like peanut butter M&M, fruit snacks, etc.
At the bottom you’ll notice I have a few different columns. A lot of the snacks indicated with numbers are ones that are shelf-stable and pre-packed. Others are snacks that are at home in the fridge or freezer or require prep (like mashed potatoes). I have a variety of quantities of those prepared (see right side of table) so I can choose any combination of 2 of those for my husband to bring out each lap, in addition to the pre-packed shelf-stable snacks. The bottom combinations make sure I have enough snacks between the pre-packed snacks and 2 fresh snacks every time, based on the above chart I had made to estimate how many snacks I needed for each segment.
The other reason this chart is helpful is that I know how many extras of everything I have at home, too. So while I have certain amounts prepped and packed per column Z; column AA notes the extras I have pre-packaged and sitting at home, so if I get tired in lap 3 of beef sticks and want to not eat those, I can figure out what other 4 snacks I want that I have prepped and have my husband bring those alternatives.
One other note for nutrition and macronutrients: I use a macronutrient fueling tracking spreadsheet to help me track my calorie intake as well as sodium intake, to make sure I’m getting enough on a rolling basis. It also helps me figure out how many enzymes to take for each snack, if I don’t know it off hand or my brain forgets (as it might after running for 20+ hours!). You can read more about how I built and use this fueling spreadsheet here.
Planning Supplies
Over the last few months and especially the last training runs, I built a list/library of likely common issues I experienced or had learned about by reading other people’s race recaps and reports that I wanted to be prepared for. I organized it by type of problem, then listed potential supplies and solutions. For example, I had a blisters/feet section; low sodium; high or low blood glucose (because I have type 1 diabetes); etc.
The solutions list here is unique to me/how I solve things, but here’s an example of what I would include:
Sodium
More electrolyte pills more frequently than 45 min
Short term fix: Chicken broth (¼ is 530mg sodium. Entire thing is 2120mg)
Less sodium but variety: GZero (no carb) gatorade sips – whole bottle 270mg
I then also started a separate document for 100M Prep. This included a long checklist of all the items I had brainstormed as solutions – so in the above sodium example, it included extra electrolyte pills; chicken broth; Gatorade Zero; etc.
This became helpful for me to a) make sure I had these things at home and to get them if I didn’t have them yet and b) to make sure I had set them out/organized them prior to my run so they’d be easily accessible for my husband to find.
The 100M Prep document also helped me break down larger tasks, too. Instead of “blister kit”, I started a sub-list that described everything I wanted in that baggie.
This also helped me realize when I needed to add a task for splitting supplies. For example, if I had a big tube of cream or ointment that I possibly wanted to be in two places (such as a certain type of foot lubricant). I had previously bought a bag of empty lip gloss tubes for making travel size toiletries (shampoo, face wash, etc.). I realized that they also worked great for liquid, gel, cream supplies for ultra running, too. And so I added tasks for splitting those into smaller tubes once I decided and listed where they should go and thus how many I needed.
I also had a checklist for each lap bag, which is a combination of which snacks (planned above) and other supplies (like eye drops) that I wanted to have each time. I made a checklist for each lap, then laid out all my supplies and checked them off the list for each lap. Once I had all the supplies laid out, I then compiled them into one bag for each lap and added a label. This way my husband has one bag to bring for each lap, and there is a sticky note on top of each bag that has anything else (e.g. 2 fresh food items from home) he needs to add and bring that lap.
(Again, this is planned food, electrolytes, and enzymes for each lap. See the above section to see how I estimated the food/snacks, electrolytes, and enzyme needs.)
I had started a list in a PDF for each lap, then printed the list for each lap on a sticky note so I could easily tape it to the bag and it would be easy for my husband to read.
Editor/Husband/Crew note from Scott: “These pre-prepped lap bags and printed sticky notes turned out to be most useful for making sure I got everything prepped each time. When I got home after each pit stop, I would pull out the next lap bag and make sure I had everything charging/washing/drying that I’d need at the next pit stop. Then when it got close to time to go, I’d work down the checklist, collecting each thing and putting it in my bike’s saddlebags, and then put the lap bag on top when I had everything packed.”
Crew Checklist
The same document as the overall solutions list became my Crew Checklist document. I added a checklist for what we should be doing at each lap. Again, this is unique to me, but it included things like putting my watch on the charger; removing trash from my vest; replacing water and ice in my hydration pack; replacing my battery for charging my phone; putting my fuel/enzymes/electrolytes into my vest and using eye drops; swapping socks; seeing if I need replacement supplies for low blood glucose; and after midnight considering whether I wanted to drink a Diet Mtn Dew for joy and caffeine.
You’ll also spot the section I added for my husband for after he gets home to remember to charge batteries on various things, use the pacing spreadsheet to help him figure out when to come back out, etc.
At the bottom of my crew document (the lap checklist is at the top, followed by the comprehensive solutions list), I also included an example pep talk section with constructive things to say. If there’s things you don’t want your crew to say (e.g. “you’re almost there!” or “only X hours left” are on my ‘please no’ list), you can also list those out. I also have my list of run-ending situations that my husband and I agreed upon, which includes things like having a broken bone; severe dehydration or peeing blood; hypothermia; etc.
And finally in the document at the very bottom, I created a checklist for post-race care so when I get home and everything feels terrible and I don’t know what to do, my husband has my pre-thought-of checklist of things in the best order (shower then compression sleeves; making sure I eat something within an hour of finishing; etc) to help me do all the self-care things I’m probably going to forget about.
Editor/Husband/Crew note from Scott: “Peace-time plans are of no particular value, but peace-time planning is indispensable” and “No plan of operations extends with any certainty beyond the first encounter with the main enemy forces.”
– This particular document ended most useful for pre-race planning purposes, including our night-before review of all the plans. I glanced at it a couple times during the race, but mostly relied on the lap-bag checklist and the physical presence of items in my saddlebags at the pit stops.
DanaWatch
The other thing I had prepared was a document with instructions for friends who had agreed to help out during the overnight hours for me. My husband was “on call” and crewing the whole time, but overnight there were sections where I was out running 3-4 hours and he needed those times to sleep. For those hours, we set up “DanaWatch” (as I call it), with a friend who will text me every half hour or so to check on me. If they don’t get a text back (a simple emoji or other text from my watch), they were to call me, and if they couldn’t reach me, they’d call Scott. So, the document has these instructions, an outline of my safety plan, Scott’s number, etc. so everyone knows what the plan is. I had friends staggered over different times. For example, a friend in the UK was to text me starting around 8am his time, which is midnight for me. When another friend wakes up on the east coast (three hours ahead of me), she’d starting texting me, and so on. This way I wouldn’t feel “alone” and would have extra folks watching out to make sure I’m still on track.
—
I think that’s everything I did to prep in advance! Mainly, having those documents built to add ideas to (especially problems and troubleshooting solutions) and building out my pace chart so I could progressively make my fuel, electrolyte, enzyme and supply plans in advance was really helpful. Then I blocked off time the week before my run to make sure I had everything prepped and ready to go well before the day before my race, so I wasn’t stressed about getting ready. As I described in my other preparation for ultra post, anything I could do to limit stress and mitigate decision-making fatigue, I did. And it definitely helped!
As I prepared for months for my first-ever 100 mile run, I did a lot of research to figure out how I should be prepared. There’s no one way to “prepare” for an ultramarathon of any distance, and much of the stuff online is about your training plan and physical preparations. Which is definitely important, but not the only thing that needs preparation.
After a lot of reading, thinking about my own plans and preparation, I’ve realized there are 4 general types of preparation for an ultramarathon that I’ve been doing: mental preparation and training; nutrition preparation and training; race day strategy preparation; and the actual physical training and running to prepare for an ultramarathon.
Usually, blog posts either cover the last category (training plans and physical training philosophies) or one of the other categories. This blog post summarizes everything I’ve done in all of these categories together in one place – in part to help me if I ever run another ultra following my first 100 mile attempt!
Mental preparation and training
It’s commonly said online that running 100 miles (or most ultra distances) is 80% mental and only 20% physical. (Or similar splits like 90/10). This is in part because it is not feasible to physically train to run the distance prior to your race (usually); and the first time you tackle a new distance, you always have many (often dozens!) of miles of distance that you’ve never covered before. It’s going to be uncomfortable, and you have to plan for that. Thus, mental preparation and training as much as possible to be prepared to deal with these challenges.
The first major aspect of this, for me, is practicing and reminding my brain how to process and work through discomfort. Discomfort is distinct from pain and being injured. (Pain and an injury should include evaluating whether you should cease your activity.) I’ve fortunately (and unfortunately) had recent experiences of pain when I broke my toe. Returning to walking and then running involved some discomfort as my body got used to covering miles again. It was a very distinct feeling that was not easily confused with pain from a broken bone, which to me feels like an “electrical” type of feeling.
This recent experience with pain is easy to differentiate from the discomfort of running long distances and being tired and sore. I’m working to capture these thoughts when I have them, and transition from “I’m tired and this hurts and this is terrible” during training runs and convert these thought patterns to “I’m tired and uncomfortable. But this is not pain; this is discomfort. This is how I’m going to feel at mile 34 or 57 or the back half of my 100M, and I’m going to keep running then and I’m going to keep running now to practice this feeling.” I want to register and save this feeling and mental state for what it’ll feel like during my 100M, so it’s easier to pull that out when I’m exhausted and uncomfortable at 3am and still likely have another 40-50 miles to go.
Similarly, I also try to envision different scenarios that I will experience in my “race” or 100 mile experience. In my case, I plan to run on a paved trail for a solo endeavor (DIY or self-organized, rather than an organized race with other people). Some of the scenarios I am expecting to experience and deal with include:
I will be running a course with 7 “laps” or loops of various lengths. This involves me coming back to the same point seven times so that I can get re-fueled by my crew (my husband), change clothes if needed, etc. I envision coming in for my second or third lap, having to turn around to head back out for another (but not my last) lap and not wanting to leave.
How I planned to deal with this scenario: I’ve written down crew instructions for my husband, which include how to refuel and replenish my supplies; a list of troubleshooting scenarios and supplies; but also specific things that would be constructive to say to me. In this instance, any of the following:
You are strong and you can do this.
You only have to do the current lap.
Walk as much as you need to.
This 100M will be one of the first times (other than a training run where I practice the transition) running all day and into the the night. I’m a little apprehensive about this idea of running for 14 hours in the dark (due to the time of year). Partially, this is because I’ve never run 14 hours before, and I’ll be doing it after already having run for 10 or so hours! And because I’m not as experienced running in the dark.
How I planned to deal with this scenario: I have a clear set of “day to night” transition supplies and instructions to gear up for the night. I will be equipped with reflective components on my vest; a bright colored shirt; a waist lamp; a head lamp; a blinky red light on the back of my vest. I will focus on getting geared up and recognizing that it’s a mental transition as well as a physical gear transition. I will also try to think about the novelty and adventure aspects of running through the night. It’ll probably be wet and cloudy – but it might clear up in patches enough to see some stars! And – the running through the night is something I didn’t think I could do, which is actually why I’m doing a 100M, to prove to myself that I can do anything I want to set my mind to. This is the purpose of being out here, and it’s a necessary part of achieving 100M.
At some point, most people do a lot of walking. I’m fairly unique in my “running” approach – I run/walk from the start, and also not like many people run/walk. In ultras, most folks walk every X minutes or when they reach hills. I consistently run/walk with 30s of running, then 60s or 90s of walking – from the very start. These are short intervals, but it’s what works well for me. But like everyone else, regardless of initial strategy, I expect there will be a time where it might be more efficient to try a brisk, consistent walk for a few minutes (or miles!), or a slow slog (inefficient walk) because that’s all I can convince myself to do.
How I planned to deal with this scenario: The goal is forward motion, however I can move. Walking is ok, and expected – and I will remind myself of that. I know there is a crossover point when running speed slows down to a certain degree and running becomes as efficient at a certain point. I also know these points, speeds, and effort levels will change throughout my 100M. It helps that I’m already a proactive walker; I have no shame, guilt, or hangups related to walking because it’s ½ or ⅔ of my forward motion strategy from the start! But I will remind myself that my plans for intervals can change and I can experiment to see what feels good throughout.
It’s possible that I could trip and fall, especially as I get tired and scuffle my feet on the trail, even though I’m on the paved trail. I also might get swooped by an owl or startled by something which causes me to trip and fall unexpectedly.
How I planned to deal with this scenario: I’ve got my safety plan in place (more on that below) and know I will first while on the ground disable the alarm on my watch so it does not call 911 (assuming this doesn’t appear to be needed). I will move my body to see if I’m just sore or if there are any scrapes or injuries that need addressing. I will stand up if possible, continuing to check myself out. I will slowly walk, if possible, and see how I feel. I’ll also probably call and let my husband know, and either ask him to come meet me earlier than expected that lap or just let him know so he can check on me when we meet up as planned. I will let myself walk any soreness off for a while (and turn off my interval alerts) before resuming a planned run/walk strategy.
So these are some of the scenarios I’m envisioning dealing with and my plans for them, with the hope and expectation that my brain will be better equipped to deal with them as a result of thinking about them in advance.
Depending on your race/route/plans, you might need to add other types of scenarios – such as leaving the aid station with warmth and light before heading into the night; or what to do if your crew doesn’t show up as planned; or your drop bag gets soaked with water; or the aid station is out of supplies or there is no one where you expect an aid station.
The other part of my mental preparation is a lot of pre-problem solving. Similar to the above scenarios, I have thought through what I need to do for the following:
I drop my fuel, enzymes, or electrolytes and can’t find them.
How I planned to deal with this scenario: I will call or text my husband and adjust plans for where he meets me. I will use the backup fuel supplies in my pack as needed to tide me over. (For my race, I have fuel in individual baggies and separated out for each “lap” or segment, plus extras and backups, so my husband can grab the backup bag or the next lap bag and bring it to me.)
I run out of water.
How I planned to deal with this scenario: There are 3-4 water fountains along or nearby my planned run route, and I can re-fill my hydration bladder within ~3 miles from any spot on the trail. I can also again call my husband and have him meet me sooner to re-fill my hydration pack.
My stomach gets upset.
How I planned to deal with this scenario: I have supplies (such as Immodium, GasX, Tums, etc) in my running pack that I can use. I also have more supplies laid out at home that I can ask my husband to bring.
I don’t feel like eating.
How I planned to deal with this scenario: I included this on the list because I read that it happens to a lot of people. But, as a person with type 1 diabetes…I have 20 years of practice of consuming sugar or food when my blood sugar is dropping or low, even when I’m not hungry. I have also practiced consistently fueling throughout my long runs, and I am used to eating when not hungry. I expect it is more likely that I will get tired of certain textures, so I have planned out my fuel so that “harder to chew” or crunchy foods that might hurt my mouth are the snacks I eat earlier, and then eat softer snacks or snacks that require less chewing later in the run. I also have a variety of backups that include different textures and some liquid options that I can substitute for my planned fuel.
Other scenarios I’ve pre-problem-solved are getting blisters or sore spots on my feet; chafing; getting low on sodium/electrolytes; muscles hurting on other parts of my body other than my feet; having feet that swell; getting itchy or having other types of allergic reactions; having trouble breathing; my eyes hurting; being really tired; being hot or cold or wet; my blood sugar staying higher or lower for a longer period of time; and mentally feeling “low” and unmotivated and wavering in the pursuit of my goal.
How I planned to deal with this scenario: As part of the ‘crew instruction’ list I’ve made for my husband, I have listed out all the supplies I have to address these categories. I will also have all of these supplies grouped and set out at home. My husband is awesome at troubleshooting problems in general, but he’ll also be tired at 2 am after only sleeping for 2 hours (plus I will be tired), so I created this to help me prep all the gear but also when I tell him “I’m ____”, he can offer the requisite supplies to address the problem without me having to try to figure out what my options are and decide what to do. All of this is to help mitigate the decision fatigue I will have and the overall fatigue he will have.
Note: I’ve also previously read a really good tip about managing decision fatigue. Tell your crew – in my case I’ve told my husband and written it onto the crew sheet – not to ask open-ended question, but to offer specific suggestions or options. For example, say “Do you want 2 or 2.5 liters of water in your hydration pack?” instead of “How much water do you want?”. For refilling my snacks, I’ve told my husband to refill my snack pack from the pre-filled bags, but the bag also has a sticky note about grabbing fresh prepared food. I told him to specifically ask “Do you want your waffle; sweet potato tots; mashed potatoes; or” (whatever is on my list of pre-prepared food for him to make and bring), instead of “What do you want?”
A lot of these I put on my list to think about based on race reports I’ve read from other people, that covers what they experienced (e.g. feet swelling and finding it helpful to have a half size bigger shoe to change into) and how they troubleshot things during the race while in between or at aid stations.
I have learned quite a bit and improved my planning and preparation by reading race reports of DNFs and also of finished races of different lengths. The longer the race, the more challenges there are and the more time to learn and sort them out. So that’s why I appreciate reading Wes’s multi day (eg 240 mile) recaps as well as 100 mile race reports, even though my focus has been on 50ks previously and now “just” a 100M.
One other thing I’ve thought about is the importance of knowing what your criteria for quitting/stopping/DNFing. For me this links back to discomfort versus pain. An injury should involve stopping temporarily and maybe permanently. But being tired, sore, uncomfortable – for me those should not qualify as reasons to stop. My goal is not to stop before 100 miles unless I have an actual injury (eg broken toe level pain).
2. Nutrition preparation and training
Yes, it’s worth “training” your nutrition. This means training your body by practicing fueling with the same foods and strategies as you want to use on your race. There’s a mantra of “nothing new on race day” that is both useful and not applicable to ultrarunning. In general, a lot of ultrarunners seem to do well (per my above search through many race reports) with eating small portions of “whatever looks good” at aid stations. If it looks good, their body is probably going to deal with it ok. But not always. And a lot of time people will bring fuel and rely on things they haven’t tested on their long runs prior to race day. Don’t be that person!
Test your fueling options and strategy (e.g. timing of fueling) on most runs, not just your very longest runs. For me, I do fuel for any runs of 2 hours or longer, because that correlates with when I bother to bring hydration and therefore also bring fuel. (That’s 8 miles for me at an average 15min/mile pace). Some folks use 1 hour or an hour and a half as their cutoff. But the point is – don’t just test your fuel on 6 hour runs. Fueling on shorter runs helps those runs feel better; you’ll likely recover from those runs more quickly; and it helps your body practice with those fueling options. You don’t want to find out at hour 8 of your 36 hour race that your body doesn’t do well with ___. It’s better to find that out at hour 3 of a 4 hour run, or similar.
Create your list of fuel that works for you. This should be based on your preferences but also how it helps you meet your fueling goals. When you have an idea for a new fuel, make sure you take it on your next run and try it. If you’re like me, you might want to try it near the end of your run, just in case your body doesn’t like it while running. If your body doesn’t like it, cross it off your list. You don’t want to be hauling or trying to eat food you know your body doesn’t like during a 100 mile run! I’ve found some things that I like to eat and found tasty fresh out of the oven – like ½ of a GF banana bread muffin – felt terrible in my mouth during runs. Some combination of the dry muffin (vs. freshly moist out of the oven) and the taste was not ideal for me. I ate it, and didn’t have GI distress, but I got home and promptly moved the remaining half portioned muffin baggies to my husband’s section of the fridge/freezer where my snack rejects go, and crossed it off my list. If it doesn’t bring you joy, or if it makes your brain cranky, it’s probably not a food you want for your ultra.
Don’t feel like there is a “wrong” food, as long as it’s something that’s not going to spoil easy or melt or be too hard to eat on the go. Look at snacks and meals you like to eat; is there a serving size or a variation that you like to eat? If so, try it! People eat all sorts of things in ultras, from puréed fruits and vegetables like applesauce or baby food pouches, to candy and chips to hamburgers and soup. Walk the store aisles (physically or virtually) and get ideas for food to try. But don’t limit yourself to sports “products” like blocks, gels, gu, drink mix, and similar. You’d be surprised about the variety of food that is portable, and in individual portions is close to the same macronutrients (calories, carbs, fat or protein, sodium, etc) as more expensive sports products. A lot of time you are paying for convenience and a certain texture/delivery method. But you can achieve the same intake of macronutrients through a variety of foods and beverages.
Some people stick with 1-2 foods or fuel sources (like liquid calorie/electrolyte solutions or gels/gu/blocks), but get tired of the sweet taste or the taste/texture of what they’re eating. Having a variety can help with this. Make your list, and for each run make sure you’re working through trying out and approving or removing the foods that you want to use during your race. Ideally, try them 1-2 times before your big run.
If you can, practice with some of the aid station type food including warm food (eg quesadilla or burger or whatever). Have someone meet you on longest runs with this freshly prepared, or take it with you and eat it for your first fuel. (Watch out for food spoiling/going bad – I always eat the hot/fresh prepared stuff first out of my set of fuel options when I get my pack refueled, to reduce the chance of bacteria growing or the food otherwise spoiling.) This is harder to do and may not be possible, but it could help expand your options for what you’re willing to take at aid stations if you’ve tested a version of a similar food before during a training run.
More planning ahead on nutrition for race day and training runs: figure out your timing of nutrition strategy and how many snacks or how much fuel (liquid or otherwise) you need to consume each hour or segment or between aid station. Pre-portion your fuel/snacks and if possible, label them. Plans can change and you can adapt on the fly, but having everything pre-portioned and ready to go means you can more easily start your training runs, fill your drop bags, or prep bags for your crew by having everything portioned out.
Planning ahead also means you get to the store or order however much you need so you’re not adding stress the last few days before you race or run in order to have your fuel set up and ready to go.
Don’t be afraid to use a timer. Some people wear running GPS watches that have alert/alarm features for fueling. You can use regular phone alarms, too, or apps like “Timer+” or “Intervals Pro” – both are ios apps that have free versions that allow one alarm each. You can choose whether it pushes a notification to your phone or watch or provides a verbal audio alert. I use both these apps and have one alarm that’s verbal audio reminding me to take electrolytes every 45 minutes; and the other one is a push-notification only that helps me remember to fuel roughly every 30 minutes. I generally am checking my watch so it’s easier to remember to fuel every :30 and 1:00 from when I start running, which is why I choose that one to be a push notification just in case. That works for me, but figure out your ideal timing and alert/alarm strategy to help you remember to fuel and electrolyte as you need to.
Since I’m running my ultra solo/DIY, I’m taking advantage of some fresh/heated fuel options, like mashed potatoes, ¼ of a ham and cheese (gluten-free) quesadilla, etc. For these, I am leaving a pre-printed sticky note on the baggie of shelf-stable fuel with a reminder for my husband to bring 2 of my fresh/hot options each time as well as anything else I need him to bring for that lap. To aid the bringing of the fresh/home food, I made a printed set of instructions that lists what these are, broken down by location (freezer, fridge, or on the counter) and instructions on how to make them. This is a critical step because what he predicts I want or how I want something to be cooked or prepped for a run doesn’t always match what I was wanting or expecting. Having clear instructions he can follow (eg heat ¼ quesadilla in microwave for 30s) works well for both of us and further helps with limiting his decision/processing fatigue since he’ll be responsible for grabbing and making 2 things; getting the lap bag of refuel; packing up ice and water; and getting all that and any other requested supplies out to the trail on time to refuel me as I pass by again.
If you have crew, think similarly about what food you want to have; how they’ll make it and serve it to you; how you’ll consume it at the aid station or as you move along on the trail. All of this planning will pay off.
(Another benefit of my macronutrient/fuel tracking spreadsheet is that my husband has access to it and can check it to see if I’m sticking to my fueling and electrolyte strategy, so he can troubleshoot and recommend things if I need support in fixing a problem. I don’t think he’ll use it much, but this secondary use of the spreadsheet was inspired by one of Heather Hart’s many excellent ultra posts talking about showing her empty fuel wrappers to her crew to prove that she was fueling. In my case, instead of counting wrappers, my husband can check my spreadsheet.)
3. Race day strategy (and pre-race and post-race strategy)
Continuing on the theme of pre-planning and laying out your strategy, I also think about strategy related to race day and leading up to race day as well as after race day.
My goal is to eliminate stress; pre-do as much work as I can physically and mentally to reduce the load when I will be physically and cognitively fatigued and overloaded.
Pre-race
For example, I look at my schedule prior to the race and try to clear out stressful activities (or prevent scheduling them, if possible). I know I’ll need to spend hours physically prepping (per above, making fuel and organizing supplies), so I put that on a to-do list and make a block of time on my calendar for it. I think about tasks that I will have before and after the race, such as changing my continuous glucose monitor (CGM) and pump sites to be in optimal locations on my body for the race; but also changing them early enough prior to the race so that they are settled in and I know they are working well. I also do things like pre-fill my reservoirs with insulin, and do enough reservoirs for a few days before and a week or so after the race. Like during the race, anything I can do to help reduce cognitive fatigue or pre-do steps of tasks that I know I will find harder to do is the goal.
This includes also blocking off my schedule with reminders to go to bed earlier. I think about when I’ll be waking up on race day and the night before, set my bedtime reminder for about 8 hours prior. Then every day before that I set it 15 minutes later, working back about a week and a half. I don’t always hit these sleep times, but progressively slightly shifting my sleep like this has been effective prior to international trips with a lot of time zone changes and also has paid off for getting a better night’s sleep the night or two before a race that involves waking up early.
I also specifically think through all the steps from waking up to starting my race, and how to optimize those. I eat a particular breakfast prior to the race, time it so that I can best get some macronutrients in, and time the insulin so I don’t have much of a BG spike but also then don’t have much insulin activity happening when I start my run. I don’t always get this right, but I attempt to line up my schedule so that I wake up and immediately eat what I have laid out on my bedside table and start hydrating, so that I can sleep as long as possible and don’t have to spend extra minutes convincing myself to get out of bed to go make breakfast. Some of these strategies are unique to me being a person with insulin-requiring (in my case, type 1) diabetes; but it’s pretty common for other ultrarunners to have strategies around what to eat the morning before a race; how many hours prior to the race; etc. I’d suggest you decide based on first principles and your own knowledge what to do for you.
Pro tip/personal vent: most people who blog or write about “avoiding insulin spikes” prior to the race or during the race – if they don’t actually administer exogenous insulin (aka inject or pump it, their pancreas makes it) – they also don’t usually actually know anything about the insulin response to food in their body. They are mostly repeating that from hearing it from others who repeat it from a long chain of people. You are SUPPOSED to spike insulin in response to what you’re eating: that’s good because it manages your blood glucose levels and helps your body process and store what it needs to be storing. It is also very normal for your blood sugar to rise in response to eating. The only people who need to think about “insulin spikes” are people who don’t think about it as insulin “spikes” but as insulin activity or more commonly “insulin on board” (IOB), which are people with insulin-requiring diabetes. This is different for us because we have to inject/pump insulin separately (our pancreases don’t make it on demand in response to sensing food in our bodies) AND because the insulin we use takes longer to act – 45-60 minutes instead of mere minutes – as well as has an hours-long “tail” effect. So it’s a lot of work to match the peak timing of insulin to the impact of different types of food in our bodies as well as watching out for insulin “stacking” over the many-hour activity curve for each dose. Your body, if you don’t have insulin-requiring diabetes? It does this, on its own, like magic. Yay, you! So ignore the stuff about “avoiding insulin spikes” and focus instead on things like whether the food feels heavy in your stomach when you run or gives you GI distress or otherwise doesn’t make you feel good. If it doesn’t, try different food and try different timing.
4. Race start and race strategy
You should definitely have a plan for how you run your race. In my case, because I’m a run/walker, I think about which set of intervals I will start at (likely 30:90, meaning 30s run and 90s walk, because that’s also how I train and helps me achieve my easy effort and easy paces). My goal is to start easy and limit excitement. Since I’m solo running, I don’t get swept up in other people running and racing. But, I always find the start and the first mile to be hard. So my strategy instead is to start, make sure all my intervals and run trackers are turned on; my electrolyte and fuel timers are set; and that I get my audiobook or podcast going. I troubleshoot any of these as needed on the walk intervals as I get going. I specifically try not to think about pace, especially the first half mile, nor how it’s feeling so I don’t catastrophize. I know the first 0.75 miles or so always feels pretty rough, so I aim to do no foreshadowing of how anything else is going to feel.
For most people running organized races, it helps to have studied the course maps and elevation profiles. Learn the course by heart, in terms of knowing how many miles to each aid station and what the elevation profile is like, and what your strategy is for each section. This means having a pace plan from the start and if you are going way too fast (due to excitement and other people around you), switching to walk breaks to help moderate your pace if you can’t slow your run pace down on its own. It also might help to not only have a pace plan but to also put time estimates on aid stations or check points. Use any extra time – especially if you are far ahead – to address any issues popping up (chafing, blisters or hot spots on your feet, etc.). Don’t start foreshadowing and forecasting that you can hold this too-fast pace through the whole race. You likely can’t (physically), and skipping the plan to stop and address issues will also doubly backfire later.
Even though I’m not running an organized race, this is still something I struggle with. I’m setting the goal to stop for bathroom breaks or shoe re-lacing or hotspot fixing in the first out and back “lap”, recognizing that it will help get my average time here to slow down a bit and keep me from powering through it too hard based on initial excitement. My goal is to make sure I don’t skimp on self-support (e.g. foot care or re-applying anti-chafe) by folding that it in to my goal pacing.
In general, though, because I’m running a 7 “lap” course, I focus on each lap. And only that lap. I’m running known out-and-back or triangle shaped “loops” that I know and love, so I can treat the first out-and-back like a long extra-easy run and settle in to watch landmarks while I listen to my audiobook and focus solely on managing effort. When I get back after the first loop and refill my vest, I then can think about the lap that I’m on (13 miles next, a much shorter loop). When I’m back, then I think about the next out and back (about 16 miles). And so on. My goal is to never think about how much time or distance is left. I’m not good at “running the mile I’m in”, as people often advise, but I am fairly good at focusing on a sub-component and the process overall. So focusing on each lap, and knowing there are 7 laps of varying lengths, helps me compartmentalize the experience. I’ll run ¼ of the first out and back in the dark and transition into the daylight; the second lap should also be during the day; then I’ll transition to my night gear for the third lap and be in the dark on the 4th, 5th, and 6th lap. I don’t have aid stations or elevation changes to really break up the course, but since I know the course and all the landmarks well, even with the variable distance “laps”, that aids me in knowing what to watch for and keep moving toward, even if I transition to a walk or get off track pace-wise from problem solving and am trying to re-orient myself again afterward.
It’s good to think about what supplies you’ll carry versus what you will have access to at aid stations, what you have in drop bags, and what your crew will have. I generally carry most of my needed first-aid/don’t feel good supplies on me: anti-chafing, kinesio tape for blisters or muscles, anti-nausea medication, etc. But I have a set of supplies prepped and ready for my husband (who is my crew) to bring to me if needed. I won’t have aid stations, so I think about my planned re-fuel stops as aid stations where he’ll primarily be. If something gets really bad, though, he can bike out to meet me. In some races you may have crew access to the trails wherever you need them; in other races, they are not allowed or able to access you outside designated points. Plan and carry supplies accordingly.
And, plan for your crew how to help you and how you’ll communicate with them. I will have cell service on my run, so I plan to text my husband to give him updates (in addition, he can geo-track my phone’s location) of when I’m on or off the last predicted pace to a refuel stop; what I want him to bring (e.g. the 2 hot/fresh food items, or any extra supplies from my laid-out stash); and how it’s going. We have practiced on training runs for him to grab my vest and refill ice and water, fuel, electrolytes/enzymes/eye drops, then bring it back to me (biking) or when I re-pass him after I’ve turned around and come back to the spot where he is per my course plan. But I also expect him, as crew, to also get tired and mentally fatigued, so I’ve made a checklist that he will use to make sure he completes the steps every lap. There’s also a checklist for day to night transition and night to day transition. This is in the same online document as my expert list of supplies and strategies to troubleshoot every issues, so he doesn’t have to guess what the good options are for fixing blisters or low sodium or whatever the issue may be. He runs, but he doesn’t do ultra runs, and regardless everyone is different in terms of what works for them and especially what works for them at different stages of an ultra; thus, having this crew guide or checklist or supply/strategy “cheatsheet” is a benefit, especially as both he and I get more and more tired through the night.
My strategy also includes making sure my devices stay powered. I always carry a small battery and a charging cord for my phone, and will keep my phone power topped off. This is because I use it for run tracking; geolocation for my crew (husband); fuel/electrolyte reminders; fuel tracking via my spreadsheet; and it is the “receiver” for my CGM so I know what my blood sugars are. Thus, it’s a mission-critical device and I always like to keep it charged. I will also grab a watch charger from my husband after a certain number of laps to top off the charge on my watch 1-2x, based on how it’s battery is doing. He’ll replace the battery in my vest each time after I’ve used it (we’ve got 2-3 small batteries for this purpose so he can take one home and re-charge it while I’m using the other, plus another backup). My phone then also serves as an emergency back-up light if my other two lights fail at night.
Speaking of lights and night gear, have a plan for when and how you’ll transition to night gear. Because I’m running a solo/DIY race and I’m not experienced at running at night (although I’ll do a run or two in training to practice the transition and my gear), I’m actually choosing to start my run at 6am so I run about 1.5-2 hours in the dark at the start of my race. Why? My husband doesn’t believe it’s necessary and is still arguing with me about it, but my strategy is intentional. I want to start the run in my lights and night gear and practice running in the dark again so that I can see if I need to tweak or adjust it for later that night around 6pm when I need to run in the dark again. This gives me one more practice round and mentally will help me – or at least, that’s the goal – know what it’s like to run in the dark. Given that I’ll run in the dark for 14h overnight, I don’t want to pick up my lights and take off and be 6-8 miles down trail from my husband and my backup gear if I realize something isn’t working well. I know I’ll be prone to just sticking it out for the entire lap; this way, I get a mini, 1.5h test of the gear on the same day and that way when I do a 3-5 hour first lap in the dark that evening, it’ll be slightly more likely to go smoothly and I’ll take all the smoothing I can get for my first 100M and my first all night and overnight run!
My other strategy involves self-care in the sense of regular medications that I need. Of course, I’ll be managing my blood sugars and insulin very carefully all day throughout (often thinking about it every 10-15 minutes to make sure everything is on track). But I also take allergy medication twice a day at morning and night, as well as a thyroid medication at night. So I have set reminders on my husband’s calendar to make sure he brings out my bags of night medication (e.g. allergy and thyroid) and in the morning (allergy) medication to make it less likely that I’ll forget to take them. Thankfully if I mess this up and am super delayed or forget to take them, it won’t derail my race/run much, but I definitely will feel not taking my allergy medication within hours so that will also help me remember to take my thyroid evening medication, too.
Another self-care strategy is around keeping my eyes hydrated with eye drops on a regular basis. In October 2021 I started to have really dry, gritty eyes and went to my eye doctor and was diagnosed with…dry, gritty eyes. Helpful! But, sarcasm aside (I love my eye doctor), I got eye gel to use before bedtime and eye drops to use throughout the day. Then in August 2022 I realized I had subclinical hyperthyroidism from Graves’ disease, which is an autoimmune disease (to go with type 1 diabetes, celiac disease, and exocrine pancreatic insufficiency) that causes eye issues. So! My dry gritty eyes were a precursor to my thyroid level changes. At any rate, learning how and when to use eye drops has become routine and I know how helpful it is to keep my eyes lubricated. I use preservative-free eye drops, not because the preservatives bother my eyes but because they come in miniature vials that are very easy to put in your pocket. Supposedly they are designed to be single use, but they usually contain enough lubrication for 2-3 rounds of drops for both eyes. So I twist off the lid, drop in both eyes, put the lid back on, and stuff it back in my pocket. I have set reminders on my calendar during the run to do this every few hours in case I forget, but I have also put vials in each lap bag (along with electrolytes and enzymes) and this presence of new eye drop mini-vials will help remind me (hopefully) to stay on top of eye lubrication.
Keeping my eyes from getting dry will hopefully help me be able to wear my contacts longer, because I usually take them out at night. But, I also will have my husband ready with my contact case and contact solution to take them out; then I will switch to my glasses or run without them (because I don’t need to see far or read signs off in the distance) for some period of hours, while still using the eye drops to keep them happy.
I’m fairly nervous about my eyes being an issue, since I’ve never run this long or all night. This was exacerbated by reading race recaps where folks talked about losing their vision! Yikes! I read a little bit more and realized they’re talking about corneal edema, where there is temporary swelling in the edema that makes your retinas visually look cloudy (if someone else looks at your eye). It usually goes away when people stop running after a few hours or day. But given my eye issues, before I had realized I was dealing with eye stuff related to Graves’ disease and thyroid stuff, I was concerned that my tendency to dry/gritty eyes would make me at higher risk of this, even though it seems like only 1-2% of 100M finishers ever deal with this. But, like everything else, I decided to have a strategy for this. I’ll seek to prevent it with regular lubrication and if it’s cold and windy, using my glasses (in lieu of contacts) or clear biker glasses or sunglasses to help protect my eyes from irritation and drying out further. But if it does happen, I’m using the advice from this post and bought a small vial of 5% hypertonic eye drops to use and try. (I had a regular annual eye doctor appointment a month prior, so I checked with my eye doctor about this. She had never heard of it and consulted a cornea specialist who had also not heard of it, which helps confirm that it’s pretty rare! Although they admitted they don’t get a lot of endurance athletes, looked it up on PubMed like I had, and agreed that if it happens to try the 5% hypertonic eye drops. Note that contact wearers want to take the contacts out before using these drops.) If I start to have vision issues; and I have the clear visual symptoms of this (according to Scott’s assessment of looking at my eyeballs); I’ll try the eye drops and ideally they’ll help. Since this is a known issue, if I still have some vision and can run safely (given my 6 foot wide paved trail in a safe location with no navigation required); I will likely try to continue – again based on discussion and advice with my doctor. But having a plan for this is much better than suddenly having vision issues in the ultra and feeling like I need to abort, when it might be ok to continue running (again on advice from my doctor).
Another strategy is thinking about how I’ll use caffeine. I usually drink caffeine up until noon, then switch to caffeine-free diet soda (and more water) in the afternoon and evening. I’ll drink a diet Mtn Dew when I wake up with my breakfast, but only one, and I will aim not to drink any throughout the day and save them for after midnight, when I’ll have been running for 18+ hours and have spent 6 hours in the dark. That way I have a “pick me up” to look forward to, both in terms of the taste/flavor of diet Mtn Dew, which I love, and some caffeine. There’s some suggestion that weaning off caffeine in the weeks prior to the race would make this a more effective strategy; but for me I think removing the joy of diet Mtn Dew would not be a net benefit. I’m also not convinced that I know what amount of caffeine is needed for an overnight boost, nor that I can test this reliably enough to have a solid evidence-based strategy here. So instead, I’m likely going for the mental boost of the taste change and the placebo effect of thinking the caffeine is helping. I have, however, tested drinking a diet Mtn Dew during a long run in the morning; so I do know that my body is ok taking it in.
This is yet another example of how I’m trying to remove decision-making during the race by pre-planning wherever possible for decisions like when to take caffeine or not; what to eat when; etc. I have laid out pacing sheets for a wide variety of run paces – so wide that the fastest pace (if all goes amazingly well) would have me finishing 8 hours faster than the slowest pace I have charted out. But the reason this matters is because I’m using the slowest time to estimate how much fuel I need to have prepared, then preparing more as backups (see more detail in the nutrition section). I created my overall fuel list then started putting in estimates of how many of each I would be willing to consume, also factoring in palate fatigue and texture fatigue and not wanting to chew or put ‘hard’ things (like Fritos) into my mouth in the later hours of my run. I balanced all of these variables and came up with 6 max servings of my chili cheese Fritos, most of which will be consumed in the earlier hours; 6 max servings of a few other routine things I can eat in most situations, then smaller counts (eg 1-4) of other things like the hot/home food that my husband will bring out in addition to the shelf-stable food. Once I had my overall counts totaling enough fuel for the slowest hour estimate and the number of servings; I then made a lap-by-lap list of what I wanted to eat when. I’m going to prepare these bags with the numbers I need per lap based on the timing (e.g. 10 snacks for the slowest pace estimated for my longest lap in between refuels, of which 8 are shelf stable and 2 will be added based on the sticky note reminder for the fresh/home options). Each of these lap bags will also include the requisite number of electrolyte pills I need, based on similar estimates from my “slow” paces, and the enzymes I need (because I have exocrine pancreatic insufficiency and need these to actually digest the fuel I consume), plus new eye drops. The point of this strategy is to remove decision making for both me and my husband: we don’t need to figure out how many enzymes or electrolytes I have “left” from the last lap (because I am off my fueling plan or more likely because I packed extra for each); instead, he can simply pull out all the trash, old enzyme/electrolyte bags, and replace with the new fuel, electrolyte, and enzymes along with my water/ice refill.
You may not have the complexity of my situation (type 1 diabetes, celiac, exocrine pancreatic insufficiency) influencing your fueling strategy and choices and how you’ll deal with fuel on the run. But, you might want to consider similarly planning your fuel. You may need to adapt your strategy based on how you’re feeling and what options you have in your pack, drop bag, with crew, or at an aid station, but you can plan for options to address issues of fatigue, palate/texture fatigue, etc. That, essentially, is what I have done.
Finally, I also consider a safety strategy part of my important race planning. I wear a watch that will generate an SOS alert and call emergency services if I fall during a run. I have the ability to press and hold a button on my watch or my phone to similarly generate an emergency services call. My location is tracked by my husband (and my mom from afar); and my husband also has access to my CGM for blood glucose tracking. He’ll have extra alerts and alarms set at different thresholds than we typically do for glucose levels. Finally, we’ve also created what I call the “DanaWatch” plan/squad, which is 3 people who will be texting me periodically from midnight to 9am my time, which is the overnight hours when Scott will be intermittently sleeping for 1-2 hour snatches in between refueling me. The plan is for my friend in the UK to text me every half hour and watch for a response that I’ll generate from my watch – probably a simple thumbs up emoji or tapping one of the auto-generated responses like “thanks” or “hi” or “I’m good”. After a few hours, a friend on the east coast will take over. Then my mom in central time zone after she wakes up will start texting. Nothing fancy, but the point is that they have ensured I’m still moving and ok. If I don’t respond within 5 minutes, they’ll call me; if I don’t pick up the phone, they’ll call Scott. This means that there wouldn’t be more than about 30 minutes where I’m not actively being “watched” virtually in case I get swooped by an owl, fall down and hit my head and am too disoriented to call for help (or some other very rare situation). I don’t expect that will happen; but I also think I’ll appreciate the “company” since I’m again, running a solo, DIY race where there aren’t aid stations, other runners, and other crew out and about to cheer me on. It’ll also help my husband sleep better/feel better, so any of those reasons are worth this strategy!
Post-race strategy
Like pre-race strategy, post-race strategy and planning is also critical for me. Once I cross the finish “line” and stop, I get cold and start to feel being wet (from sweat or rain) very quickly. My feet and everything hurt even more. I am absolutely not hungry despite knowing I need to re-fuel. But later I am ravenously hungry like a switch has shifted. So I plan accordingly.
First up, gear change. I want to change into dry clothes. I remind my husband to remind me that yes, despite the pain/hassle of getting out of a wet sports bra and changing it, I’ll regret not changing out of it in addition to changing my shirt. Sometimes, if we are getting in the car to drive home, I quickly swap to a dry shirt and then take the sports bra off under my shirt and just leave it off. No need for gymnastics to put another one on if I am just riding in the car. Same with shoes: once I take my sneakers off, my feet will not want to go back in sneakers. Definitely not the same sweaty, dirty shoes I was running in, but also not cleaner and even bigger shoes. Instead, I prefer sandals/arch support flip flops. I have those, compression sleeves, and my clean dry clothes ready to go. I learned after my first trail marathon how good a washcloth feels for rubbing off sweat and dirt, so I also have a washcloth. It works for removing masses of mud before you get in the car, too. Or if you’re not muddy and hot and sweaty, pouring some cool water on it and washing your face feels heavenly.
Next up is fueling. When running an organized race, I don’t want to eat any of the race food, even if I can have it. (By “can have it” I mean that it’s safely gluten free with no cross-contamination risk, since I have celiac disease.) Usually I can’t have it, and I plan accordingly to bring food that is not the same food I’ve been eating throughout my ultra (because I have palate fatigue). I don’t want to eat as soon as I stop running, but usually after changing in the car and driving off, my body switches into “you’re safe” mode and wants to start refueling. Make sure you have all your food in the seat with you so you don’t have to stop and dig it out; or worse, have to try to twist around or reach for it (because you won’t want to do that most likely).
And again, you may have palate fatigue or similar (or it may disappear as soon as you are done), so having a few good options will be useful.
I also try to get enough groceries and prepare food for the following several days, too, when I’ll still be hungrier and making up for burned energy. My motivation to cook/prepare/put together food will be low, so having a stocked fridge and freezer with easy to prepare food is important.
Also, you may not be driving home from your race (or being driven home), so make sure to plan your logistics accordingly. Can you get to the airport that same day? Should you? Do you want to? And the next day? Is it safe to fly in your physical state? What different supplies do you need for flying that might be different (due to security regulations around liquid etc) than you would if you were driving home? Do you have enough snacks/food for the travel days following your run?
Training strategy
Oh, and yes, you have to physically train for your ultra. I am by no means a coach or an expert ultra runner. I am a solid, places-from-last back-of-the-pack runner who is a consistent run/walker. So get or make a training plan (Heather Hart has some great free ones for various distances). And stick to it. Except for when you don’t stick to it.
Wait, what?
You set your training strategy for “if all goes well”, but also build in flexibility and extra time for when things don’t go well. Like wildfire smoke season making it unsafe to run outside for a few days or weeks. Or you break your toe and spend 4 weeks not weight bearing. Or you have a lot of life stress, child or parental care, job stress, or any number of things. All this stress impacts training. Give yourself grace and be prepared to be flexible.
I have a hard time with this; I like my spreadsheets and my plans. But wildfire smoke and a broken toe were part of my 2022 ultra training experience this year, and I had to adjust training (and race plans) accordingly. At some point, you have to make the go/no-go decision about whether you’re going to run your race.
Think about what the “ideal training” is. Think about what is the “minimum training” to complete your event safety. If you’re somewhere in between, it’s going to be mental training and planning that can make the difference. At some point, if you’re above ‘minimum’ training you can decide to run even if your training isn’t ideal. Remember, it probably won’t be ideal and it isn’t for a lot of people. But per the mental training section and the wisdom I’ve gained from a lot of ultra runners…the most important factor might be deciding to do it. If you decide to, barring injury during the race or an accident, you will. If you decide mid-race you can’t or don’t want to, likely you won’t.
I think one thing I observe people not training is their walking strategy. Mine is baked in, because all my training short and long runs are intervals of run/walk. Many folks talk about walking hills or walking X minutes per Y minutes or Z miles. If that’s the plan for your race, train it during long runs. Walk hills or powerwalk or hike hills during runs or at the ends of runs. Practice a slow walk mixed in or a faster more efficient power walk. This will help build different muscles and help you maintain more efficient form (and speed) when you shift to it during the race, and help you go longer.
Similarly, practice with your vest/pack/handheld and other hydration gear. Practice with a similar stuffed and weighted pack. Practice with your head lamp. Do a run early in the morning as it transitions from dark to light; do a run into the evening as it transitions from light to dark to get used to your gear; practice troubleshooting it; and to improve your strategy for these transitions. If it’s wildfiresmoke season where you live, practice running masked as well. (On my last long run, I wore my mask for the full 8 hour run because air quality was so yucky.)
Also train and practice with your crew, if possible. Especially things like helping them tape or lubricate, tying your shoes, helping you put your pack on, them packing your pack/vest with supplies, etc. Any of these steps can be practiced during a training run so you and they can figure out what questions and assumptions you each have, and to build the crew checklist and instructions.
In my case, I’ve trained with my husband on refilling my ice and water in my pack during several training runs and previous races. We haven’t trained yet on him re-packing my (new) vest, though, so that’s on our list to practice on runs heading into my 100M. We did practice one run where I needed him to pick me up at a trail construction closure and drive me to the other side, with him bringing me a fresh/hot home-prepared fuel option. It worked well to a degree; I had a ¼ ham and cheese quesadilla slice in the microwave and had told him how to microwave it, which I had factored in cooling time for when he would be driving it to me before I would eat it. But he also tried to optimize and then put it in our car-based portable food warmer, which doesn’t do well with plastic bags (it needs a tupperware container) in general and was way too much heat. So it was scalding hot when I got in the car! Oops. Lesson learned. That was maybe unique to the car scenario but we will also test and practice the other food warming up options to make sure he doesn’t accidentally re-optimize where I’ve already optimized the food process; and make sure I have in fact optimally optimized the food strategy for each item.
Conclusion
Wow, that’s a lot of planning and strategy now that I’ve written it all out. Which makes sense, because I’ve been thinking about all these things for months and iterating on my strategies and plans. Hopefully, it’ll pay off and help immensely with making my 100M experience more smooth (note that I doubt any 100M would be easy/easier but I hope for “smoother”!) than it otherwise would be.
In summary, I pre-plan mentally for how it’ll feel running; I attempt to solve as many problems in advance as I can and prep supplies for fixing problems; I test, plan, and practice my fueling as much as possible; I aim to carefully pace effort as well as speed during my run; I break my run up into mental chunks so I am not dwelling on what’s to come but focusing on running the current segment; I try to minimize decision fatigue during and after the race by pre-doing anything I can and pre-supplying myself to make it easier; and of course, I train for months to prepare physically as best as possible while realizing that my training might not ever be ideal but that I can still safely attempt to run 100 miles.
PS – if there are any strategies, tips, or approaches you take to ultrarunning, especially 100 miles or more distance-wise, I’d love to hear them! Please share them in the comments or link to any posts you’ve written. I’m still learning and likely will always be evolving my strategies!
—
Note: I wrote this post before my 100 mile attempt. I ended up completing 82 miles and happily choosing to stop, knowing that I could physically keep going. Looking back at the above and reflecting on my experiences, I didn’t have a single challenge or experience that I wasn’t prepared to deal with or couldn’t deal with, thanks to all of the above work. So I’m thrilled and proud of my 82 mile experience!
One area that I’ve noticed is frequently misunderstood is how “open source” and “DIY” are different.
Open source means that the source code is openly available to view. There are different licenses with open source; most allow you to also take and reuse and modify the code however you like. Some “copy-left” licenses commercial entities to open-source any software they build using such code. Most companies can and do use open source code, too, although in healthcare most algorithms and other code related to FDA-regulated activity is proprietary. Most open source licenses allow free individual use.
For example, OpenAPS is open source. You can find the core code of the algorithm here, hosted on Github, and read every line of code. You can take it, copy it, use it as-is or modify it however you like, because the MIT license we put on the code says you can!
As an individual, you can choose to use the open source code to “DIY” (do-it-yourself) an automated insulin delivery system. You’re DIY-ing, meaning you’re building it yourself rather than buying it or a service from a company.
In other words, you can DIY with open source. But open source and DIY are not the same thing!
Open source can and is usually is used commercially in most industries. In healthcare and in diabetes specifically, there are only a few examples of this. For OpenAPS, as you can read in our plain language reference design, we wanted companies to use our code as well as individuals (who would DIY with it). There’s at least one commercial company now using ideas from the OpenAPS codebase and our safety design as a safety layer against their ML algorithm, to make sure that the insulin dosing decisions are checked against our safety design. How cool!
However, they’re a company, and they have wrapped up their combination of proprietary software and the open source software they have implemented, gotten a CE mark (European equivalent of FDA approval), and commercialized and sold their AID product to people with diabetes in Europe. So, those customers/users/people with diabetes are benefitting from open source, although they are not DIY-ing their AID.
Outside of healthcare, open source is used far more pervasively. Have you ever used Zoom? Zoom uses open source; you then use Zoom, although not in a DIY way. Same with Firefox, the browser. Ever heard of Adobe? They use open source. Facebook. Google. IBM. Intel. LinkedIn. Microsoft. Netflix. Oracle. Samsung. Twitter. Nearly every product or service you use is built with, depends on, or contains open source components. Often times open source is more commonly used by companies to then provide products to users – but not always.
So, to more easily understand how to talk about open source vs DIY:
The CREATE trial used a version of open source software and algorithm (the OpenAPS algorithm inside a modified version of the AndroidAPS application) in the study.
The study was NOT on “DIY” automated insulin delivery; the AID system was handed/provided to participants in the study. There was no DIY component in the study, although the same software is used both in the study and in the real world community by those who do DIY it. Instead, the point of the trial was to study the safety and efficacy of this version of open source AID.
Open source is not the same as DIY.
OpenAPS is open source and can be used by anyone – companies that want to commercialize, or individuals who want to DIY. For more information about our vision for this, check out the OpenAPS plain language reference design.
In 2020 we had a bad wildfire smoke year with days of record-high heat and poor air quality. It was especially problematic in the greater Seattle area and Pacific Northwest (PNW) where most people don’t have air conditioning. I previously wrote about some of our strategies here, such as box fans with furnace filters; additional air purifiers; and n95 masks. All of those are strategies we have continued to use in the following years, and while our big HEPA air purifier felt expensive at the time, it was a good investment and has definitely done what it needs to do.
This year, we got to September 2022 before we had bad wildfire smoke. I had been crossing my fingers and hoped we’d skip it entirely, but nope. Thankfully, we didn’t have the record heat and the smoke at the same time, but we did end up having smoke blowing in from other states, and then a local wildfire 30-40 miles away that has been making things tricky for several days on and off…several different times.
I’ve been training for an ultramarathon, so it’s been frustrating to have to look not only at the weather but also the air quality to determine how/when to run. I don’t necessarily have a medical condition that makes me higher risk to poor air quality (that I know of), but I think there’s some correlation with being allergic to a lot of environmental things (like dust, mold, trees, grass, etc) that makes it so that I also am more sensitive to most people I know to poor air quality.
Everyone’s sensitivity is different, but I’ve been figuring out thanks to multiple stretches of up and down AQI that my threshold for masking outside is about 50 AQI. If it gets to be around 100 or above, I don’t want to be walking or running outside, even with a mask. And as it gets above 150 outside, it becomes yucky inside for me, too, even with the doors and windows closed, the vents on our windows taped shut, and air purifiers and box fans etc running. My throat was scratchy and my eyes hurt, and my chest started to feel yucky, too.
It got so bad last week that I took a small, portable mini air purifier that I had bought to help mitigate COVID-19 exposure on planes, and stuck it in front of my face. It noticeably made my throat stop feeling scratchy, so it was clearly cleaning the air to a degree. On the worst days, I’ve been sitting at my desk working with the stream of air blowing in my face, and I’ve also been leaving it turned on and pointed at my face overnight.
This is kind of a subjective, arbitrary “this helps”, but today we ended up being able to quantify how much it helps to have our big air purifier, box fans with furnace filters, smaller air purifier, and the mini air purifier. Scott ordered a small, portable PM2.5 / PM10 monitor to be able to see what the PM2.5 and PM10 levels are in that exact spot, as opposed to relying on IQAir or similar locally reported sensors that only tell us generally how bad things are in our area.
It also turned out to be useful for checking how effective each of our things are.
It turns out that our box fans with furnace filters taped to the back are most effective at fan speed “1” (they all go up to 3), probably because putting it up to 3 is prone to stirring up dust from the floor (despite robot vacuuming multiple times of day) and increasing PM10 levels. A box fan with 2” MERV 10 filter taped to the back doesn’t affect the already-low PM2.5 levels indoors; on fan level 1 the PM10 gets reduced to zero as long as it’s not pointed at the carpet and stirring up dust. So while it doesn’t help with smoke, these fans are good with increasing circulating air (so it feels cooler) and getting rid of the dust and cat hair that I’m allergic to.
The big HEPA air purifier we bought has a connected app that tells us the PM2.5 levels, and our portable PM2.5 monitor confirms that it’s putting out air with a PM2.5 level of 0. Yay! This sits in our kitchen by our front door, so it helps clean the smoky hallway air coming inside.
The hallway air is TERRIBLE. The hallway opens directly to the parking garage, and is usually about as smoky as the outdoor air: it only has a single A/C duct for the whole building, which isn’t always running. The stairwell leading outside is a little cleaner than the hallway and outside. (So I’m glad we have our best air purifier situated to take on the air coming in when we open the hallway door). So we won’t be spending time exercising in the hallways, either; with that level of air quality you might as well be outside anyway, because we need to be masked either way.
The other purifier we have is a smaller purifier. I have it sitting on the counter in our bathroom, because the air exchange to outside is really reduced compared to what it should be (and the building management doesn’t seem very interested in trying to figure out how to fix it). That purifier gets PM2.5 down from 4 to 1 ug/m^3, or about a 4x improvement! Which is pretty good, although not quite as good as the big purifier in our kitchen/entry. Since it’s small enough to sit on a desk or bedside table and blow clean air at me where I’m working or sleeping, we decided to order 2 more of these smaller purifiers for my office and our bedroom, since the box fans take care of PM10 but not the PM2.5.
Since the portable air quality monitor would be hard to fit inside his mask or his mouth, and impossible to read there, Scott also held up the PM2.5/10 monitor to the exhaust valve on his n95 mask (note: not all our n95 masks our valved but the valved ones are good for wildfire smoke and managing temperature levels inside your mask when exercising) while outside, and the average PM2.5 level there is about half that of the ambient air. Since about half the time he’s breathing in (and the meter is sucking in outside air) and the other half of the time he’s breathing out (so it’s getting the mask-filtered air he inhaled and then exhaled), this suggests that the mask is doing it’s job of reducing PM2.5 levels he’s breathing inside the mask to very low levels (probably about the same as our very clean indoor air).
He also held it over the small air purifier that I’ve been keeping my face over. It, too, reduces PM2.5 down to about 2 – so not as good as the bigger purifiers, but a ~2x improvement over the ~4 in the ambient air that I would otherwise be breathing.
TLDR:
Box fans with MERV 10 filters are great for allergens and PM10, but don’t noticeably reduce the PM2.5. Higher MERV filters might do better, but are very expensive, and probably less cost-effective than a purifier with a proper HEPA filter.
Small and big air purifiers work well for reducing PM2.5.
N95 masks are effective at drastically reducing the PM2.5 you’d be exposed to outside.
If you’re like me and are bothered inside when the air quality outside is bad, additional air purifiers (small or big) might help improve your quality of life during these smoky days that we are increasingly getting every year.
In addition to the primary endpoint results from the CREATE trial, which you can read more about in detail here or as published in the New England Journal of Medicine, there was also a continuation phase study of the CREATE trial. This meant that all participants from the CREATE trial, including those who were randomized to the automated insulin delivery (AID) arm and those who were randomized to sensor-augmented insulin pump therapy (SAPT, which means just a pump and CGM, no algorithm), had the option to continue for another 24 weeks using the open source AID system.
These results were presented by Dr. Mercedes J. Burnside at #EASD2022, and I’ve summarized her presentation and the results below on behalf of the CREATE study team.
What is the “continuation phase”?
The CREATE trial was a multi-site, open-labeled, randomized, parallel-group, 24-week superiority trial evaluating the efficacy and safety of an open-source AID system using the OpenAPS algorithm in a modified version of AndroidAPS. Our study found that across children and adults, the percentage of time that the glucose level was in the target range of 3.9-10mmol/L [70-180mg/dL] was 14 percentage points higher among those who used the open-source AID system (95% confidence interval [CI], 9.2 to 18.8; P<0.001) compared to those who used sensor augmented pump therapy; a difference that corresponds to 3 hours 21 minutes more time spent in target range per day. The system did not contribute to any additional hypoglycemia. Glycemic improvements were evident within the first week and were maintained over the 24-week trial. This illustrates that all people with T1D, irrespective of their level of engagement with diabetes self-care and/or previous glycemic outcomes, stand to benefit from AID. This initial study concluded that open-source AID using the OpenAPS algorithm within a modified version of AndroidAPS, a widely used open-source AID solution, is efficacious and safe. These results were from the first 24-week phase when the two groups were randomized into SAPT and AID, accordingly.
The second 24-week phase is known as the “continuation phase” of the study.
There were 52 participants who were randomized into the SAPT group that chose to continue in the study and used AID for the 24 week continuation phase. We refer to those as the “SAPT-AID” group. There were 42 participants initially randomized into AID who continued to use AID for another 24 weeks (the AID-AID group).
One slight change to the continuation phase was that those in the SAPT-AID used a different insulin pump than the one used in the primary phase of the study (and 18/42 AID-AID participants also switched to this different pump during the continuation phase), but it was a similar Bluetooth-enabled pump that was interoperable with the AID system (app/algorithm) and CGM used in the primary outcome phase.
All 42 participants in AID-AID completed the continuation phase; 6 participants (out of 52) in the SAPT-AID group withdrew. One withdrew from infusion site issues; three with pump issues; and two who preferred SAPT.
What are the results from the continuation phase?
In the continuation phase, those in the SAPT-AID group saw a change in time in range (TIR) from 55±16% to 69±11% during the continuation phase when they used AID. In the SAPT-AID group, the percentage of participants who were able to achieve the target goals of TIR > 70% and time below range (TBR) <4% increased from 11% of participants during SAPT use to 49% during the 24 week AID use in the continuation phase. Like in the primary phase for AID-AID participants; the SAPT-AID participants saw the greatest treatment effect overnight with a TIR difference of 20.37% (95% CI, 17.68 to 23.07; p <0.001), and 9.21% during the day (95% CI, 7.44 to 10.98; p <0.001) during the continuation phase with open source AID.
Those in the AID-AID group, meaning those who continued for a second 24 week period using AID, saw similar TIR outcomes. Prior to AID use at the start of the study, TIR for that group was 61±14% and increased to 71±12% at the end of the primary outcome phase; after the next 6 months of the continuation phase, TIR was maintained at 70±12%. In this AID-AID group, the percentage of participants achieving target goals of TIR >70% and TBR <4% was 52% of participants in the first 6 months of AID use and 45% during the continuation phase. Similarly to the primary outcomes phase, in the continuation phase there was also no treatment effect by age interaction (p=0.39).
The TIR outcomes between both groups (SAPT-AID and AID-AID) were very similar after each group had used AID for 24 weeks (SAPT-AID group using AID for 24 weeks during the continuation phase and AID-AID using AID for 24 weeks during the initial RCT phase).. The adjusted difference in TIR between these groups was 1% (95% CI, -4 to 6; p=-0.67). There were no glycemic outcome differences between those using the two different study pumps (n=69, which was the SAPT-AID user group and 18 AID-AID participants who switched for continuation; and n=25, from the AID-AID group who elected to continue on the pump they used in the primary outcomes phase).
In the initial primary results (first 24 weeks of trial comparing the AID group to the SAPT group), there was a 14 percentage point difference between the groups. In the continuation phase, all used AID and the adjusted mean difference in TIR between AID and the initial SAPT results was a similar 12.10 percentage points (95% CI, p<0.001, SD 8.40).
Similar to the primary phase, there was no DKA or severe hypoglycemia. Long-term use (over 48 weeks, representing 69 person-years) did not detect any rare severe adverse events.
Conclusion of the continuation study from the CREATE trial
In conclusion, the continuation study from the CREATE trial found that open-source AID using the OpenAPS algorithm within a modified version of AndroidAPS is efficacious and safe with various hardware (pumps), and demonstrates sustained glycaemic improvements without additional safety concerns.
Key points to takeaway:
Over 48 weeks total of the study (6 months or 24 weeks in the primary phase; 6 months/24 weeks in the continuation phase), there were 64 person-years of use of open source AID in the study, compared to 59 person-years of use of sensor-augmented pump therapy.
A variety of pump hardware options were used in the primary phase of the study among the SAPT group, due to hardware (pump) availability limitations. Different pumps were also used in the SAPT-AID group during the AID continuation phase, compared to the pumps available in the AID-AID group throughout both phases of trial. (Also, 18/42 of AID-AID participants chose to switch to the other pump type during the continuation phase).
The similar TIR results (14 percentage points difference in primary and 12 percentage points difference in continuation phase between AID and SAPT groups) shows durability of the open source AID and algorithm used, regardless of pump hardware.
The SAPT-AID group achieved similar TIR results at the end of their first 6 months of use of AID when compared to the AID-AID group at both their initial 6 months use and their total 12 months/48 weeks of use at the end of the continuation phase.
The safety data showed no DKA or severe hypoglycemia in either the primary phase or the continuation phases.
Glycemic improvements from this version of open source AID (the OpenAPS algorithm in a modified version of AndroidAPS) are not only immediate but also sustained, and do not increase safety concerns.

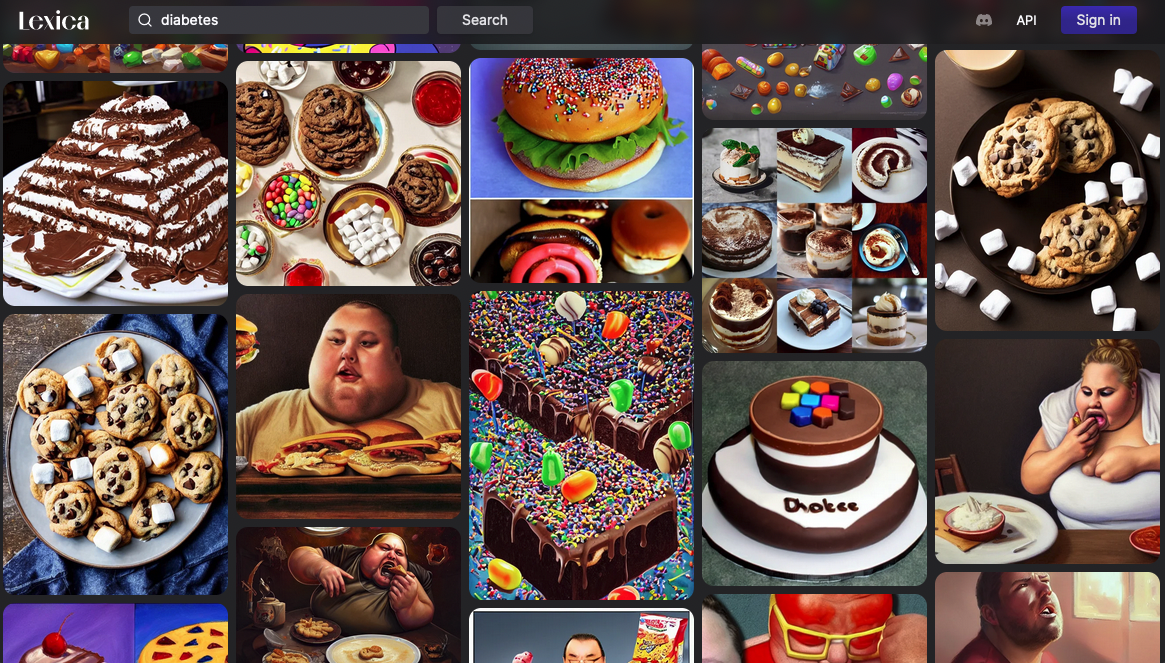
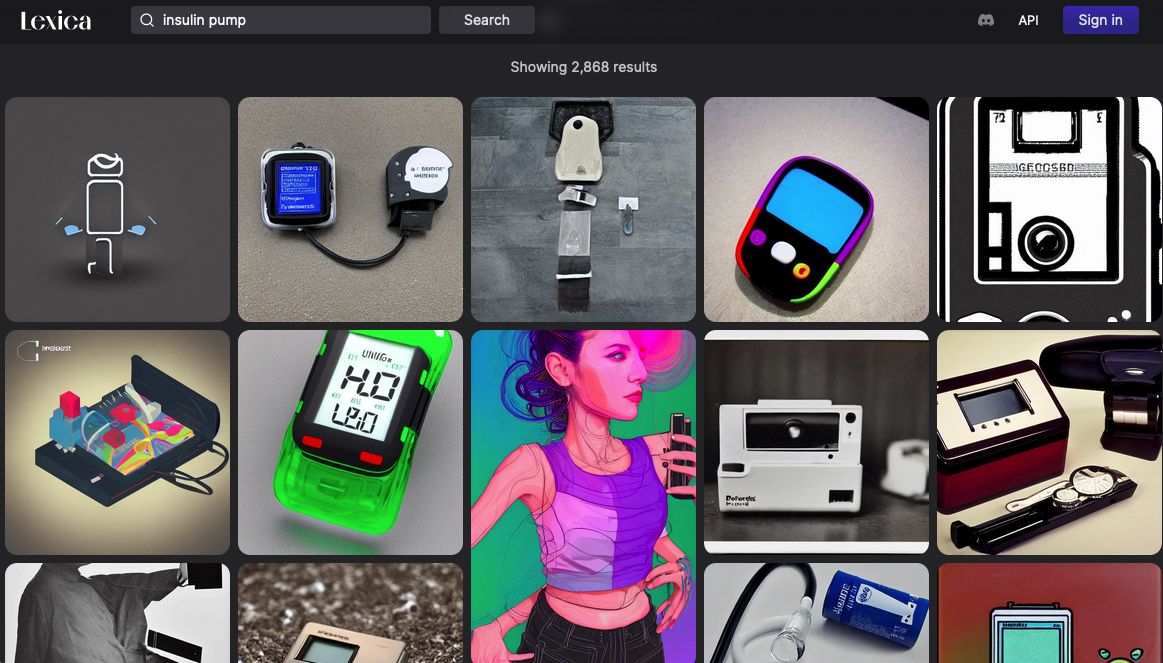

 I went slow the first lap (part of why I was feeling so strong), and I took my time in between laps. I pulled off my socks and shoes. I used hand sanitizer on them to draw some of the water out, then re-lubricated and added Desitin (to continue to help draw water out of my feet and aid in preventing blisters). Then I put on a fresh pair of toe socks and added more lamb’s wool in between key toes that typically are blister-prone. At this stage I had no blisters, and other than wet soggy feet was in good shape! Sitting for 10 minutes for my sock and foot care change chilled me, though, and I was happy to start moving again and warm back up.
I went slow the first lap (part of why I was feeling so strong), and I took my time in between laps. I pulled off my socks and shoes. I used hand sanitizer on them to draw some of the water out, then re-lubricated and added Desitin (to continue to help draw water out of my feet and aid in preventing blisters). Then I put on a fresh pair of toe socks and added more lamb’s wool in between key toes that typically are blister-prone. At this stage I had no blisters, and other than wet soggy feet was in good shape! Sitting for 10 minutes for my sock and foot care change chilled me, though, and I was happy to start moving again and warm back up.

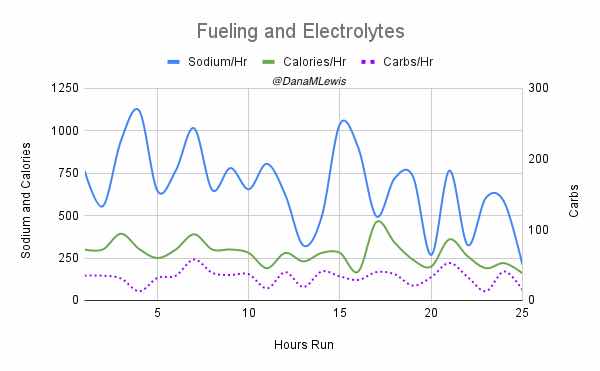
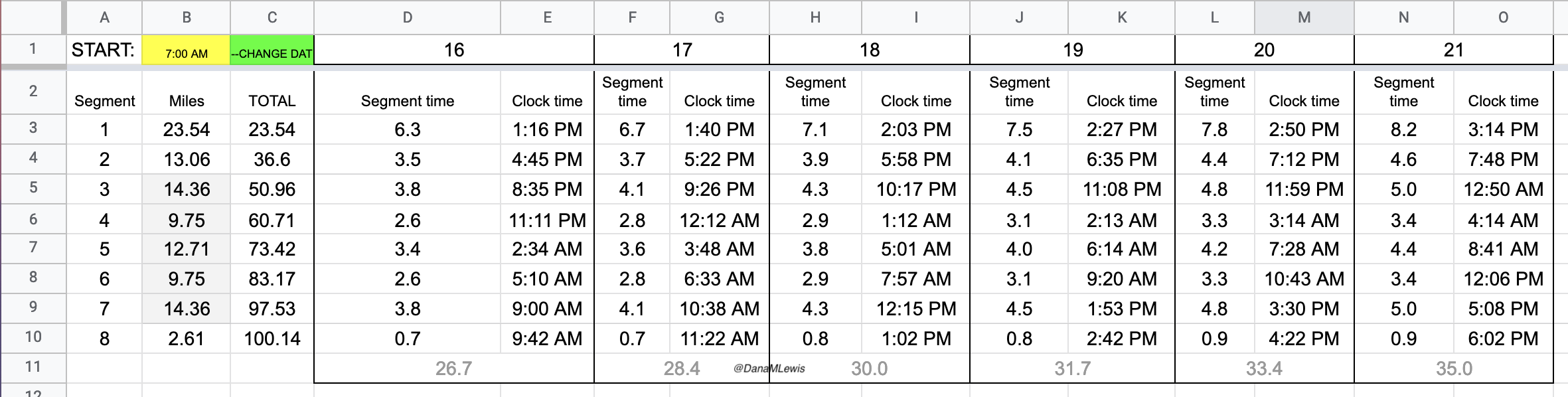
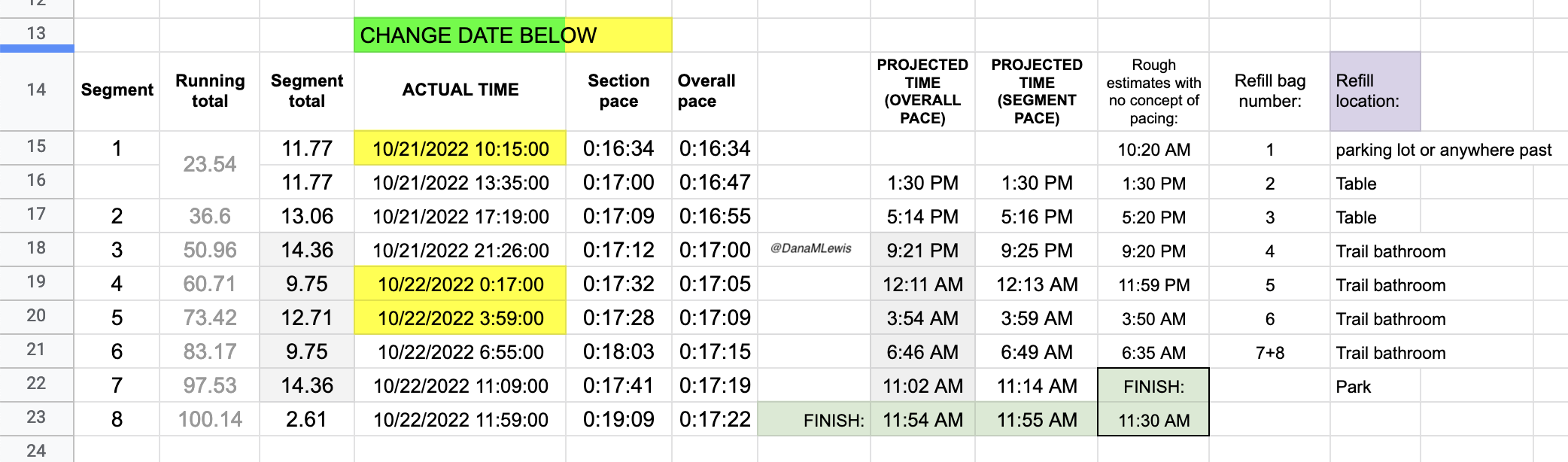
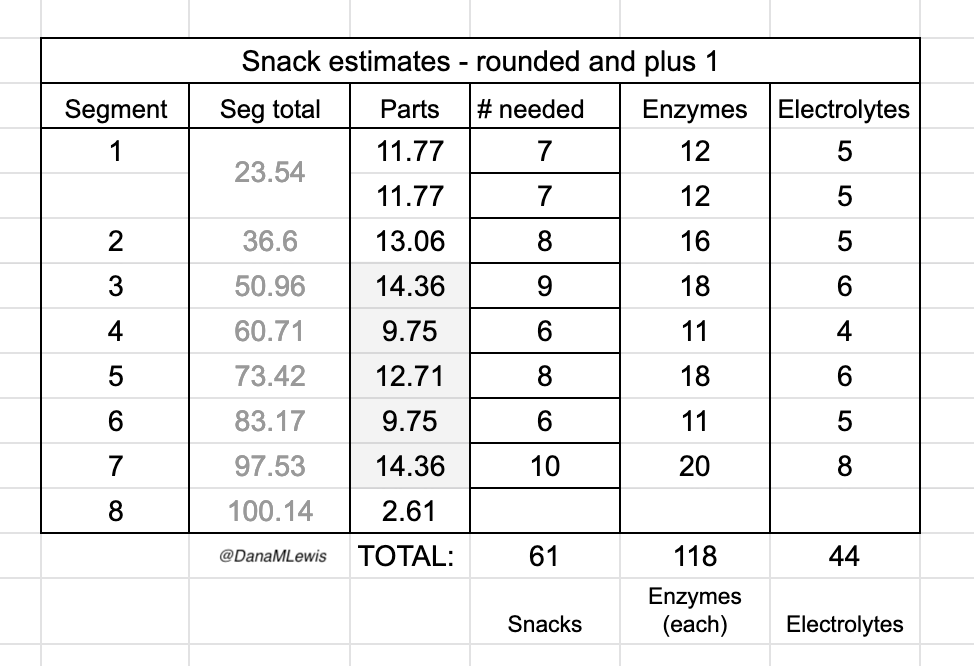
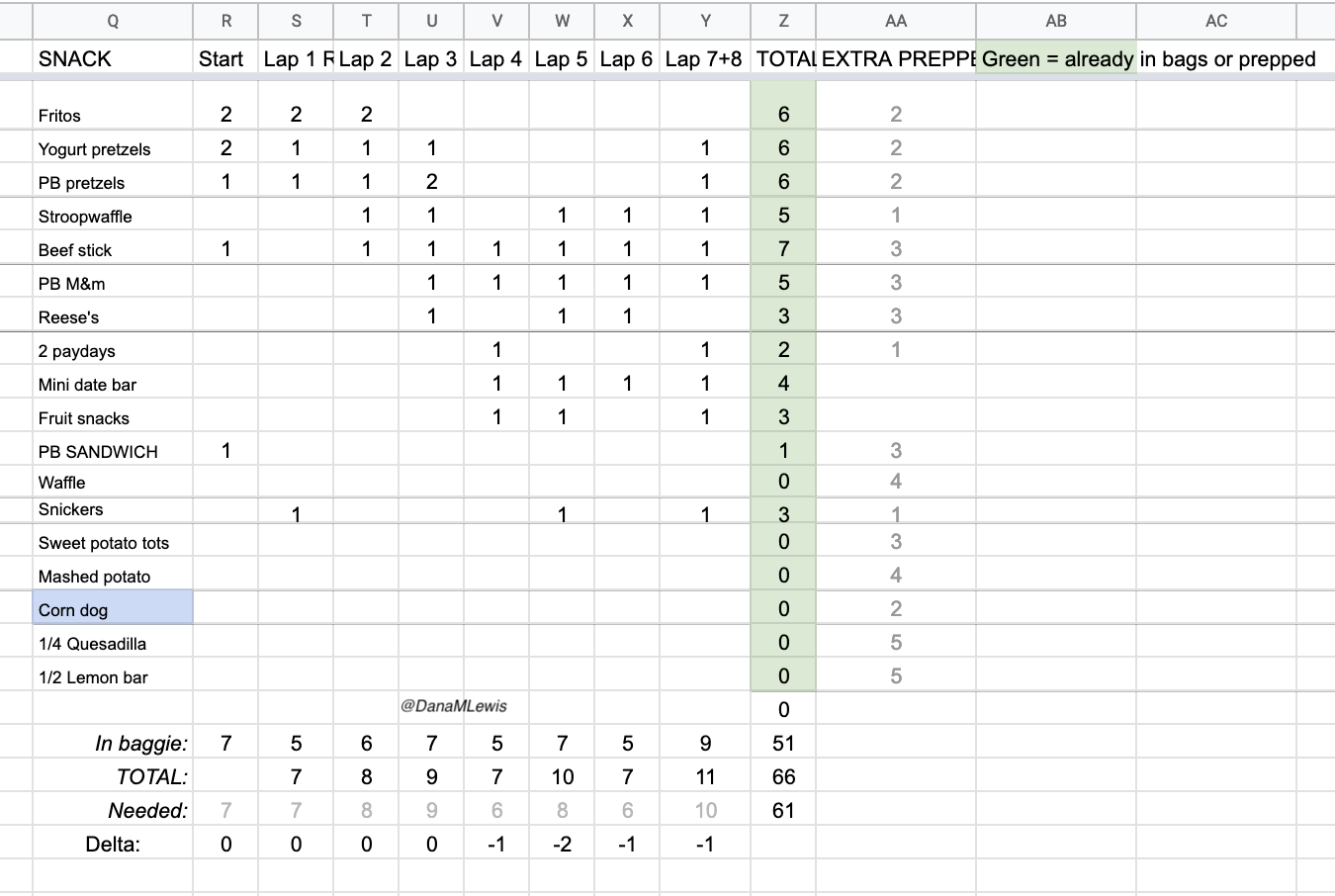


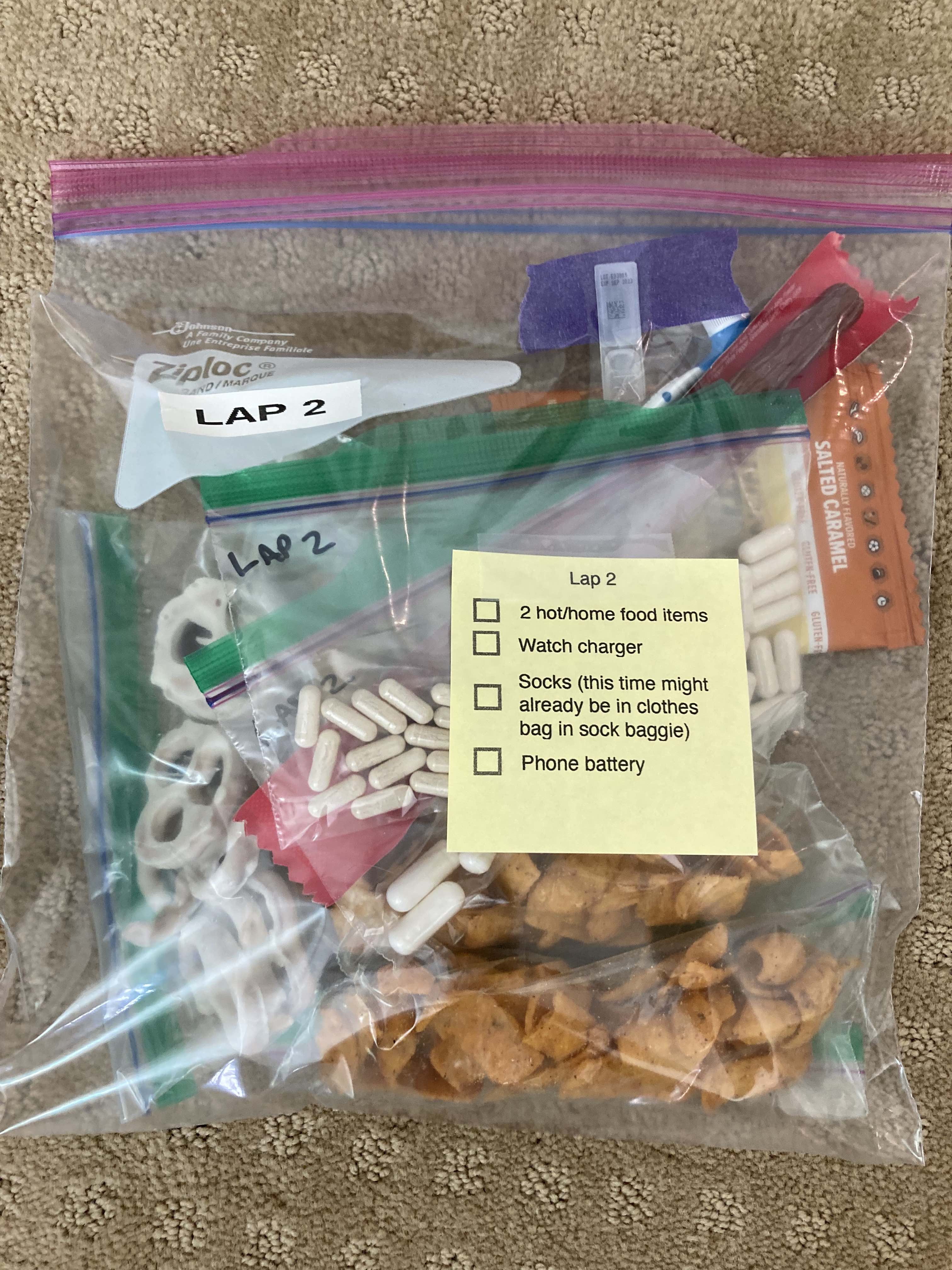
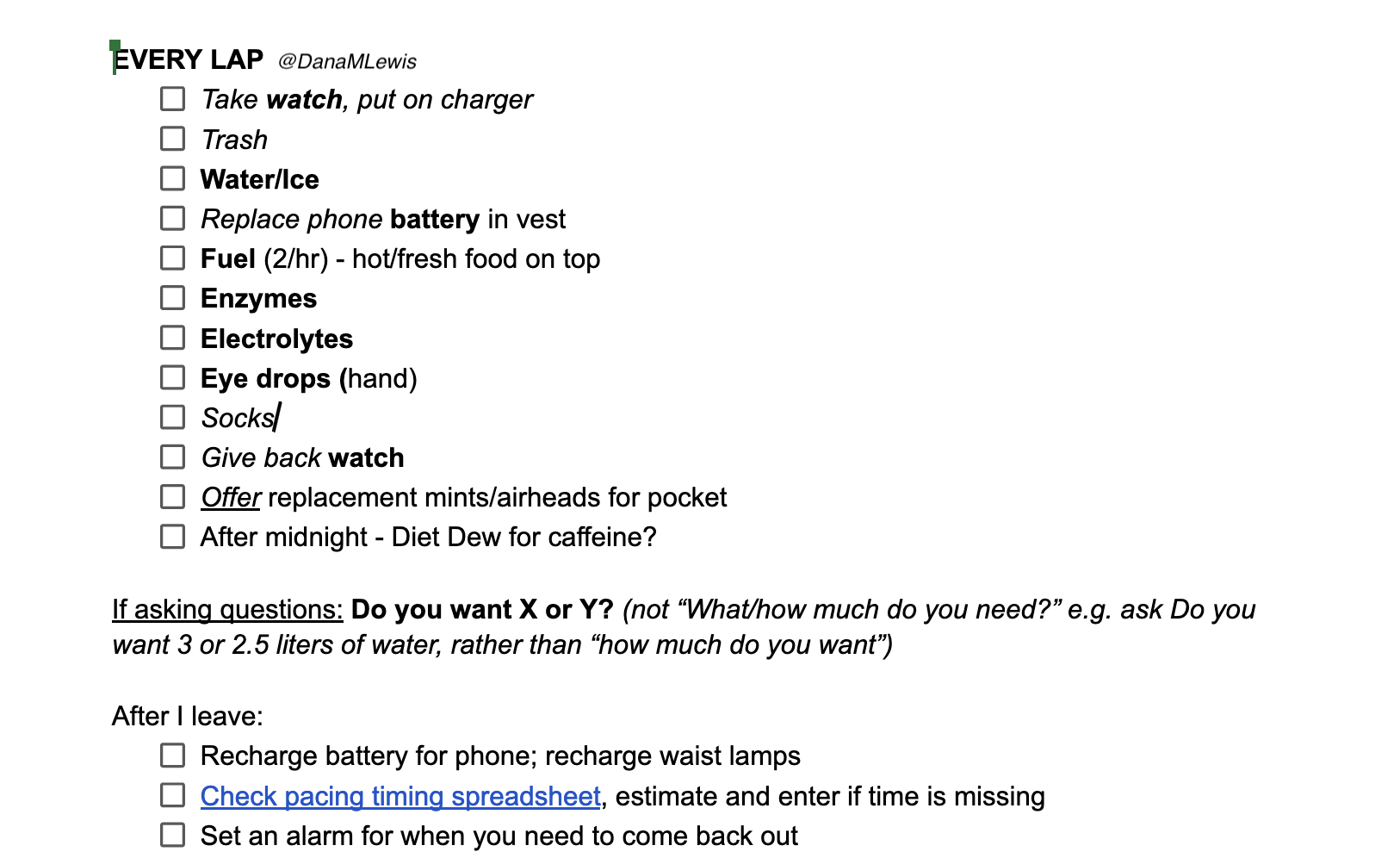
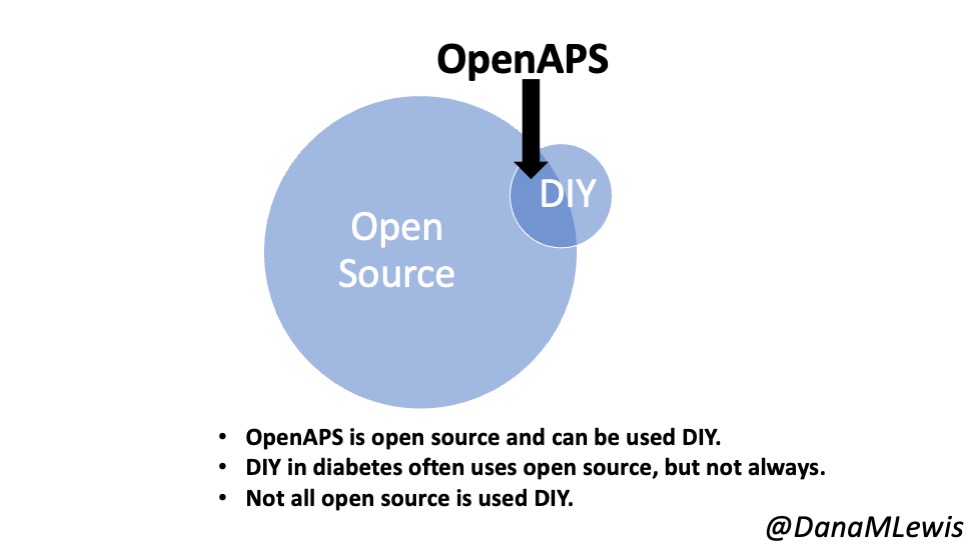


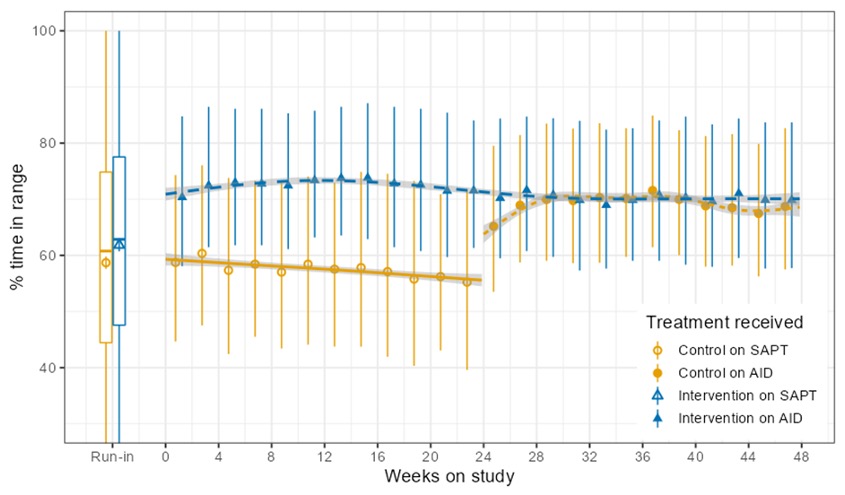
Recent Comments