I’ve now run two ultramarathons (both happened to be 50k races, with a race report for the second race here), and was planning my third ultrarace. I had my eye on the 50 mile (50M) version of the 50k I ran last year. It’s on a course I adore – a 6 foot wide crushed gravel trail that’s slightly uphill (about 1,000 feet) for the first 30 miles and then downhill at 2% grade for the remaining 20 miles. It happens to be close to home (hour and a half drive to the start), which helps for logistics.
I started training for the 50M weeks after my 50k this year, including talking my husband into taking me out to run some of the segments along the first 25 miles of the course. I’ve done the back half of the course several times through training and racing the 50k, and I wanted to check out each of the earlier segments to get a sense of what trail bathrooms existed on the course, make notes about milestones to watch for at various distances, etc.
After the first training run out there, when I started talking goal paces to get through the first and main cutoff at mile 30 (cutoffs got progressively easier from there, and even walking very slowly you could finish if you wanted to), my husband started to suggest that I should just run the course some other time on my own, so I didn’t have to worry about the cutoffs. I told him I didn’t want to do that. The cutoffs are a good incentive to help me push myself, and it’s worth the stress it causes in order to try to perform my best. (My target pace would get me through a comfortable 15 minutes before cutoff, and I could dial up the effort if needed to achieve cutoff). However, he suggested it another time and pointed out that even when running an organized race, I tend to run self-supported, so I don’t really don’t benefit as much from running in a race. I protested and talked again about the camaraderie of running when everyone else did, the fact that there were aid stations, the excellent search and rescue support, the t-shirt, the medal, the pictures! Then out loud I realized that I would be running at the back of the pack that I would miss the pictures at 25 miles because the photographer heads to the finish before I would get there. And they stop finish line pictures 3 hours before the end of the race. (Why, I don’t know!) And so I’d miss those photos too. And last year, I didn’t partake in the 50k staffed aid stations because I couldn’t eat any of their food and didn’t want any extra COVID exposure. Instead, my husband crewed me and refilled my hydration at two points on the course. The un-staffed aid stations didn’t have the plethora of supplies promised, and one race report from someone near the front of the pack said they were low on water! So it was a good thing I didn’t rely on the aid stations. I didn’t wear the tshirt last year, because it wasn’t a tech tee. Medals aren’t that exciting. So…why was I running the organized race?
My only remaining reasons were good search and rescue (still true) and the motivation of signing up for and committing to running on that date. It’s a commitment device. And my husband then smashed that reason, too, by reminding me that the only commitment device I typically need is a spreadsheet. If I decide I’m going to work toward a goal, I do. Signing up doesn’t make a difference.
And to be fair, he crews me whether it’s an organized race or not! So to him, it makes no difference whether I’m running an organized race or a self-organized long ultra.
And so I decided to give it some thought. Where would I run, if I could run anywhere in an hour’s distance from home? Do the same 50 mile course? Was that course worth it? Or was there somewhere closer to home where I could run that would be easier for my husband to crew?
He suggested running on our “home” trails, which is a network of hundreds of miles of paved trail that’s a short walk away. I immediately scoffed, then took the suggestion seriously. If I ran “from home”, he could crew from home and either drive out or e-bike out or walk out to bring me supplies along my route. If the park trail bathrooms ended up getting locked, I could always use the bathroom at home (although not ideal in terms of motivating myself to move quickly and get back out on the trail). I’d have a bigger variety of fueling options, since he could microwave and bring me out more options than if it had to be shelf-stable.
The list of benefits of potentially doing my own DIY or self-organized ultra grew.
(And then, I broke my toe. Argh. This further solidified my willingness to do a DIY ultra, because I could train up until when I was ready, and then run my distance, without having to choose between a non-refundable signup and not running or risking injury from running before I was ready.)
Eventually, my plans evolved (in part due to my broken toe). I was originally going to DIY a 50M or 100k (62M) over Labor Day weekend, recover, then re-train up and run a DIY 100 mile (100M) in late October or early November. When I broke my toe, I decided to scratch the “test” 50M/100k and just train and run the 100M, since that was my ultimate goal distance for the year.
Here are the pros of running a DIY ultra or a “self-organized” ultra, rather than an organized race with other people:
- For me specifically, I have better trail options and route options. I can run a 95% flat course on paved, wide, safe trails through my local community.
- These are so local that they are only a few minutes walk from my door.
- The location means it’s easy for Scott to reach me at any point. He can walk out and bring me water and fuel and any needed supplies when I complete a loop every 4 or so hours. If needed, he could also e-bike out to bring me anything I need if I ran out or had a more urgent need for supplies. He can also drive out and access the course every half mile or mile for most of my planned route.
This also means I have more fuel options that I can prepare and have for Scott to bring out. This is awesome because I can have him warm up ¼ of a ham and cheese quesadilla, or a corn dog, or sweet potato tots, or any other fuel options that I wouldn’t be able to use if I had to rely on pre-packed shelf stable options for a 30 hour race.
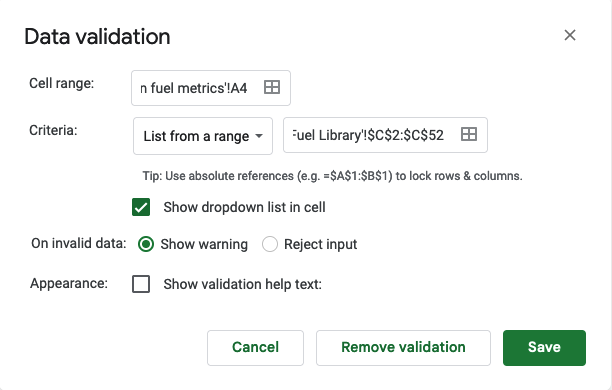
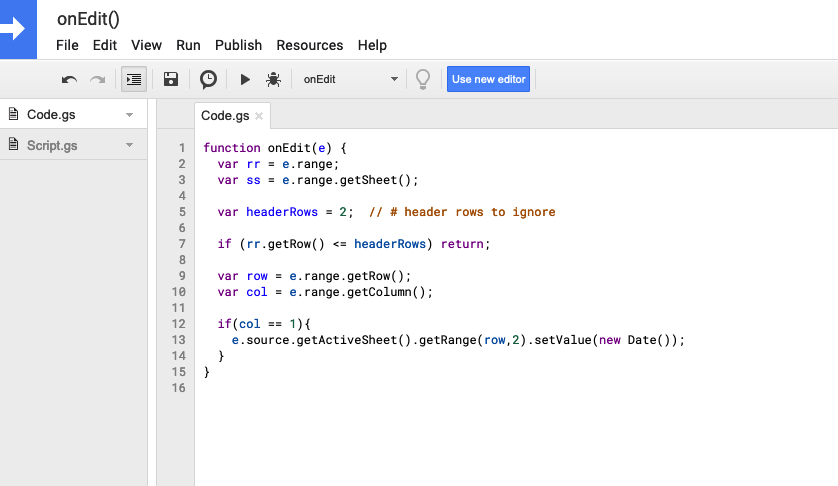
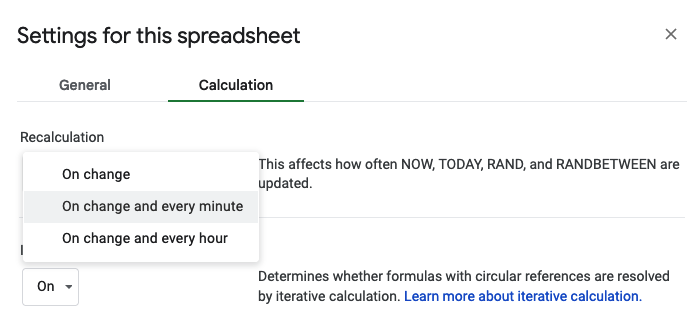
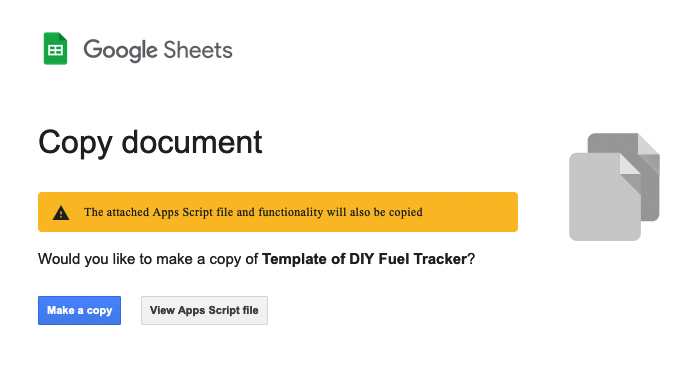
(Note that even if I did an organized race, I most likely still wouldn’t benefit from aid station food. In part, because I have celiac and have to have everything gluten free. I also have to watch cross contamination, so a bowl of any kind of food that’s not individually packaged is something that’s likely contaminated by gluten. COVID has helped reduce this but not completely. Plus, I have diabetes so I need to be roughly aware of the amount of carbs I’m eating to decide whether or not to dose insulin for them, given what is happening to my blood sugar at the time. And, I have exocrine pancreatic insufficiency (EPI) which means I have to dose enzymes for everything I eat. Grazing is hard with EPI; it’s easier to dose and eat the amount that matches my enzymes, so pre-packaged snacks that I know the carb and fat and protein count means I know what insulin I need and what enzymes I need for each set of “fuel”. Guessing carb counts or enzyme counts in the middle of the night while running long distance is likely not going to be very effective or fun. So as a result of all that – pre-planned food is the way to go for me. Related, you can read about my approach for tracking fuel on the go with a spreadsheet and pre-planned fuel library here.)
- There is regular public bathroom access along my chosen route.
- I’ve designed out and back laps and loops that have me coming back by my start (remember, only a few minutes walk from home) and that make it so I am passing the bathrooms multiple times on a regular basis in case I need them.
These laps and loops also make for mentally smaller chunks to tackle. Instead of 100 miles, I’ve got a ~24 mile out and back, a 13 mile loop, a 16 mile out and back, a repeat of the 13 mile loop, repeating again the 16 mile out and back followed by the 13 mile loop one more time, and then a quick 5 mile total out and back (so 2.5 out and back). These are also all routes I know well, so mentally finding waypoints to focus on and know how far I’ve gone are a huge benefit for mentally breaking down the distance into something my brain and body “know”.
- There are no cutoffs or pace requirements. If I slow down to a 20 minute mile (or slower)…well hey, it’s faster than I was walking with my hands-free knee crutch a few months ago! (I rocked anywhere from a 45 minute mile to a 25 minute mile).
There’s no pressure to go faster, which means I won’t have pressure to push my effort, especially at the start. Hopefully, that means I can maintain an “easy”, even effort throughout and maybe cause less stress to my body’s hormone systems than I would otherwise.
The only pressure I have will be the pressure I put on myself to finish (eventually), which could be 26 hours or could be 30 hours or could be 36 hours or even slower… basically I have to finish before my husband gives up on coming out to refuel me!
- And, once I finish, it’ll be ‘fast’ to get home, shower, refuel, and be done. This is in comparison to a race where I’d have an hour+ drive to get home. I’ll need to walk home which might actually take me much longer than that after I’ve ambulated for 100 miles…but it should hopefully be shorter than an hour!
- Finally, the major benefit is flexibility. I can set my race date for a weekend when I’ve trained enough to do it. I can move it around a week or two based on the weather (if it’s too cold or too rainy). I can even decide to move it to the spring (although I’d really love to do it this year).
Here are some of the cons of running a DIY ultra or a “self-organized” ultra, rather than an organized race with other people:
- Theoretically, it would be easier to stop because I am so close to home. I haven’t committed money or drive time or dragged my husband to far away places to wait for me to finish my run. (However, I’m pretty stubborn so in my case I think this is less of an issue than it might be for others?)
- Yet, out and back loops and the route I’ve chosen could get monotonous. I chose these loops and the route because I know the distance and almost every tenth mile of the route super well. The first 6 miles of all the laps/loops are the same, so I’ll run those same 6 miles repeated 7 times over the course of the run.
- I won’t have the camaraderie and knowledge that other people are out here tackling the same distance. I’m a back of the pack runner (and celebrate being places from last the way most people celebrate places from first!) and often don’t see anyone running after the start…yet there’s comfort in knowing I’m one of dozens or hundreds out here covering the same course on the same day with the same goal. I do think I’ll miss this part.
- There is no one to cheer for me. There’s no aid station volunteers, fellow runners, or anyone (other than my amazing husband who will crew me) to cheer for me and encourage me and tell me I’m moving well.
- There’s no medal (not a big deal), t-shirt (not a big deal), or official finishing time (also not a big deal for me).
- There’s no cutoffs or pace requirements to motivate me to keep pushing when things get hard.
All in all, the benefits pretty clearly outweigh the downsides – for me. Again, I’m a back of the pack super slow runner (in fact, I typically run 30 seconds and walk 60 seconds throughout my whole race consistently) who can’t eat aid station food (because celiac/EPI makes it complicated) coming off of a broken toe injury (which messed up my training and racing plans), so my pros/cons lean pretty heavily toward making a DIY/self-organized solo ultra run an obvious choice. Others might have different pro/con list based on the above variables and their situations, but hopefully this helps someone else think through some of the ways they might decide between organized and un-organized ultramarathon efforts!




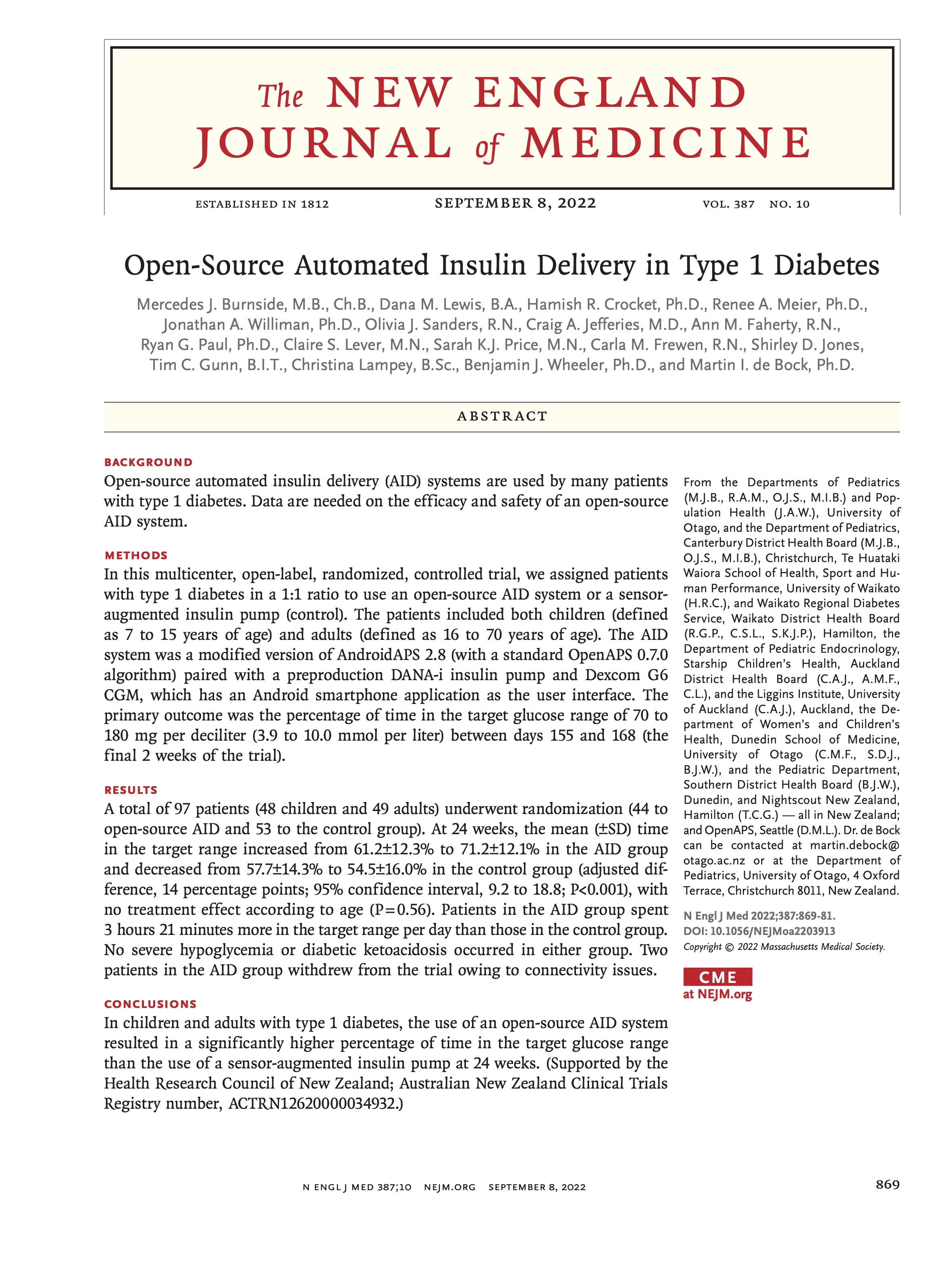 I’m thrilled to share that the results of the first RCT on open source automated insulin delivery (AID) is now published in a peer-reviewed medical journal (New England Journal of Medicine, known as NEJM). You can find it at NEJM
I’m thrilled to share that the results of the first RCT on open source automated insulin delivery (AID) is now published in a peer-reviewed medical journal (New England Journal of Medicine, known as NEJM). You can find it at NEJM 


Recent Comments