If you’re someone who is considering an IUD (intrauterine device) or has an IUD and is considering a replacement or the removal process, this post is for you. You should know about this! Feel free to share it with a friend.
I recently decided to replace my IUD. I was dreading it, because I found the insertion process the first time I got one to be the most painful thing I had ever experienced. For context, years later I massively broke my ankle in 3 places. I now am able to articulate that the pain level of an IUD insertion, for me, is like broken bone level pain inside. It “only” lasts for a few minutes at that level, but nevertheless, it is excruciating.
When I was due for my first ever replacement (swap), I asked my doctor’s office if there were any better pain management options than what I experienced for the insertion process. They told me no, the only thing they could offer was an oral medication I could try to soften the cervix. I took it in advance as directed, and also took full doses of ibuprofen and Tylenol, went for the swap process and…it was just as bad as the first insertion, even though I had previously had one. Ugh.
The good news related to IUDs is that they keep getting extended, in terms of how many years they are approved for birth control efficacy. Mine went from 5 years approval to 8 years approval, so I was looking forward to having more years in between the terrible experiences. However, my experience was that this time around when I reached a little over 5 years (fully expecting to go to 8 years with it), my period bleeding picked back up to a degree that I decided I would go ahead and swap to a new one. (Birth control-wise, they’re approved for 8 years, but the approval indication for heavy bleeding is still at 5 years, so it makes sense that some people who see a reduction in period bleeding on IUDs may see a return after that 5 year timeframe. Not everyone, but some will, and I did.)
So that’s why I was going in to get a replacement, at about 5.5 years from my last one. This time, I had a new provider’s office, but since my last office couldn’t offer me any reasonable pain mitigation, I didn’t bother asking in advance and just went in with an active dose of Tylenol in my system, mentally prepared for the pain.
But then, at my appointment when going over the risks and discussing any questions I had before the procedure, my new provider said “what pain mitigation would you like?”
I said: “What? You’re offering me something?!”
And yes, there are options and she did offer them! She talked about ibuprofen/Tylenol (I already had taken Tylenol), a hot pack for the stomach, or something called a paracervical block. It’s an injection, so she asked how I felt about needles. I laughed and told her I had type 1 diabetes (the implication being, I deal a lot with needles and regardless of what I feel about them, they keep me alive so I am used to dealing with them).
The side effects of this paracervical block include potentially experiencing ringing in the ears and a metal taste in your mouth, plus obviously the potential pain from the injection itself.
I quickly evaluated my thoughts – I didn’t think it would help (because softening the cervix previously didn’t help), and I didn’t love the idea of a block. That’s because my previous ‘nerve block’ type injections, such as when at the dentist, result in a LOT of pain for me for the injection. But, then again, the IUD replacement process is even more painful, so I thought for the small chance that it would help cut down on that pain, it was worth trying at least once. So I said yes.
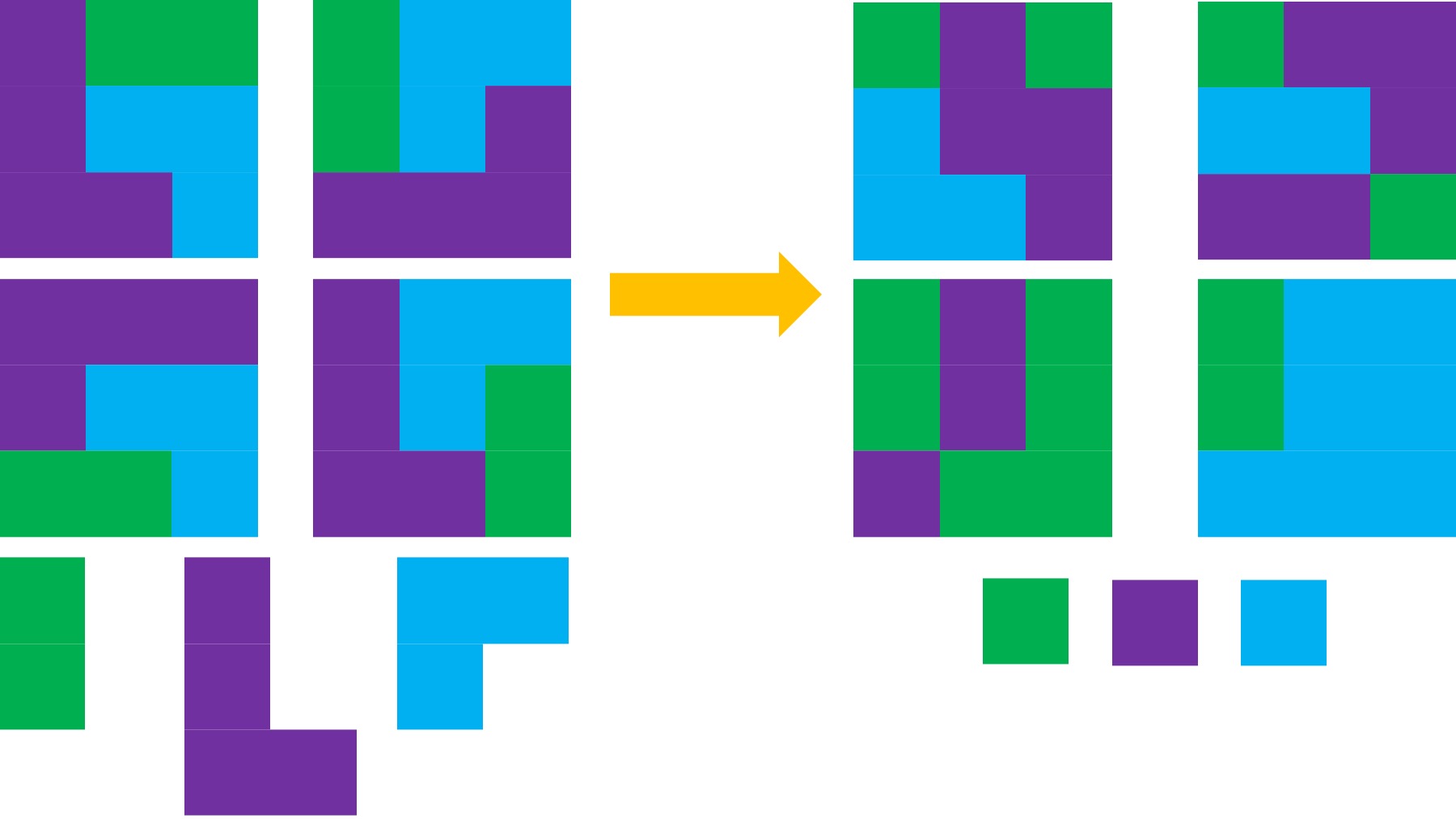
While she was getting set up, I asked her if this was new (because I was surprised I hadn’t heard of it) and she said no, it’s been around but early research showed it wasn’t much more effective than placebo so it didn’t really pick up in clinical practice, but that later studies DID show efficacy of it. (I later looked that up and she was right – there’s a 2012 study showing similar efficacy on pain reduction to placebo, aka around 30%); whereas international studies and a later 2018 study with an increased dose DID show pain reduction for more people.) And we all know it takes time for things to translate to clinical practice (see this visual and imagine it as a game of telephone), so knowing this now helps me better understand why in 2015 (my first insertion) and 2020 (my first replacement), this was not an option offered to me by my old clinic. I don’t like it, but I understand the context better.
What the experience of a paracervical block was like
The first step was a numbing spray. Then came the injection. Maybe because of the numbing spray, it didn’t feel like an injection the way I normally experience injections for nerve blocks. I felt a minor pinch and a little bit of pressure from the fluid going in. I was surprised that it took a few (it was injected into several areas) and I was borderline slightly uncomfortable, not in the sense that I was going to ask her to stop, but I was ready for that part to be done. (And probably anticipatory pain for the actual removal/swap process). But it was done and then I realized, this was nothing like the other injections for nerve blocks and it was indeed very tolerable.
(Side effect wise, I did not experience ‘ringing’ in my ears, but I did feel like I could hear more easily (e.g. sounds in the room suddenly got louder). Afterward when I got up, I did feel a little odd for about 60 seconds, but that could have also been because I was laying down and then hopped back up (see below) pretty soon after. I didn’t have any taste in my mouth, and the ‘louder sounds’ didn’t persist beyond a few minutes. None of the side effects phased me nor would influence my decision to get another one.)
Then it was time for the IUD removal. She asked me to cough and I did while it came out. It felt uncomfortable like a pinch with friction, but it wasn’t stabbing excruciating pain. It wasn’t “sharp” feeling like pain. I breathed a bit while she got ready to do the insertion of the new IUD and she asked me to take a few deep breaths. I did, and the IUD was inserted. Like the removal, it felt slightly uncomfortable, but again more like friction, and it was less than the removal.
No excruciating, stabbing pain!!!
She was done, and I immediately sat up and told her the paracervical block helped, I was so glad I had done it, and now I wasn’t going to dread my next swap.
Previously, for my first insertion and my subsequent first swap, it took me a minute or two of laying there, breathing deeply, to recover from the intense, excruciating pain. I would be able to get up and get dressed and leave on my own, but it definitely was an intense full body experience that required a few minutes and then I would feel like I had to recover from it (psychologically) the rest of the day. And obviously carry that experience 5 years forward.
In contrast, I immediately sat up and was ready to get dressed and go. I didn’t need to recover. I left and drove home in great spirits, then started texting everyone I know who had IUDs that it was a jaw-dropping, wildly different experience and they should look up paracervical blocks and when it’s time for swap/replacement IUDs, ask in advance if their doctor/clinic offers it and shop around for somewhere that will offer it if not. It is THAT wildly different of an experience. I hate making phone calls, but I will 100% make as many phone calls as it takes in the future to make sure I always have this option. It took the painful experience from broken bone level pain (e.g. 9-10/10 excruciating pain) to a tolerable discomfort with only a little bit of pain (e.g. 2-3/10 experience). I say that as someone who was told by an ER doc while he was setting my ankle, broken in 3 places, that I have a high pain tolerance.
The other benefit of the paracervical block is she said it helps reduce cramping for up to an hour. And it did! I made it home before I started to feel cramping (like strong period cramps), almost exactly an hour after the injection. I continued to alternate between Tylenol and ibuprofen the rest of the day, but this was like managing a period, and I didn’t have any pain hangover from the injection or the IUD replacement process. (Again, previously it felt like it took me hours to recover from the experience, when I had it without the paracervical block).
 Not everyone finds IUD insertions or replacement to be excruciating. If you don’t, I’m so glad for you. But my experience was that it’s the most painful thing I’ve ever experienced. Over half the people I talk to with personal experience also say it is incredibly painful. So if you are one of the people, like me, who find IUD insertions or IUD replacements to be a terrible, painful experience…ask about a paracervical block. It makes an incredible difference and I’m now not dreading the replacement or future removal.
Not everyone finds IUD insertions or replacement to be excruciating. If you don’t, I’m so glad for you. But my experience was that it’s the most painful thing I’ve ever experienced. Over half the people I talk to with personal experience also say it is incredibly painful. So if you are one of the people, like me, who find IUD insertions or IUD replacements to be a terrible, painful experience…ask about a paracervical block. It makes an incredible difference and I’m now not dreading the replacement or future removal.
(And if you have any other questions about the experience that I can answer, happy to do so – leave a comment below.)
 These are actionable, doable, practical things we can all be doing, today, and not just gnashing our teeth. The sooner we course correct with improved data availability, the better off we’ll all be in the future, whether that’s tomorrow with better clinical care or in years with AI-facilitated diagnoses, treatments, and cures.
These are actionable, doable, practical things we can all be doing, today, and not just gnashing our teeth. The sooner we course correct with improved data availability, the better off we’ll all be in the future, whether that’s tomorrow with better clinical care or in years with AI-facilitated diagnoses, treatments, and cures. 
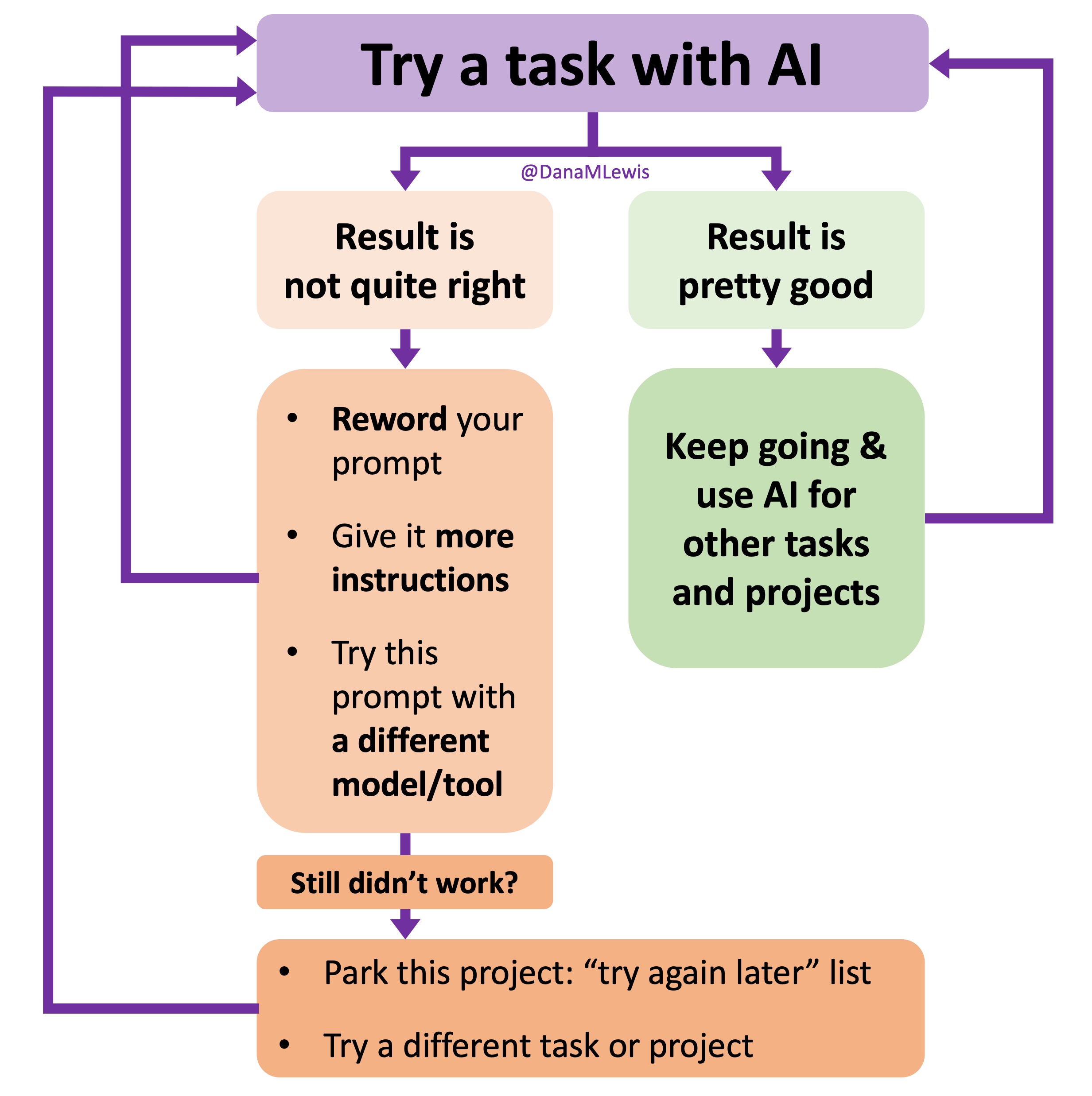 I’ve started making a list of projects or tasks I want to work on where the AI isn’t quite there yet and/or I haven’t figured out a good setup, the right tool, etc. A good example of this was
I’ve started making a list of projects or tasks I want to work on where the AI isn’t quite there yet and/or I haven’t figured out a good setup, the right tool, etc. A good example of this was  TL;DR: as more and more people are going to vibe code their way to having Android and/or iOS apps, it’s very feasible for people with less experience to do both and to distribute apps on both platforms (iOS App Store and Google Play Store for Android). However, there’s an up front higher cost to iOS ($99/year) but a slightly easier, more intuitive experience for deploying your apps and getting them reviewed and approved. Conversely, Android development, despite its lower entry cost ($25 once), involves navigating a more complicated development environment, less intuitive deployment processes, and opaque requirements for app approval. You pay with your time, but if you plan to eventually build multiple apps, once you figure it out you can repeat the process more easily. Both are viable paths for app distribution if you’re building iOS and Android apps in the LLM-era of assisted coding, but don’t be surprised if you hit bumps in the road for deploying for testing or production.
TL;DR: as more and more people are going to vibe code their way to having Android and/or iOS apps, it’s very feasible for people with less experience to do both and to distribute apps on both platforms (iOS App Store and Google Play Store for Android). However, there’s an up front higher cost to iOS ($99/year) but a slightly easier, more intuitive experience for deploying your apps and getting them reviewed and approved. Conversely, Android development, despite its lower entry cost ($25 once), involves navigating a more complicated development environment, less intuitive deployment processes, and opaque requirements for app approval. You pay with your time, but if you plan to eventually build multiple apps, once you figure it out you can repeat the process more easily. Both are viable paths for app distribution if you’re building iOS and Android apps in the LLM-era of assisted coding, but don’t be surprised if you hit bumps in the road for deploying for testing or production. As things change in my body (I have several autoimmune diseases and have gained more over the years), my ‘budget’ on any given day has changed, and so have my priorities. During times when I feel like I’m struggling to get everything done that I want to prioritize, it sometimes feels like I don’t have enough energy to do it all, compared to other times when I’ve had sufficient energy to do the same amount of daily activities, and with extra energy left over. (
As things change in my body (I have several autoimmune diseases and have gained more over the years), my ‘budget’ on any given day has changed, and so have my priorities. During times when I feel like I’m struggling to get everything done that I want to prioritize, it sometimes feels like I don’t have enough energy to do it all, compared to other times when I’ve had sufficient energy to do the same amount of daily activities, and with extra energy left over. (

 It’s important to remember that even if the total amount of time is “a lot”, it doesn’t have to be done all at once. Historically, a lot of us might work 8 hour days (or longer days). For those of us with desk jobs, we sometimes have options to split this up. For example, working a few hours and then taking a lunch break, or going for a walk / hitting the gym, then returning to work. Instead of a static 9-5, it may look like 8-11:30, 1:30-4:30, 8-9:30.
It’s important to remember that even if the total amount of time is “a lot”, it doesn’t have to be done all at once. Historically, a lot of us might work 8 hour days (or longer days). For those of us with desk jobs, we sometimes have options to split this up. For example, working a few hours and then taking a lunch break, or going for a walk / hitting the gym, then returning to work. Instead of a static 9-5, it may look like 8-11:30, 1:30-4:30, 8-9:30.
 And: patients should not be punished for asking questions in order to better understand or check their understanding.
And: patients should not be punished for asking questions in order to better understand or check their understanding.  I’ve learned from experience that waiting rarely creates better outcomes. It only delays impact.
I’ve learned from experience that waiting rarely creates better outcomes. It only delays impact. (Thank you).
(Thank you). I encourage you to think about scaling yourself and identifying a task or series of tasks where you can get in the habit of leveraging these tools to do so. Like most things, the first time or two might take a little more time. But once you figure out what tasks or projects are suited for this, the time savings escalate. Just like learning how to use any new software, tool, or approach. A little bit of invested time up front will likely save you a lot of time in the future.
I encourage you to think about scaling yourself and identifying a task or series of tasks where you can get in the habit of leveraging these tools to do so. Like most things, the first time or two might take a little more time. But once you figure out what tasks or projects are suited for this, the time savings escalate. Just like learning how to use any new software, tool, or approach. A little bit of invested time up front will likely save you a lot of time in the future.
Recent Comments