I thought I would share some of how I am using AI. Previously I’ve talked a lot about broad concepts of prompting LLMs and the types of projects that can be done. I’ve provided particular examples that I’ve found useful for n=1 custom software (to address software-shaped feelings, often) or for improving n=1*many software like my apps PERT Pilot (iOS | Android), Carb Pilot, etc. But I haven’t talked a ton about which LLMs I use and why.
There’s a reason for that.
I noticed back in the day (of artisanal hand coding, going uphill in the snow both ways to build things) that a lot of programmers would be super dismissive and bullying about which language/program you talked about using. Let’s say you picked up a project and built it in C++: someone might come in and declare that it is the stupidest thing ever, and you should’ve used Python. But if it works in C++…who cares? The same thing about whether you use a visual “IDE” or code from the terminal, and whether you use tabs or spaces, or prefer vi or vim or nano…who cares? Use what works for you. I always noticed and hated and tried to ignore the “you should do it this way!” unless there was a “hey, heads up, doing it this way is better because very concrete reason X,Y,Z”.
So when you read my blog posts about LLMs, you might pick up on my generic use of talking about AI/LLMs without calling out a specific one (for example, see my last post where I talked about using LLMs to build solutions for software-shaped feelings). That’s because if the first one you picked up was Claude, and you liked it – great. Use that. All of my advice regarding prompting and other stuff applied. But if you used and liked ChatGPT? Also great, advice also applies. It’s easy to read (as a non-technical person) advice that’s for ChatGPT and be confused about whether you can extrapolate it to another tool and environment. That’s now exacerbated by the fact that we went from web-based AI (think ChatGPT and Claude websites) to desktop and phone-based apps to now also agentic “CLI” (command line interface) options. There’s oodles of ways to use an LLM of choice depending on where you are, what you like, and what you are trying to do. Try one and if it works for you, great. Be willing to try other things, too, but it’s fine if it doesn’t work as well for you and you keep using what does work. (If it doesn’t work, that is a good reason to try something else, as different models are better at different things and the different tools may have different capabilities).
Here’s what I have used over time, what I’ve tried and why I’ve switched over – or not switched at all.
First, I mainly used ChatGPT (web) because that’s what was available in the early days. I found it useful especially as the models progressed. I also had tried Claude when it became available (web), but didn’t find it as useful. I tried a few times with different types of projects and prompts. It was ok-ish, but I preferred ChatGPT especially for technical projects. I also tried Gemini (web) and had a similar lackluster response. I was thrilled when there became a (Mac) app for ChatGPT, and when there became more functionality like tool integration. Before, I was having to copy in code and get it to re-write or advise, then I would copy/paste code back over. (Hey, still easier than noodling over stack overflow entries and trying to figure out how it applied to my project). But, it was burdensome. Then it got to where it could see the context of my file, but only one file. That was better but still lacked the context of everything else. However, for one-off questions about random topics and other types of non-coding work, I still preferred ChatGPT’s models overall, especially increasingly the models with thinking. I now use 5.2-thinking as the default for all my work (this was written in early February 2026; assume that in future when you read this, I will probably be on the latest thinking/reasoning models).
Note: if someone says “I used GPT 5.2” when describing what they did, you have to ask what level of thinking they had it set to. Was it auto mode? Or thinking mode? Yes, sometimes auto mode will eventually trigger thinking mode but it drastically differs based on the prompt, and I find most users on free accounts using auto don’t see it go into full thinking the way my prompts get 5.2-thinking from the start, and that influences how useful the answer is. And again, it likely doesn’t have context for the project or if it does only one file’s worth.
Meanwhile, Scott has been a big fan of Claude Code, the agentic CLI for Claude’s models. He’s very, very productive with it for work on his laptop using the CLI tools. I had on my list to try CLI tools, but I put it off for a long while in part because I had finally experimented with Cursor.
I started using Cursor to test if it was better (for me) for coding-related projects. It’s basically a desktop app that I can open a project folder in and see all the files – whether they’re XCode (iOS app) files or Android Studio kotlin or javascript or python or markdown or whatever. I don’t have to open all the different ‘run’ apps to work on the code (although I still need to use XCode or Android Studio to ‘build’ and run the simulator or deploy to my physical phones for testing, these are no longer my primary interfaces for the coding work). And, this means all the files in the project are *in context* (or, able to be searched within a prompt to give it context), without me having to go tell it to look at file A for context – it can look itself and figure out which file is relevant or has the relevant code. (This is also because of the increasing capabilities of ‘agents’ which can do more sophisticated multi-step things in response to your prompts.) Cursor allows you to pick which models you want to use, so you could limit it to just Claude or ChatGPT-related models, but I don’t – I use all the latest models. I can’t really tell a difference with this setup what model is being used (!) which honestly shocked me because from the web version I *can* tell such a difference between the two, but the Cursor-style setup that has context for the full project takes away that difference. And Cursor has been very fast to iterate and instead of having it be slow to go prompt by prompt, they now have planning mode and agents where you can start by having it plan a set of work and build a checklist (even a big one with lots of tasks) and then it’ll go do some, most, or occasionally all of it. It’s also gotten better about running things in a sandbox to test its work, so I spend a lot less time on iOS projects: for example, going into XCode and having to come back to Cursor and complain about a build error that is preventing me from testing. Instead of that happening 3 of every 4 times, it now seems like it happens only 1 of 4 times and often this is a very minor issue that it fixes with a single follow up action and I can build. So that prompt>build>test timeline loop has gotten WAY faster, even just comparing the last 3 months or so. Because I have found such success with my iOS projects, Cursor has become my go-to interface of choice harness/setup for most projects, including Android apps, iOS apps, new data science projects, and anything else that involves code and/or data analysis.
However, Cursor is a desktop app. One of the benefits of ChatGPT is that I could do something on the desktop app and walk away and go for a walk and if I thought of something, pull out my phone and add another prompt to it via the phone app in the same thread that had the same context window. (Mostly – it can’t access a code file from my phone, but whatever else was loaded in the chat history it has). This means that ChatGPT was still my mobile/phone LLM of choice. I often found myself with my phone dreaming up a new project and essentially doing “planning” mode with ChatGPT (5.2-thinking, as of Feb 2026) for scoping out a project and thinking through constraints. When I was back at my laptop, I would have ChatGPT write a summary and/or prompt to give to another LLM, then go give it to Cursor. I’d have Cursor riff on that plan and add to it, then go implement it. This has worked wildly well, but I do wish I had a way to do at least planning mode with Cursor from my phone.
But, aside from that, I have felt as productive with Cursor (for laptop usage) and ChatGPT (for phone based and non-coding usage) as Scott does with Claude Code (on his laptop; he also uses ChatGPT as his phone LLM of choice).
Lately, you might have heard about “OpenClaw” (aka “MoltBot” aka “ClawdBot” – it had a few name changes). It’s a security nightmare, so don’t just use it if you’re not thinking it through, but the TL;DR is that it’s a way to set up a way to send prompts to an LLM and have it run them on your computer, with full access to all the different tools and accounts you’ve set up. However, it’s a security nightmare and very risky, so most people shouldn’t be using it (including you, probably). The only reason I’m bringing it up is because I *wish* I had a way for mobile commands to a coding LLM that had access to my code, so I could basically instruct Cursor to work on something while I’m away from my laptop. But, I am not willing to set something up with permissions to remote control my laptop fully (which is basically what OpenClaw does), so I haven’t been able to do so.
Until this weekend.
I kept thinking that what I wanted was the ability to remotely prompt Cursor, because it has access to the full project. There are a few ways to do this, either via something like OpenClaw (nope, see above) or if you host your code on Github and run ‘cloud’ based LLMs on it. I didn’t want to do that, the projects I have are local on my computer, and I want the LLM to have context and ability to write code and edit code on that project. (Otherwise, I’ll just use ChatGPT which is sufficient on my phone for other things). This could be because I’m away from my laptop – cross country skiing in the mountains and thinking through projects and wanting to start a prompt on the drive home so it can have something for me to review and test when I’m back, or just in the other room and don’t want to go get my laptop out. If only there was a way to have Cursor check a Google Sheet, for example, for a new prompt and then go run it.
Light bulb.
Cursor (desktop) can’t, but a scheduled job on my computer could be set up to check a Google Sheet every so often and find the prompt and send it to an LLM agent that can be run on my laptop. I could have the LLM log the prompt and what it did and the output, so even though I wouldn’t see it in the ‘chat history’ of the desktop app the way I do with ChatGPT or Cursor (desktop), I could still review a summary of what it thought/did and review the code when I was back on my laptop. (Bonus: because this project folder is synced to a backup cloud that I have access to on my phone, I can review this from my phone, too!).
How did I figure this out and make it work? I used ChatGPT (as my phone-based brainstorm LLM app of choice) to talk through the idea and talk through technical options, including my ‘requirements’/preferences of not using Github/cloud based actions for this. This discussion laid out a plan and I was surprised that the Cursor CLI (as opposed to desktop) would work for this, which means I could download Cursor CLI and log in/set that up (under the same account I used Cursor Desktop with), and with a simple script I added to my Mac via Terminal, have it check the Google Sheet at the designated interval, find the prompt, run it, record the status in the sheet plus record a status in the log of the project.
So after all, I am finally using a CLI for an LLM! (Although, I will say after I downloaded it and installed and logged in just to set it up for this project, I actually hate the UI, go figure, so my resistance to CLI-based LLMs was probably an intuitive strong preference for GUI-based LLMs.) But I’m not using it directly as a CLI, my script on my Mac is calling it to do the work based on the prompt I put into a Google Sheet. Google Sheets, which I’m very comfortable with, becomes the place I prompt my code-based LLM to do remote work from. (FYI, for setup, I’m also using a free Google Cloud Console Project which you give permissions to which is part of the way it can read/write from the Google Sheet remotely.)
End to end, this setup involved 1) terminal (on my Mac); 2) Cursor CLI; 3) Google Cloud Console; 4) Google Sheets.
I will have to continue to set this up for other projects that I want to do, but the bulk of the hard work is done – the additional projects will be a few minutes of configuration and testing each time, so I’ll do that every time I touch those projects and find myself wanting to do remote work.
But this is exactly what I love about AI-driven development. You can build amazing things that would not have been in your wheelhouse to even attempt before. You can troubleshoot and fix all kinds of issues along the way on the big ambitious project that becomes a realistic option to build and implement, whether it’s just for you or it’s something that a lot of other people would use. And, you can use it to customize your environment and tools and make up completely new tools (again, which you never would’ve thought was possible to do before!) that enable you to do work in ways that weren’t possible before. I keep saying this, but it’s worth keeping a log somewhere of projects that are still “too hard” and coming back to them every few months and trying them again with newer models or setups. (If you haven’t used anything with ‘agents’, you REALLY should try this on a project.)
It’s exciting to keep adding to existing projects, building new projects you didn’t have time to do before, and building the projects that you only figured out how to dream up with the help of new technology.
I have to ask myself these days, is this a software-shaped feeling?
This is a riff on something I see online more and more frequently, where people comment about recognizing if this is a “software-shaped problem”. Meaning, is this something that can be solved with software? More recently, this often means n=1 custom, boutique software that we can build ourselves. This is often easier and even faster than trying to search for something that maybe exists elsewhere and kinda works but not perfectly and requires a lot of work to tweak to the use case. Instead, now, we can spend the same (or often a lot less) time building something that perfectly fits.
I have been doing this for years. Juggling data in my head is hard – so I often turn to spreadsheets. For example, trying to figure out my enzyme dosing originally for exocrine pancreatic insufficiency – I had too many meals and too many variables to track, so I made a spreadsheet. When I then incorporated dosing enzymes for everything that I ate, that meant also everything I was eating while ultrarunning – which I did every 30 minutes to fuel. So I made a spreadsheet for that and then a template with dropdowns to use while running. I could quickly enter data that way, but Google sheets was slow to load on my phone and the extra seconds of delay was frustrating. Thus, I made a simple app I called “Macros On The Run” to allow me to more quickly open and tap the drop down and select my fuel item. Since I was building a custom app interface I could have all the summary data I wanted from my run, both hourly stats on calories and sodium consumed but also the entire per-run stats. I then was able to export my data to be able to analyze it later (particularly, also transposing it into the spreadsheet I use for food and enzyme intake). Does anyone else have this use case? No, probably not. But it was so empowering to be able to track and capture information in a format that worked well for me. And because I had learned how to build apps to build PERT Pilot to share with other people (because not everyone loves spreadsheet interfaces), I knew how to build apps, so I had the skillset that translated to figuring out how to build another app. This was before agentic AI, by the way, but this is now even easier.
Enter this week. I realized that I had expressed frustration to both my mom and Scott about a situation where I have a medicine/treatment that is done once a week, but it’s not a time-anchored or time-specific treatment. I don’t always take it Tuesday at 7pm. Depending on my schedule it could be 5pm, 9pm, whatever. But also, if I’m traveling, it can be a day earlier or later. It’s 7 days, plus or minus one day. Previously I was adding an event to the calendar for every week, and then moving it around. But I realized looking ahead at a busy summer full of travel that it was hard to move one without having to move another, because it’s not the week before that only matters, moving one also influences the chain of following events. If I usually do it on Tuesday but I’ll be traveling and not home until Thursday (and don’t want to do it while traveling), then I need to move the previous week from Tuesday to Wednesday so the following week’s Thursday is not out of the allowed ‘window’. So instead of 7-7-7, or ending up with 7-9-5 (which means two weeks are out of bounds), it becomes 7-8-6. But because these are single calendar events, there’s no alert when something goes out of bounds/out of the ‘allowed window’. Setting a recurring event (eg calendar event every 7 days) doesn’t resolve this, either. Juggling all of this in my head felt like a waste and non-optimal.
If only, I thought, I had a way to create an event type that was based on the “chain” relationship to the events before and after, that I could set to every 7 days but have an ‘allowed’ grace window of plus or minus a day, so that anything 6-8 days was allowed.
Google calendar doesn’t support this. But I know that you can subscribe to other calendars and show them, eg how I edit events in TripIt and subscribe to the calendar feed so I can see those events in Google calendar.
Thus, I found myself asking, “is this a software-shaped feeling?” of frustration? I can build apps, after all. Could I build an app that somehow publishes a calendar feed that I can see in Google calendar and see these events and get alerts when they are out of bounds? Ideally I’d be able to use Google calendar to edit these events, the way I do my other calendar events.
The mental model I had was app>feed>display in calendar. I was laying in bed, but I pulled open one of my LLMs that I have on my phone and sketched out the idea in a few sentences and asked what was possible to do and what technically it would take to do this. It brainstormed two key options, one with Google authentication and complicated multi-step back end (storage and databases and hosting and servers and all the stuff I *can* do but hate doing and doesn’t make sense for a quick n=1 prototype), and one simple one where the app would create its own iCloud calendar and then publish a feed I could see via the Google calendar. Aha, I thought, that’s it.
The next day I sat down at my laptop and used my coding LLM of choice. I asked it to build this app where it would allow me to create a ‘series’ of events with a set window (eg default to Tuesday at 7pm) and allow me to set a grace period (eg +/-1 day) and see the distance between events and flag a visual cue if they fall out of the window. It should then create events in an iCloud calendar. I would then subscribe and view it via Google calendar, so I could see it via my laptop or phone. Eventually I would see if I could edit it from those views, but for now, just being able to push and adjust from the app would be fine. (Note: my prompt was a little more specific than this, but the important part wasn’t telling it how to build the app or what I wanted it to look like. The important part is making sure it understands the end goal and user interactions so we design the backend and the front end to support what I actually want to do as the end user.)
It…did it. This isn’t a story of “one-shotting” and getting things perfectly from a single prompt, but I continue to be appreciative that the first hours of setting up a project and getting it to build on your device and get the basic functionality working that used to take 4-6 hours and lots of gnashing teeth is now a 15-20 minute endeavor, usually. And that’s what happened here, I had a working functional prototype working on my phone in about 15 minutes. I spent more time after that making it look better, testing it, adjusting events, etc, but the initial setup and functionality was a very quick process. That’s huge. For me, it doesn’t matter what the total amount of time it is to get a project ‘done’ or usable for real-life testing. You’ll see people talk about how you get 80% of the work done quicker but it ‘takes longer’ for the last 20%, but I honestly think I do way more (so it’s not just 20%) when I haven’t exhausted myself gnashing my teeth about the fundamental basic how-does-it-work and does-it-build and what-is-this-build-error.
This app probably doesn’t matter to anyone else, but if you have a use case for it and would like to try it, let me know. I called it SchedulerPilot. It creates a new iCloud calendar called SchedulerPilot that you can see on your phone, and then also subscribe to elsewhere to view (e.g. if you set it to be viewable via a link), such as in Google calendar. That means I can give Scott access to see it the way he sees my other calendars, plus view it from my browser-based calendar view on my laptop. I can’t edit events from Google calendar in the browser, but I was able to (much more easily than I expected) add functionality to edit directly from my phone’s calendar app the way I usually do on the go. I also then was able to add functionality in the app for it to flag when the in-app view and calendar view were out of sync. It shows a list of events and how they differ and I can choose whether I pull calendar changes into the app view, or if I did the tweaking in the app, push those changes back to the calendar. They automatically sync. I can also add notes to the event and ‘lock’ it so if I make other adjustments and push updates, it doesn’t overwrite it. This is key for travel-based constraints where I am definitively moving it to do when I get home from a trip, but sometimes I haven’t booked flights for the trip so looking at my calendar it may otherwise be confusing WHY the event is moved for the week. Having a lock shows it’s there for a reason, and the optional note also provides good context clue for why it’s moved. I can also add more events in the future with the tap of a button, if I’m still using this as my method for scheduling in the future (and I’m guessing I will be).
Here’s an animated demo showing the point of the app and why it’s useful:
The point isn’t convincing you to want to use my app. Most people don’t have a use case for this. But I want more people to build the patterns of recognizing when their feelings are trying to tell them something (e.g. this is a problem we could work on improving, even if it is not solvable) and build the skills of identifying when this is a software-shaped feeling. Especially when we are dealing with health-related situations and especially chronic non-curable diseases, and especially ones with treatments or medications that are not fun, it is so important to solve friction and frustration whenever and wherever we can. Not everything is a software-shaped feeling, but the more we recognize and address, the better off we are. Or at least I am, and I hope to help others do the same.
PS – If you find yourself with a software-shaped feeling and aren’t sure where to start, feel free to reach out and I’m happy to help chat and brainstorm and help you figure out which LLM tools work for you to help build software that fit those feelings. (Even if you tried a particular LLM in the past, they are frequently updating models and tools and it is worth trying again. They have gotten way better and require way less specific prompting, like I outlined here – although there may be some tips you still find useful in this post.) It used to be that you had to fund someone or badger someone to help build something if you didn’t have previous technical skills (or invest a LOT of time and energy) to learn them to do a thing. Now, you don’t have to do that, or plan to have a company to get funding to build a prototype. You can just…build things. And it’s ok if it’s “just” a n=1 solution. If it works for you, it’s worth the time. And chances are, it’ll be something that works for someone else, too. And in the meantime, you’ll have made something that works for you. If you felt like you needed permission, you have it. It won’t fix everything, but that doesn’t mean you should fixing what you can. It feels really good to have forward progress and to do something productive.
I’ve had a quote in the signature of my email for oh, something like 20 years. It says “Doing something for someone else is better than anything you could do for yourself.”
I discovered this a few months after I was diagnosed with type 1 diabetes. It sucked, I was miserable, even though I was figuring things out, because my 14 year old brain was very preoccupied with worrying that everyone would think (know) that I was different. I don’t know why that bothered me so much, except for the fact that I’m human and this is a very human thing. This is part of why I didn’t want an insulin pump, because I didn’t want people to look at me and know I had type 1 diabetes. (I grew up in Alabama: stigma against people with diabetes was strong then and honestly still is strong today.) But eventually I decided to drop that concern because I hated having to wake up every Saturday and Sunday morning to eat 60 grams of carbohydrates and do insulin shots. Waking up to eat felt stupid. So I got an insulin pump, and somewhat accepted that people would know that I have type 1 diabetes. And because of that, I decided to start volunteering in diabetes-related things, no longer worrying that people would “know” that I had diabetes. And it turns out…focusing on that, and other people, did so much more for me than anything I had been doing in the first months of living with type 1 diabetes.
I have retained this awareness and mental model ever since. Any time I start feeling overwhelming emotions, often related to or triggered by new health challenges (yay, immune systems that keep on giving new challenges) and feeling alone, I turn to a plethora of activities centered around 1) getting out and moving through space and 2) trying to do things for other people.
It works. It is very, very effective. Sometimes it’s only a momentary solution, but that brief respite in my mental suffering, so to speak, is enough to help break the cycle. I also then realize that if I find myself falling back into the same pattern, then instead of having brain cycles about that, I should instead use that brain cycle to PLAN to do my next thing, with/for other people.
I have observed lately that in these times (over say, the last 10 or so years), it seems like a lot of people would benefit from these types of strategies but maybe don’t realize they’re having these experiences and that they could intervene and break some of these recurring mental patterns. Maybe they don’t know what to do, so that’s the point of this post: a random assortment of things I’ve done over the years when I’ve hit these spots. Some of these activities I do over and over again and some are newly discovered that I’ve recently started. Some of them will feel silly to you or not a good fit for you – that’s to be expected. The kinds of things I am able to do and like to do are wildly different from what might be interesting and in your wheelhouse. But, consider this the ice breaker for you brainstorming YOUR list rather than staring at a blank page not knowing where to start – I predict looking at this list will spur a range of reactions from “ugh, that’s silly” or “I can’t do that/that doesn’t work for me” to “I could do that”.
And, why should you do this? Maybe you don’t perceive yourself to run into these situations, but…maybe you do. More and more often I am startled when, in professional contexts, someone will offer a happy holiday type wish or a “how was your X break” comment and the response is an Eeyore-style “everything is terrible ::gestures at the world::”.
From the outside, I personally have struggled with what to say in response to these (specifically talking about professional contexts). I recognize that the person saying this has a lot of feelings and feelings are valid. Yet. This is often rude and unprofessional. Why? Because you are projecting a lot of that negativity into professional spaces, which is not always the space for discussing those feelings & the situations that are contributing to them. It’s “drive-by dooming” which is contagious (negative feelings spreading) and unproductive. (I was actually struggling to figure out how to articulate why these situations were bothering me until Ken Jennings did a post thread about it – his point was about drive-by dooming on social media, but I see this pattern happen in professional contexts which has been bothering me and I think this framing applies here, too.) I still don’t know what to say, in the moment, in response to these, because I think people might be easily offended in the moment by trying to gently push back and say I hear your feelings but this isn’t a good place right now / this is not appropriate for this. (And honestly: I have observed this pattern for 6+ years so it is not political in one direction or the other, it is pretty common.)
Since I haven’t figured out what to productively say in the moment that won’t hurt relationships – while recognizing that saying nothing is inadvertently hurting relationships, too, by not helping people see when they are ‘infecting’ other people with drive-by dooming – that’s the point of this post. Maybe it will help someone recognize a reflexive pattern of doing this and give them some ideas for other avenues to address these feelings and/or break some of the cycle of these feelings.
First and foremost – go for a walk/roll/ride (however you move through space). If you’re in your pajamas, fine. No one cares. (Bonus: if it’s at night, no one can see what you’re wearing! So if it’s dark out, that’s even more reason to grab a flashlight or a headlamp and go for a walk/roll/ride.). Maybe it’s a 60 second walk around your yard or down the street and back. It doesn’t have to be far/long/etc but the point is to feel the air moving on your face and to physically move you through space. I figured this out at the start of the pandemic, that physically moving myself out of my environment into an outdoor space and “away” from the physical space where I was having those emotions really helped. Did I still have those emotions? Sure. But it became at least infinitesimally easier to work through them or feel like I was able to “step away” from them slightly. It doesn’t have to be fast, and if the weather isn’t wonderful it doesn’t even have to be outside – go to a different room in your house, even, that isn’t your usual place to sit or lay down, to get some physical separation from your ‘usual’ spots. Bonus points if it is somewhere you can open your window and get fresh air (if you’re not in a bad outdoor air situation).
Second, find something or start thinking of something that you can do for someone else. It can be tiny, it can be for someone inside your house, it can be for someone you don’t know. Even the planning to do something can be powerful, even if it’s not something you can do right away (but do follow through on that). It can be related to the things contributing to your feelings, but you have to actually do things to take action – not just sit with the feelings. And, it can be things that prevent you from seeing things that give you feelings.
What do I mean? If you find yourself ruminating over the state of your country and politics, for example, consider whether this is actually useful to you to do so. Do you NEED to be up to date several times a day on what is going on and what everyone is saying about what is going on? Really? (Unless you’re a social media manager and this is your job, or you work in politics…you maybe actually don’t?). Consider putting a timer on your social media and/or news apps to help you see if you are compulsively checking these apps or news sources. If you do need to see them for another reason, consider muting words and accounts heavily. Turn off auto-play of video content so you’re not distracted by something you didn’t come into the app to see. Curate your feed by unfollowing (which you can often do separately than ‘unfriending’) or muting accounts that you don’t need to see right now. Yes, even if it’s someone you know including a friend or family member. If they are online drive-by dooming everywhere, you absolutely do not have to see that and know what they’re doing/saying and take on THEIR feelings and contribute to your own sense of dooming.
Some digital strategies to consider:
Mute/block/unfollow
(You can mute words and accounts forever or for things like 24 hours, 7 days, 30 days)
Put a timer on apps to limit, or at least help you gauge awareness of how long you are using them
Grayscale your phone or icons
Remove apps from phone
Try a different platform (i.e. pinterest style) where it’s easier to curate a feed and/or a new platform because you can start from scratch intentionally creating a feed
Outside of phones/social media/ digital stuff, though, think about doing other things:
Sign up to volunteer at your food bank
Join a buy nothing/purchase zero type group and find an “ask” you can meet. Post a few things you’d like to give away.
Find a few books you no longer want and look up/look for your nearest “Little Free Library” and go take your books there.
Don’t have any books you can stand to give away? Go to a used bookstore and get a few, read them, and then donate them.
Live in an apartment building? See someone’s package not delivered to their doorstep (i.e. left incorrectly in the lobby)? Go carry it to their doorstep for them. Bonus: this helps you move through space!
Make/cook/bake/create a batch of something and give it to someone else. (If you need ideas and you’ve never made fudge before, try this microwave fudge recipe. Nom. Or make something you love and give some to someone else to try.)
It doesn’t have to be home baked. This year at Christmas I was feeling the un-cheer of not having big holiday plans. One of the things I did was look through my boxes of gluten free cookies and realize I have a lot of great treats from other countries (shout out to my friends in New Zealand, Australia, UK, etc) that most people don’t get to try. Also sometimes it’s hard because I feel like I have to eat the whole thing when I open it and I feel guilty if I don’t because they’re special! So two birds with one stone: I opened 4 different kinds of cookies and made a variety holiday cookie plate of GF cookies and went out one night and drove around listening to holiday music and surprised a couple of my friends/their kids by delivering a GF cookie plate. Some of the families have someone who is GF, others aren’t GF. They maybe didn’t care about the cookies but that wasn’t the point. The point was the gesture which they DID appreciate, and I got to feel the holiday spirit (and have a few cookies myself that week without feeling pressured to eat the whole package once open). If you know someone with a food allergy or is GF (celiac or otherwise), this is an AWESOME thing to receive because it’s rare for us to get a “variety” versus getting a whole batch of the same thing (which is ALSO great, but this is slightly different kind of great). But the other point is: these were packaged cookies! I didn’t make them! And I didn’t get fancy plates or anything: I put them on paper plates and put them in clear gallon ziplock bags. And that was fine.
Use AI and start a new project and have it help you learn to do something new. This could be something like building your first app or website, anything digital that you maybe thought you couldn’t possibly figure out how to do. These tools have come a long way and it’s a lot more feasible now to tackle just about any project! I went from never having developed mobile apps to developing an iOS app, another one, my first-ever Android app (with stops and starts along the way until the models got good enough to help me through it), all kinds of research and data science steps, and more. Even if you tried a year or two ago and it didn’t work – try again. The models are much, much better, and you should even think about trying again after 3 months because things are changing that much! (And AI can help with non-digital projects, too, it’s helped me think step by step on some of my first paintings that I wouldn’t have known where to start without it.)
The other thing I ended up doing a lot of this season was painting rocks. This started because I walk outside almost every day and several times over the past few years I will randomly spot painted rocks that people leave on the trail to find and move around and trade. I love seeing them. Last year someone did a few holiday ones, and this year I found myself thinking “I wish someone would do that again!”. Oh wait. Maybe *I* should do that?! After all, I have paints. I could get rocks and paint them. They probably wouldn’t be very good, but they don’t have to be. So I started looking up ideas (which is how I rediscovered Pinterest for the first time in 6 years) and found a few designs I thought I could maybe handle doing. And I started painting and realized that it would be fun to surprise people with and give them painted rocks and suggest THEY go leave them somewhere in their neighborhood/trail/wherever to make them smile. I ended up giving my first batch away without having any to put on my trail. So I made some more but they also turned into gifts. They’re not amazing (my hand muscles make it very challenging to paint straight lines for example) but a mix of practice, picking designs that tolerate mistakes, and separating how the rock actually looks (does it look like X?) rather than critiquing how I didn’t perfectly mimic the reference design, means that I’ve continued to paint rocks. I love doing this because 1) it’s fun to surprise people, 2) it gets me into a “flow” state while painting, 3) anytime I get into a negative feeling cycle I can now use the process of planning and picking out my next designs or starting my next batch of rocks (e.g. doing the base coat of paint that has to dry first) as an outlet, and 4) it encourages people to go out and put them out which is good for them (makes them happy) and will make someone else smile the way I get thrilled when I see painted rocks out in the world.
Maybe painting isn’t your thing (it wasn’t my thing until I tried it this year!), but the point is to find something that you could learn to do or use something you can do and tie it into doing things for other people. It will feel better than having the cycles of negative feelings where you feel like you can’t do anything. And maybe you can’t do anything about the situation that causes the negative feelings, but maybe you could. And if not, doing something else to distract yourself or inject more positive feelings into your life could be a great strategy to try.
Think “motion is lotion” and by doing something, anything, it will give you momentum so then you can do something else, including tackling bigger issues or problems or needs that you have.
(PS – if you have a favorite thing that you fall back to doing when you find yourself tipping into these patterns, please comment below – I’m always looking for things to add to *my* list to be able to do!)
What if you could stop the spread of infection once it arrives at your house? This is easier to do now than ever before in the era of wearables like smart watches and smart rings that gather biometric data every day and help you learn what your baseline is, making it easier to spot when your data starts to deviate from baseline. This data often is the first indicator that you have an infection, even before you develop symptoms sometimes.
But, you need to know your baseline in order to be able to tell that your data is trending away from that. And despite the fact that these new devices making it easier to have the data, they actually make it surprisingly challenging to *quickly* get the new data on a daily basis, and the software they have programmed to catch trends usually only catches *lagging* trends of changes from baseline. That’s not fast enough (on either of those metrics) for me.
(The other situation that prompted this is companies changing who gets access to which form of data and beginning to paywall long-time customers out of previous data they had access to. Ahem, looking at you, Oura.)
Anyway, based on past experiences (Scott getting RSV at Thanksgiving 2024 followed by another virus at Christmas 2024) we have some rich data on how certain metrics like heart rate (RH), heart rate variability (HRV), and respiratory rate (RR) can together give a much earlier indication that an infection might be brewing, and take action as a result. (Through a lot of hard work detailed here, I did not get either of those two infections that Scott got.) But we realized from those experiences that the lagging indicators and the barriers in the way of easily seeing the data on a daily basis made this harder to do.
Part of the problem is Apple and their design of “Vitals” in Apple Health. They have a “Vitals” feature that shows you ‘vital’ health metrics in terms of what is typical for you, so you can see if you fall in the range of normal or on the higher or lower end. Cool, this is roughly useful for that purpose, even though their alerts feature usually lag the actual meaningful changes by several days (usually by the time you are fully obviously symptomatic). But you can’t reliably get the data to show up inside the Vitals section, even if the raw data is there in Apple Health that day! Refreshing or opening or closing doesn’t reliably force it into that view. Annoying, especially because the data is already there inside of Apple Health.
This friction is what finally prompted me to try to design something: if the data is there inside Apple Health and Apple won’t reliably show it, maybe I could create an app that could show this data, relative to baseline, and do so more reliably and quickly than the “Vitals” feature?
Turns out yes, yes you can, and I did this with BaselinePilot.
BaselinePilot is an iOS app that pulls in the HealthKit data automatically when you open it, and shows you that day’s data. If you have a wearable that pushes any of these variables (heart rate, heart rate variability, respiratory rate, temperature, blood oxygen) into Apple Health, then that data gets pulled into BaselinePilot. If you don’t have those variables, they don’t show up. For example, I have wearables that push everything but body temp into Apple Health. (I have it on a different device but I don’t allow that device to write to Health). Whereas Scott has all of those variables pushed to Health, so his pulls in and displays all 5 metrics compared to the 4 that I have.
What’s the point of BaselinePilot? Well, instead of having to open Apple Health and click and view every one of those individual metrics to see the raw data and compare it to previous data (and do it across every metric, since Vitals won’t reliably show it), now at a glance I can see all of these variables raw data *and* the standard deviation from my baseline. It has color coding for how big the difference is and settings to flag when there is a single metric that is very far off my baseline or multiple variables that are moderately off the baseline, to help me make sure I pay attention to those. It’s also easy to see the last few days or scroll and continue to see the last while, and I can also pull in historical data in batches and build as much history as I want (e.g. hundreds of days to years: whatever amount of data I have stored in Apple Health).
So for me alone, it’s valuable as a quick glance “fetch my data and make sure nothing is wonky that I need to pay attention to or tell someone about”. But the other valuable part is the partner sharing feature I built in.
With partner sharing, I can tap a button (it shows up as a reminder after your data is synced) and text a file over to Scott (or vice versa). Opening the file in iMessage shows a “open in BaselinePilot” button at the bottom, and it immediately opens the app and syncs the data. You can assign a display name to your person and thus see their data, too, in the same format as yours. You can hide or delete this person or re-show them at any time. This is useful for if you are going on a long vacation and sharing a house with family members, for example, and so you want to share/see your data when you’re going to be in physical proximity but then don’t need to see them after that – you can hide them from view until that use case pops up again.
Simulated data and simulated partner data displayed in BaselinePilot.
Ideally, I’d love to automate this data syncing with partners (who agree) over Bluetooth, so you don’t have to tap to share the file on a regular basis. But, that won’t work with the current design of phones and the ability to background sync automatically without opening the app, so I’ve stopped working on Bluetooth-based solutions given the technical/policy constraints in the phone ecosystems right now. Eventually, this could also work cross-platform where someone could generate the same style file off of their Android-based BaselinePilot and be able to share back and forth, but Scott and I both use iPhones so right now this is an iOS app. (Like BookPilot, I built this for myself/our use case and didn’t intend to distribute it; but if this sounds like something you’d use let me know and I could push BaselinePilot to the app store for other people to use.)
All of this data is local to the app and not being shared via a server or anywhere else. It makes it quick and easy to see this data and easier to spot changes from your normal, for whatever normal is for you. It makes it easy to share with a designated person who you might be interacting with regularly in person or living with, to make it easier to facilitate interventions as needed with major deviations. In general, I am a big fan of being able to see my data and the deviations from baseline for all kinds of reasons. It helps me understand my recovery status from big endurance activities and see when I’ve returned to baseline from that, too. Plus the spotting of infections earlier and preventing spread, so fewer people get sick during infection season. There’s all kinds of reasons someone might use this, either to quickly see their own data (the Vitals access problem) or being able to share it with someone else, and I love how it’s becoming easier and easier to whip up custom software to solve these data access or display ‘problems’ rather than just stewing about how the standard design is blocking us from solving these issues!
What else have I built that you might like to check out? I just built “BookPilot”, a tool to help you filter book recommendations by authors you’ve already read, based on the list of books you’ve already read from your library data. If you use iOS, check out Carb Pilot to help get AI-generated estimates (or enter manual data, if you know it) to track carbs or protein etc and only see which macronutrients you want to see. If you have EPI (exocrine pancreatic insufficiency, also called PEI), check out “PERT Pilot” either on iOS or Android to help you track your pancreatic enzyme replacement therapy.
Book hangovers are the worst. By book hangover, I mean that feeling you get at the end of a book when you come up for air and don’t know what you’re going to read next. In general, or because you have to ‘world switch’ from one type of book or one genre or one era to another (my most common cause), or because you don’t have any books picked out to read next.
I get this feeling, a lot, because I read a lot (hundreds of books per year). I also listen to a lot of audiobooks when I’m out doing long distance activities that take several hours (e.g. ultrarunning, hiking, or cross country skiing). So while I read 5x more books than I listen to audiobooks, I still consume several audiobooks per month, too, but I’m picky about what I like to read versus what I like for audiobook content. I regularly and periodically peruse catalog additions to my various* libraries’ digital collections under genres I like to read and under audiobook categories, putting things on hold so I always have a pipeline of things ready to read or listen to. But, this relies on me periodically doing so, and sometimes the influx of new things to read based on those effort dries up and I have fewer books on hand than I would like, especially when I know I’m going to be reading more (e.g. I have some downtime from not feeling well and will be reading more than normal or when I’m traveling/on vacation).
It occurred to me the other day that it would be nice to be able to automatically check authors I have read for new books and to be able to put those books on hold. The problem is that I read a lot. I have dozens if not hundreds of authors I like, and while I remember a few to check, I don’t have a good way to do this systematically. My brain finally put 2 and 2 together this week when it occurred to me that if Libby (the e-book/reading app now used by most of my libraries) allowed me to export my data, I could systematically list and look up authors and check for recent/new additions to their catalog. Ooooh.
Like most things now, there are usually ways to export or access all sorts of data whenever you’re ready to use it. Libby actually now makes it easy in the app to do this, without having to request or log in to the web portal or do any obnoxious behaviors. Tap Shelf>Timeline>look at “Actions” button in the top right. It gives you not one but THREE ways to export your data, wahoo! If I have the data, what could I do with it?
(TL;DR the rest of this: in less than a day, I built a tool that I call BookPilot which allows me to take the Libby data, parse it for the books & authors I have read, check those authors for every book they’ve ever written, then display it for me. BookPilot solves the ‘what should I read next?’ problem by systematically finding all unread books from authors I have already read. I can then easily mark off books I’ve read elsewhere (e.g. read before my Libby history started or in physical format), kick out books I know I don’t want to read, and otherwise have an awesome list of books ready to go the next time I want to spend some time checking out books and/or putting more things on hold! It works really well and that’s just on the authors I’ve already read – I plan to also add recommendations for new authors that match my favorite authors, genres, etc. There is a web dashboard where you can view and interact with the recommendations as well as the ability to work with this data via the command line.)
The whole goal was to help fuel my book pipeline and to be able to recommend books that are highly probable that I want to read, based on my past reads, but to automatically filter by what I’ve already read. (That’s a problem with asking chatbots or using other tools: it’ll show you ‘books like this’ but when you read hundreds per year, you don’t remember the covers or names of all the books you’ve read so you spend a lot of time re-checking things you’ve in fact already read.)
I started by taking the Libby data export (you can get it as CSV, json, or html) and having Cursor write a script to pull the book title and author for everything I’ve read in my export. This is about 800 books and ~350 or so authors from the last 2.75 years (when I switched from Overdrive to Libby and it started recording my history; before I wasn’t having it log my reads). It then takes every single author on the list, queries the Open Library API to find the author’s Open Library ID, then fetches all their works (up to 100 books per author at a time) using the author’s works endpoint; it then supplements this data with Google Books API queries. All API responses are cached locally to avoid rate limits, and requests include built-in rate limiting delays between calls. It stores all books by each author with metadata: title, ISBN, publication date, series information, categories/genres, format availability. It then cross-references catalog books with my reading history to mark read/unread status, attempts to filter out duplicates and non-English versions (e.g. “Anne of Green Gables” and “Anne of Green Gables (German Edition)” versus Anne of Green Gables in the actual german language title and also “Anne of Green Gables / Anne of Avonlea (Box Set)” etc). It takes a while if you have hundreds of authors but the script is set up so you can start/stop it and it will pick up where you left off. The next time you check, it will check and only add books that are more recently published (customizable thresholds, of course) so future catalog checks will be quick to look for recent additions.
Then I have a dashboard that sorts and shows me all these books, ordered by series (when series info is available) so I can see a) series I have not read from authors I have already read and b) any books in a series that I have partially read; I can also sort by author’s name or highest count of the books I haven’t read, e.g. maybe I’ve read one book from an author but they have another 30 books to consider!
(On first pass, I still need to go through and mark books that I have read from >=3 years ago digitally and/or in physical form. But a quick look has already shown that this system works great and I’ve already been able to instantly add a bunch of books to my to-read list and holds already!)
I added a thumbs up feature which automatically ports a book to my “books to read” tab, which answers my “what should I read next?” question. If I thumbs down a book, it goes away from the dashboard. I can also tag “already read” (also disappears it), “not in English” (e.g. my filters missed that this is a non-English version on the first pass) or “duplicate” for duplicate titles that have somehow crept into the listing.
I have separate recommendation lists for authors I’ve listened to (audiobooks) versus authors I’ve read (ebooks), so I can also have a good queue to fill for similar audiobook content.
I have a ton (hundreds of audiobooks, thousands of ebooks) to review, based on my ~800 books read in the last <3 years, from 350+ distinct authors. It’s delightfully overwhelming to have this many recommendations! There is nothing worse than a book hangover combined with having nothing in the reading queue and having to fight the book hangover and having to simultaneously search for what’s available and what you want to read next. (It’s like feeling hangry…book hangover hangry?) This system now means I won’t have that combination problem again: I will always have books lined up to read and if not I can quickly and more easily identify off this list from my known authors where they’ve added books or they have additional series or I can (eventually) find series from the same “era”/”genre”/”world” to continue reading and pick up where my brain left off.
Eventually, I’m going to add some recommendations for new authors that ‘match’ my most-read authors in different categories. But I don’t have to, yet, because I have so many high-ROI options based on my current author list! And the next time I drop in an updated Libby export, it will add the new authors I’ve read *and* automatically remove books from my “books to read” list that appear in my reading history.
I haven’t open-sourced BookPilot yet, but I can (UPDATE: it’s now open source!)) – if this sounds like something you’d like to use, let me know and I can put it on Github for others to use. (You’d be able to download it and run it on the command line and/or in your browser like a website, and drop your export of Libby data into the folder for it to use). (And did I use AI to help build this? Yes. Could you one-shot a duplicate of this yourself? Maybe, or otherwise yes you could in several hours replicate this on your own. In fact, it would be a great project to try yourself – then you could design the interface YOU prefer and make it look exactly how you want and optimize for the features you care about!)
* Pro tip: if you live in Washington state, most county libraries have “reciprocal” agreements if their counties offer services to each other. This means that because I lived in Seattle and have a SPL card and a King County (KCLS) card, I can also get Pierce County, Sno-Isle, etc etc etc…. It’s mainly digital collection access, but this is amazing because you can have all of these library cards added to your Libby account and when you want to go get a book, you can check ALL of your catalogs. Sometimes a book is on most of these systems and I can get on the hold list for the one with the shortest wait time. Other times, it’s only in ONE catalog and I wouldn’t have been able to get it without these reciprocal county cards because it wasn’t in SPL or KCLS (my primary local libraries)! And even when books are not in any collection yet you can add a smart tag and be notified automatically whenever something IS added to *any* of your libraries. It’s amazing. Not sure if other states or areas have these types of setups but you should look to see if you can access other catalogs/get cards, and if you live in Washington and love to read, definitely do this!
What else have I built that you might like to check out? If you use iOS, check out Carb Pilot to help get AI-generated estimates (or enter manual data, if you know it) to track carbs or protein etc and only see which macronutrients you want to see. If you have EPI (exocrine pancreatic insufficiency, also called PEI), check out “PERT Pilot” either on iOS or Android to help you track your pancreatic enzyme replacement therapy.
I was asked to contribute a talk in a session at Stanford’s recent AI+Health conference. I spoke alongside two clinician researchers, and we organized the session so that I would talk about some individual patient experiences & perspectives on AI use in health, then scale up to talk about health system use, then global perspectives on AI for health-related use cases.
One thing I’ve been speaking about lately (including when I was asked to present in DC at the FDA AI workshop) is about how AI…is not one thing. There are different technologies, different models, and they’re going to work differently based on the prompts (like our research showed here about chart notes + LLM responses, as evaluated by a patient and clinician) as well as whether it’s a one-off use, a recurring use, something that’s well-defined in the literature and training materials or whether it’s not well-defined. I find myself stumbling into the latter areas quite a bit, and have a knack of finding ways to deal with this stuff, so I’m probably more attuned to these spaces than most: everything from figuring out how we people with diabetes can automate our own insulin delivery (because it was not commercially available for years); to figuring out how to titrate my own pancreatic enzyme replacement therapy and building an app to help others track and figure things out themselves; to more recent experiences with titration and finding a mechanistic model for an undiagnosed disease. The grey area, the bleeding edge, no-(wo)man’s land where no one has answers or ideas of what to do next…I hang out there a lot.
Because of these experiences, I see a lot of human AND technology errors in these spaces. I see humans make mistakes in chart notes and also in verbal comments or directions to patients. I see missed diagnoses (or wrong diagnoses) because the medical literature is like a game of telephone and the awareness of what conditions are linked to other conditions is wrong. I see LLMs make mistakes. But I see so many human mistakes in healthcare. One example from my recent personal experiences – it’s 2025 and a clinical team member asked me if I had tried cinnamon to manage my glucose levels. This was after she had done my intake and confirmed that I had type 1 diabetes. I looked at her and said no, because that would kill me. She looked surprised, then abashed when I followed that comment that I have to take insulin because I have type 1 diabetes. So I am maybe less bothered than the average person by the idea that LLMs sometimes make mistakes, say a wrong (or not quite right, even if it’s not wrong) thing, or don’t access the latest evidence base. They can, when prompted – and so can the human clinical teams.
A big point I’ve been bringing up in these talks is that we need everyone to care about the status quo of human, manual healthcare that is already riddled with errors. We need everyone to care about net risk reduction of errors and problems, not focus on additive risk.
We saw this with automated insulin delivery – people without diabetes were prone to focus on the additive risk of the technology and compare it to the zero risk they face as a person without diabetes, rather than correctly looking at the net risk assessment of how automated insulin delivery lowers the risk of living with insulin-managed diabetes even though yes, there is some additive risk. But almost a decade later, AID is now the leading therapy choice for people with insulin-managed diabetes who want it, and OS-AID is right there in the standards of care in 2026 (and has been for years!!!) with a strong evidence base.
I also talked about my experiences observing the real use of clinical scribe tools. I talked more in detail about it in this blog post, but I summarized it in my talk at Stanford, and pointed out how I was surprised to learn later – inadvertently, rather than in the consent process – that the scribe tool had access to my full medical record. It was not just transcribing the conversation and generating chart notes from it.
I also pointed out that my health system has never asked me for feedback about the tool, and that I’ve actually seen my same clinician use multiple different scribe technologies, but with no different consent process and no disclosure about chart access or any differences in privacy policy, retention timeline, etc. (Don’t pick on my clinician: she’s great. This is a point about the broader systematic failures.)
This is where I realized later people might have taken away the wrong point. This was not about me being a whiny patient, “oh they didn’t ask for my feedback! My feedback is so important!” and self-centered.
It was about flagging that these technologies do not have embedded feedback loops from ALL stakeholders, and this is more critical as we roll out more of these technologies related to healthcare.
It’s one thing to do studies and talk about user perspectives and concerns about this technology (great, and the other two presenters did an awesome job talking about their work in these spaces).
But we need to do more. We need to have pathways built in so all stakeholders – all care team members; patients; caregivers/loved ones; etc. – have pathways to talk about what is working and what is not working, from everything from errors/hallucinations in the charts to the informed consent process and how it’s actually being implemented in practice.
It matters where these pathways are implemented. The reason I haven’t forced feedback into my health system is two-fold. Yes, I have agency and the ability to give feedback when asked. Because I’ve worked at a health system before, I’m aware there’s a clinic manager and people I could go find to talk to about this. But I have bigger problems I’m dealing with (and thus limited time). And I’m not bringing it up to my clinician because we have more important things to do with our time together AND because I’m cognizant of our relationship and the power dynamics.
What do I mean? The clinician in question is new-ish to me. I’ve only been seeing her for less than two years, and I’ve been carefully building a relationship with her. Both because I’m not quite a typical patient, and because I’m not dealing with a typical situation, I’m still seeking a lot from her and her support (she’s been great, yay) to manage things while we try to figure out what’s going on. And then ditto from additional specialists, who I’m also trying to build relationships with individually, and then think about how their perceptions of me interplay with how/when they work with each other to work on my case, etc.
(Should I have to think about all this? Do I think about it too much? Maybe. But I think there’s a non-zero chance a lot of my thinking about this and how I’m coming across in my messages and appointments have played a role in the micro-successes I’ve had in the face of a rubbish and progressive health situation that no human or LLM has answers for.)
So sure, I could force my feedback into the system, but I shouldn’t have to, and I definitely shouldn’t have to be doing the risk-reward calculation on feedback directly to my clinician about this. It’s not her fault/problem/role and I don’t expect it to be: thus, what I want people to take away from my talk and this post is that I’m expecting system-level fixes and approaches that do not put more stress or risk on the patient-provider relationship.
The other thing I brought up is a question I left with everyone, which I would love to spur more discussion on. In my individual case, I have an undiagnosed situation. A team of specialists (and yes, second opinions) have not been able to diagnose/name/characterize it. I have shifted to asking providers pointedly to step away from naming and thinking broadly: what is their mental model for the mechanism of what’s going on? That’s hard to answer, because providers aren’t often thinking that way. But in this situation, when everything has been ruled out but there is CLEARLY something going on, it’s the correct thing to do.
And for the last year, the LLMs had a hard time doing it, too. Because they’re trained on the literature and the human-driven approach to make differential diagnoses, the LLMs have struggled with this. I recently began asking very specifically to work on mechanistic models. I then used that mechanistic model to frame follow up questions and discussions, to rule things in/out, to figure out where there are slight overlaps, to see where that gives us clues or evidence for/against our mechanistic model hypothesis, and to see what treatment success / failure / everything in between tells us about what is going on. Sure, a name and a diagnosis would be nice, but it’s been so relieving to have at least a hypothetical mechanistic model to use and work from. And it took specific probing (and the latest thinking/reasoning models that are now commonly available). But why am I having to do it, and why are my clinicians not doing this?
I know some of the answers to the question of why clinicians aren’t doing this. But, the question I asked the Stanford AI+Health audience was to consider why we focus so much on informed consent for taking action, but we ignore the risks and negative outcomes that occur when not taking action.
And specifically in rare/undiagnosed diseases or edge cases of known diseases…do clinical providers have an obligation now to disclose when they are NOT using AI technology to facilitate the care they are providing?
It’s an interesting question, and one I would love to keep discussing. If you have thoughts, please share them!
Introducing Vein Pilot, a solution for finding your veins so you can NOT stick them.
Wait, what?
Most people who want to find their veins do so in order to administer medications that are intravenous (in their veins). I remember getting an infusion and having a nurse who preferred using a vein finder light. It was fancy: it displayed a red light on a rectangle of skin and the veins showed up as darkly colored, so it was very easy to assess them.
Fast forward to more recently when I’m trying to do a home subcutaneous infusion, with several needle sites, every week. At one point, I had inserted a needle and then realized blood was flowing up the tube. Oops, hit a vein. I had to pull that site out and not use it for administering the medication. (And, as someone who is a delightful bruiser, I had quite the bruise for weeks).
This made me nervous knowing that could happen again, because my needles/sites are split from the same set of tubing, and if I hit a vein and have to pull one out, I have wasted that needle/site and it then messes up how I would do the rest of my infusion. It would require additional time and using a full other set of infusion needles, since I can only administer so much per site and dropping one site would put the others over the limit. That means then I have to figure out how to split the cartridges across the remaining sites and keep a cartridge or two to split over another set of sites. This costs an extra hour of time, a backup set of sites (which luckily I have but not everyone has backups) AND causes additional ‘lump’ risk post-infusion (because every needle causes trauma to the tissues that about a third of the time leaves a loose or consolidated lump that can take anywhere from one to a bunch of weeks to go away.) So this nervousness isn’t “I have to stick another needle in!” but a more complex, nested “I have to rethink and redesign this infusion and it’s non-optimal, time-consuming, and has long-term post-infusion impacts, too”. It’s a risk for every single needle which is multiple per week, every week, for the foreseeable future. (Although it’s only happened 1/88 so far…)
As a result, I became very cautious about trying to see where the veins were in the areas I was trying to infuse in, but this is challenging. I have limited areas to infuse in, because I can’t reach some areas that are allowed – and also because I have to juggle real estate for my insulin pump, which also infuses into subcutaneous tissue, and CGM. This leaves my outer thighs, my inner thighs, and my abdomen as possible infusion sites that I can actually reach for these bigger volume infusions. And…these thigh/abdomen zones have a lot of veins. It’s not always easy to see them, depending on the light or how I’m positioned, but I definitely want to avoid them.
I started venting to myself the other day about the situation – limited real estate, lean areas that are hard to infuse in that further limit where on the thighs and abdomen I can comfortably infuse in, plus the veins limit the real estate further and cause additional stress at the time I’m going to insert the sites. Ugh! But, one thing I’ve gotten progressively better at is trying to categorize which of the things that are bothering me are modifiable. Maybe not “fixable” completely, but could they be modified to be a little bit better? I have a lot of experience now doing this with software solutions (PERT Pilot, MacrosOnTheRun, spreadsheets galore, Baseline Pilot, Book Pilot, etc. – many of my ‘software-shaped feelings’) but I also increasingly, thanks to LLMs, have started to consider physical, hardware solutions for things, too.
It’s not my default skillset, so I don’t always think about it, but in this scenario I remembered and was thinking through the light that the nurse used. I looked it up, thinking maybe I could buy one (or insurance might rent one). LOL, nope: these things are $2000+. But I looked into how they work – by shining light, identifying the contrast, then displaying a dark ‘map’ of the veins back. That helped me realize that the consumer grade “solutions” that are shining a light aren’t doing quite the same thing. I also looked at the reviews for the consumer grade options, and they are terrible for the $200 devices. Plus the shape didn’t seem like it would be usable for my use case. I tried to see if anyone had made DIY versions that were better, and there were a few 3D printed type devices that you add light strips into, and that made me think – could I try to build one?
Same lights, different purpose.
I ended up brainstorming something more simple than the ‘vein finder’ DIY projects. Their goal is to find the veins to stick them directly – I want to avoid them! But maybe the lights could be used similarly.
Instead of a “circle” (or open circle) which most of them are designed around, I decided I wanted to try a simple ‘fork’ or a rectangle (with light strips on two sides and the ends blocked) to position light pointing inward to a spot, to try to illuminate the tissue so I could see the veins more clearly than with bare eyes and room light. My LLM brainstorming partners had suggested using a combination of red + amber lights. I decided I would buy cheap light strips (you can find them in the range of $5-20 depending on length, color, etc.) and see if they worked, then iterate on a 3D printed type ‘fork’ or rectangle to use to help limit light leakage away from the area I was trying to illuminate. But I never ended up finishing iterating because…
I bought red light strips ($5 set) and amber (orange, $13 set) light strips. I got them and plugged them in to the 12-volt dimmer switch we happened to have, plus some light strip LED strip-to-wire connectors. (We originally got and had these connectors when we put up bright white LED light strips in our closet to add closet lighting. Having these on hand made it so I only had to buy the new colored light strips to prototype this idea, otherwise I would’ve bought the dimmer and strip-to-wire connectors.)
I first took the red light and put it against my leg. It didn’t really help, I couldn’t see the veins well. I couldn’t tell if that’s because I didn’t have it set up in the intended fork design – a light on each side, slightly angled inward, with tape on the outside to limit light leakage – or if the red light was non-optimal for lighting up my skin or if it’s the particular design of the light strip I had gotten.
I tried the amber (orange) light next, expecting it also to not work for the same reasons but, as I moved it across my leg, I SAW THE VEINS! They were dark. It is actually the *motion* of the light that helps, because my eyes then ‘see’ the dark vein based on the light moving, so my eyes pick up on the dark ‘line’ of the vein on either side of the light strip as it moves. By moving it over an area in different directions, I can pick out a vein, then move the light and watch for other veins nearby.
Sometimes the veins fork and I can see a good spot in the “V” of two veins, or similarly they look like they’re running in parallel to each other and I can see where there’s a good spot in between. I dim or turn off the light, holding my finger in the ‘good’ zone and look on my bare skin for freckles or marks to help keep track of this location. (I could mark it with a skin-safe marker, but I have to scrub the skin with an alcohol swab before infusing and I assume that would remove the mark, so I need other landmarks to use regardless.) I can then swab/scrub it, wait for it to dry, then place the needle.
I tried it for the first time this week. I had chosen two abdomen sites and two inner thigh sites. I didn’t actually use it with both abdomen sites, because I tried the light strip with the first side of my abdomen and didn’t see anything. That could be because the light strip is currently still too long (I need to cut and shorten it for easier handling); because of the angle of my view down on my abdomen I can’t really see both sides of the light against the skin – I only see one side; or because there weren’t any surface level veins right there. So I didn’t try with my other abdomen side, either. But I did use it with both of my inner thigh sites and it was so much easier and less stress to use it to pick an area I thought I wanted to use (generally); check the area for the nearest veins, then narrow down the exact spot I wanted to target and use.
Woohoo, less stress!
If anyone ran into this post because you are looking for finding your veins so you can stick them – it would work for that, too. You’d probably want to play around with an actual 3D printed (or even popsicle sticks) structure for the lights so you could try to keep the lights in the spot and keep the vein highlighted. In my use case, I am trying to AVOID hitting the veins and don’t need to keep it highlighted beyond figuring out where they are and picking my spot. (Then I move the lights away so I can clean the site and insert, which I couldn’t do with anything within 3-4 inches of the site, because of how I hold my hand to insert this needle at a 90 degree angle – it’s different from IV access angles.) You may get benefit out of using different combinations of colored lights and orienting them differently than I do.
But if you’re like me, want to AVOID veins, an amber/orange light strip and moving it around may be good enough for this purpose. You could iterate on different shapes/structures to hold the lights, but since a single amber light strip and the motion of it works for my use case, I haven’t iterated (yet) on a better design that would improve it.
After several months on IVIG, I recently switched to subcutaneous administration (infusion) of immunoglobulin, aka “ScIG”. As per usual, I went looking for information on what it was like and comparisons to alternatives (such as IVIG) and couldn’t find much. So this post is everything I wish I knew before I decided to switch to ScIG and what would have been helpful for the transition and getting adjusted to subcutaneous infusion of immunoglobulin.
Why I thought about ScIG
For context, I don’t have the indications (diagnoses) most people have for IG, whether that is IVIG or ScIG. So my situation doesn’t necessarily translate to other diseases: I won’t speak specifically to symptoms etc. in detail, because it’s not relevant to anyone else, but what I will focus on is the general situation. My background is also relevant: I went on IVIG with a protocol of two days every 4 weeks. I noticed an improvement to IVIG in the second week of this cycle, but I had increasing symptoms in weeks 3 and 4. My doctors were not super experienced with (did not have many patients on) IVIG and weren’t aware that this is common, depending on what type of disease you have. I went to two days every 3 weeks. I still had the week 3 “dropoff”. We transitioned me to one day every two weeks, and that cut off the ‘dropoff’ of the cycle, but things still weren’t great and I was still experiencing the symptoms that caused me to need IVIG. So – this told us that my thing is autoimmune related, because IG is slightly quieting things, but that IVIG isn’t a perfect fit for me. (However, there is no other alternative treatment.) Additionally, because I was getting frequent IVs, my infusion nurse(s) gave me a heads up that at some point I might want to discuss a port with my doctor, because I am “one valve-y human being”. My infusion nurse who commented on this indicated it’s common in weight lifters (I am not) and people who do a lot of cardio (I guess I am – see ultrarunning). This can make it more challenging for IV access even though I only ever had 1-2 failed first IV’s, they wanted me to be aware that a port may be something I would need to or want to transition to. But, the idea of a port made me really nervous, in terms of the surgery required and the healing required from that. Plus I had some grief thinking about how it would be ‘committing’ me to this long term plan of IVIG, which no one really wants to do. Especially when, see above, it’s not perfectly managing everything. I started doing some research into ScIG, which my doctor was also aware of but has had zero patients on, so I had to do a lot of the research myself to understand the plans and how to transition, what to ask her to write for the order, how to push back (!!!!) on the pharmacist when they tried to change the plan, and get the timing right when transitioning from IV to ScIG.
What I knew about ScIG is that it would be subcutaneous, infusing the volume of IG under the skin in a similar way to that of insulin from an insulin pump. I knew it was different, though, in terms of the volume of liquid, and that it would involve using infusion sites and tubing for several hours every week – but then the sites get removed, so it’s infuse & done rather than being similar to an insulin pump site that stays inserted and delivers a constant infusion. The idea is once per week (although some people split and do twice per week) infusions that I could do by myself and at home once I got trained.
Pros/Cons – compared to IVIG
One big obvious advantage of ScIG is doing it myself, at home, on a schedule of my choosing. I wouldn’t have to schedule appointments and drive 30 minutes each way and deal with other people and the inconsistencies of them swapping my nurses out last minute. (Doesn’t sound like a big deal but when you run into substitute infusion nurses who unsolicited and out of context suddenly ask you if you have tried treating your (type 1) diabetes with cinnamon, and you have to point out that no, you take insulin because not taking insulin would kill you…well, the rotating cast of characters has a variety of risks in terms of how they do things infusion-wise, too.) Theoretically, ScIG should save me time, although that’s not true at first (more on that below), even though I would be doing it once a week.
Another advantage is the subcutaneous route, e.g. infusion under the skin rather than through IV access. But this is also a disadvantage, because the volume being infused is a LOT (and mine is larger than most due to my body size, it is dosed based on weight) and requires several needle sites and then infusion under the skin results in ‘pancakes’ in each area (more below). There’s the possibility of allergic site reactions happening, which fortunately didn’t happen to me, so I didn’t have to deal with red, itching, sensitive skin during or after the infusion – but I was aware that it could be a short or longer term issue.
The next advantage is not only time savings (eventually) but flexibility. It’s a shelf-stable liquid, you don’t have to keep it in the fridge. This makes it – and the supplies and the mechanical infusion pump – easy to travel with. In fact, I did my first travel ScIG as my fifth week, and it was flawless, just like at home. The only ‘concerns’ I had was remembering to bring the bag with me on the trip and not accidentally leaving it on the plane.
Cost is another big relative advantage of ScIG over IVIG. IG is expensive. IVIG is expensive because you’re paying for facility time and nurse time, and IG itself is expensive. Weirdly, even though it’s the same thing, the subcutaneous formulation of IG is less expensive. I used an LLM to research and guesstimate costs and thought the IG itself would be the same and I’d mostly be saving a few thousand dollars per month on the facility/people time. Instead, once I saw my first claim for ScIG, I was surprised that the ScIG IG formulation was a lot cheaper per gram! (It’s still expensive: but it’s less expensive formulation wise, which I wasn’t expecting).
The major cons are having to do all this (below) myself and having to subcutaneously infuse. It can feel really overwhelming when getting started, and I’m also nervous about long-term site management. This is in part because I have type 1 diabetes and have worn/used an insulin pump for 23 years, which involves rotating those sites around my body. With ScIG, you use the same general areas of the body to infuse, but it’s actually limited further because some of the areas you’re supposed to be able to use (like back of hips or arms) are impossible to do by yourself and/or aren’t feasible because of how long the ‘pancakes’ or fluid depots take to absorb, so it would be uncomfortable. This means my legs are my prime ScIG real estate, and occasionally abdomen – but I use my abdomen (and arms and back of hips and upper butt) for my pump sites and don’t want to take away my abdomen from pump site territory, so I have fewer site options than an average person looking to start ScIG. Again, unique to my situation, but managing the number of sites (below) can feel overwhelming when you have limited real estate.
None of the cons, for me, outweighed the reasons to try ScIG, but I was aware that they might eventually be reasons why I need to discontinue.
Onboarding/getting set up nightmare
I expected getting insurance approval and getting set up to start ScIG would be hard, with the hard part being prior auth from insurance. Actually…no.
The hard part was getting the doctor’s office to get the prescription/orders to the right mail order infusion company, then getting the mail order infusion company to do everything in a timely manner. I gave them a 6 week heads up that I needed (wanted) to start on November 4, because my last IVIG would be October 28, and I needed to start ScIG exactly one week after the last IV infusion, because it takes a week for ScIG to absorb and ramp up activity. The infusion company took dozens of phone calls with various people to get things to the point of finally submitting the prior authorization to the insurance company, who immediately within hours approved it. (They probably knew it was going to be a lot cheaper than IV, which I was already approved for.)
(This is likely unique to my situation). But then there was still delay after delay of the pharmacist being confused about how I would start, because of the “high” volume I was on. (It’s a normal volume for my weight, but most people who end up on IG therapy are a lot more frail and often lower body weight than I am, at the start of whatever this disease is. Thus, more volume than they usually see.) The IG formulation I’m on has FDA limits for how much volume per needle site you can do the first week and the rate per site for the first week. Those limits meant I needed to use 8 needles the first week, but that was doable: it’s actually in the infusion pump manufacturer’s guide to use 8 needles, which FDA says is allowed. But for some reason the pharmacist kept saying only 6 was possible and that I needed to split to do the dose in two days the first week, 6 needles each time. I kept telling him 8 was allowed; I was looking at the pump manufacturer’s guide AND the 510k approval documentation from the FDA. Finally he told me he was looking at the website from the pump manufacturer which ‘said’ 8 was not allowed. He finally gave me the URL, I went to look…and it said no such thing. It’s a basic calculator that was only configured up to 6 needle sites, because (7 or) 8 are less commonly needed, but it’s possible either by running two pumps each with 4 needles, or, PER THE FDA APPROVAL, using a ‘y-connector’, which is an approved part they just order just like the infusion sites. Neither pharmacist nor pharmacy manager had ever seen/heard of it and even though they could order it, it just broke their brains over and over again, but after 8 phone calls we finally got everyone sorted on the fact that I would do one day, 8 needles, and that was that. Then I got passed to the scheduler who said after the 6 weeks advance notice, no one had scheduled me, and they couldn’t send a nurse to me on November 4. WHAT! Then there was back and forth about how it needed to get pushed back a week – which means I needed to go get IVIG again and then ScIG a week after that. I was going to do that, but it turns out I was essentially evicted as a patient from the IV place I go to (!) without knowing it, so they would’ve had to re-set me up completely with new prior auth etc. Finally, luckily, we found a slot for my ScIG start/training at an ambulatory center, and so the plan was to go there instead of a nurse coming to my house for my first infusion/training.
TL;DR: coming from IVIG, insurance approved the swap to ScIG without any denials. The infusion pharmacy was weirdly the process nightmare, when they shouldn’t have been. I am simultaneously mad and thankful that I was informed and aware enough to know what the plan should be, advocate for actually following that plan, and questioning if someone says something that doesn’t make sense. Sometimes they’re doing things the easy way or the way it’s been done for other people, even when that is irrelevant to your care. After this first infusion though, it gets easier, because after this they’ll be mailing a box of supplies to my house every month.
First ScIG (training, nurse supervision)
I was really nervous going into my first ScIG, in part because I didn’t know what to expect. Thanks to people who post pictures and info on Instagram and Reddit, I had searched for “ScIG” and “subcutaneous immunoglobulin” and the IG product’s name to at least see pictures of what the sites and infusion pump looked like, which helped. But I knew I was going to be using 8 needles and I was nervous that they would hurt and that the infusion would hurt and I wasn’t sure how long it would take for things to stop hurting after. (Spoiler alert: it was a LOT better than I was fearing of the worst case scenario, comfort-wise!)
The first appointment at the ambulatory center took a lot of time because we had to do onboarding type stuff and open boxes and a lot of supplies. We got everything set up and laid out, and the nurse did the priming of the tubing and inserted the first two needles for me. Then I did the rest. I was pleasantly surprised that inserting the needles did not hurt – which I thought was because we used lidocaine cream (more on that below), and covered it with tape and let it sit for 20 minutes before we started. I found it slightly challenging to gently hold the plastic ‘wings’ of the site after I had inserted the needle while I placed the large piece of tape down, to securely hold the site, but this is probably because of the muscle weakness/clumsiness (why I’m getting IG), and I’ve gotten better over time. But that was the hardest part of the first infusion, which tells you that it wasn’t really that hard to do. Once you get the needles placed, you put the first syringe (attached to the tubing and your sites) into the pump, and pull back the spring-loaded plastic mechanism: it’s not electronic, let alone powered, like an insulin pump, just a spring-loaded plastic device that applies constant pressure to the end of the large syringe. Then you turn the pump on (a mechanical on/off switch) and it basically makes some noise as it pushes the tab at the end toward the end of the syringe, and then that pressure is what starts the infusion. (Pressure on the liquid into the tubing; not pressure on or near the sites). I did feel when the infusion started and it felt a little uncomfortable – not painful. But I got used to the feeling since it was constant and it was fine from there on. Because of the volume I’m on, I swap cartridges a few times during my infusion, which is easy (twist one off, twist one on, re-start the pump). At the end, you stop the pump, gently pull the tape off the sites and pull the site straight out, put gauze pressure to stop any bleeding, then pop a bandaid on, and you’re done.
All in all, it was better than I expected, but I did still feel overwhelmed at the idea of doing this all every week, even though I knew I would gradually decrease the number of needle sites, which would help. But the thought of doing the next one a week later felt overwhelming, especially because it took about 18 hours after the infusion was done for the fluid depots or “pancakes” as I call them to fully absorb, and my legs were uncomfortable. I didn’t want to get bumped or bump anything where I had infused and I didn’t want to let the cat walk across my legs. Subsequent ScIGs though have confirmed (see below) that it has gotten more comfortable over time and if I do have an uncomfortable site, it is pretty much all gone 16-18 hours after my infusion ends, so it doesn’t drag on.
I left the ambulatory center with the pump and supplies I would need for the next 3 weeks of infusions. I went home and rested the rest of the day, because my muscles were worn out from the way I sat in the infusion chair (and was tensed with stress). That’s probably specific to my situation.
After I got home from my first ScIG, I had boxes of supplies to go through. I waited a day, then when I had more energy, sat on the floor and spread everything out and sorted it into piles so that I had a bag with the supplies (IG boxes of cartridges; needle sites; tubing; gauze; bandaids; etc.) divided up for each week. That way, each infusion I just had to grab a bag and the pump and wouldn’t have to sort through a mountain of supplies. That was a good call, because it made it a lot more simple for my first at-home, by myself, ScIG.
Note: they offered to send a nurse to my home for ~2 more visits or that I could go back to the ambulatory center, and my insurance would easily cover that. But, I felt confident after the first one, because I also came home and made notes of what I would do and checked my supplies above and had anchored the process in my mind so I felt confident doing the second one myself.
Second ScIG (home, solo)
I was nervous, again, about doing my next ScIG as my first one alone, because it felt like there were a lot of supplies and steps to do. This includes starting with “pre-meds” of taking Tylenol and a Benadryl in advance. There was also putting on lidocaine cream in the spots where I was going to stick the needles. For the second infusion, I was “only” doing 6 sites, but that’s still a lot. I put on lidocaine cream and stuck squares of press and seal over them. This was recommended by the infusion nurse, and also because they didn’t send tape in my box to accommodate doing this, even though they did send lidocaine cream. The press and seal seemed to work ok, but it added time where I needed to do it before I started setting everything up because it needed to sit for 20-30 minutes. I also had to be careful not to brush off the press and seal, so that felt physically stressful. Once I had everything set up (all the cartridges opened; tubing connected to sites; the tubing primed; the pump set out), I was able to sit and pull off a press and seal square; use gauze to wipe off the cream; use an alcohol swab to clean the area, then grab a needle and pull off the rubber band, pull back the wings, remove the needle guard (and put the rubber band and needle guard somewhere I wouldn’t drop later for the cats to eat), and insert the needle. Like the first time, I found placing the tape on each site challenging. The ‘site prep and insertion’ process felt like it took forever. Then once that was done, I unclamped my tubing and turned the pump on, and whoosh – we were off. Like before, I jumped a little when the infusion started but it didn’t bother me after that. Everything went smoothly, but I did feel like I noticed the pressure over time in a few of the six areas (but not all) during the infusion. After the infusion was done, I did the same process of peeling off tape gently, then pulling off the site, then gauze pressure, then bandaid. Then I was done! I was pretty pleased with myself but again, exhausted from sitting up and doing it, so I decided I would do my next one laying down to save muscle energy.
I was satisfied with only having one training and glad I didn’t bother asking for a second nurse visit to supervise, so I was able to do this on my own schedule. I realized I liked doing it starting in the early evening so that when I would’ve been home sitting around anyway…I could be home sitting around and infusing while I read or listened to a podcast. I was already appreciating the schedule flexibility!
Like the first infusion, my legs were uncomfortable after the infusion, and overnight. It again took about 16 hours before that feeling went away. I also noticed a few days later that one of the sites that had bled a little when I pulled the needle out, had a slight bruise. I made note of that so I could avoid the area for the next few infusions (more on site rotation below). But other than that, no issues with the first solo home infusion, which was my second ScIG.
Subsequent ScIGs, site rotation
Each week has gotten a little easier, to the point where (after 5 weeks) it now feels routine and manageable.
It does help that I was transitioning down in the number of needle sites. During week 1 I used 8; week 2 I was able to use 6 (because I wasn’t limited by the first week safety limits on volume per site); and week 3 I went down to 5 sites.
I didn’t realize at first but even if you want to use fewer sites than you have needles for, e.g. you have a set of 6 sites and you want to use 5, you can clamp one of the sites and only insert 5. So even though I was sent home with 6 and 4-sites for my three weeks, the pharmacist confirmed over the phone that I could clamp and do 5. I actually ended up doing 5 sites in weeks 3, 4, and 5. I wanted to transition to 4 sites, but this will result in a larger volume per site and take a little bit longer. I have one more set of faster tubing (which is what determines the speed; the pump applies constant pressure and the tubing determines the speed) but I can’t switch to it until week 6, so I stayed on 5 sites with the medium speed tubing for a few weeks. However, in week 3, I did notice a few sites bruised underneath the skin. They weren’t painful, but I could feel a slight lump exactly where the needle had been under the skin. The pharmacist confirmed this was likely a hematoma (i.e. a bruise or tissue clot) from the site insertion and if the skin was not raised, red, spreading, etc – it should heal and go away on its own. Most of them have, but I have one that is still there three weeks later. It’s not a big concern, but I am keeping an eye on the rate at which I get these bruises and whether that impacts what areas of the legs I can infuse in. It also factors in to wanting to use fewer needles per week, because these lumps seem to be more related to the simple presence of a needle under the skin than to total volume per site or the speed: I will confirm the latter when I graduate on week 7 to the fastest tubing speed possible. It doesn’t happen with every site, so I’m not sure if that’s just a leaner area (where I have more muscle and less fat) or if it happened to be somewhere I accidentally bumped or pressed it down while taking off the tape, etc. Regardless, because of some combination of any of those reasons, I’m planning to eventually go down to 4 sites per week. This will make it easier to rotate, because I can do one each on the inner and outer thigh of each leg, and it will be easier to track week by week. In the meantime, in week 6 I also tried shorter needles. Originally, I was given 9mm. 6mm is also an option, and this matches the length of my insulin pump infusion sites, which suggests it should be sufficient length to reach my subcutaneous tissue with ScIG, too. The insertion was a little easier (because I have to push in 3mm less of needle length into the skin) and I’ll need a few weeks to see if that reduces my under the skin bruising rate.
I was very cognizant the first two weeks about making sure my needle sites were more than 2 inches apart. My first week I had all 4 needles in a square, two inches apart from each other. That was technically fine, but my ‘pancakes’ or fluid depots ended up bumping into each other and made my legs more uncomfortable. For week 2 I did kind of the same thing, avoiding the previous needle areas and being two inches apart, but one set of pancakes touched whereas the other leg and other areas didn’t…and those areas with pancakes that didn’t touch were more comfortable. I realized I needed to optimize for enough distance apart so the pancakes don’t touch each other, and preferably away from last week’s pancake spread area. That causes me to have to pay more attention when I am still using 6/5 needles a week because I’m focusing on my legs. The more I keep the sites separated, the easier they are. In fact, I began using my inner thighs in week 4 and week 5 and while some people say (and the nurse repeated to me) that they are ‘sensitive’, it actually did not hurt at all to put the needle there – even without lidocaine cream in advance – and I couldn’t feel the infusion during or after. Awesome. That gave me a lot more real estate than just my outer legs, and since I have a lot of muscle on the top of my thighs but plenty of fat on the inner and outer side thighs, I try to target using there, and keeping them separate from each other + last week’s sites works really well.
I did on week 3 also try abdomen sites for the first time. I didn’t want to use this area much because I want to preserve it for insulin pump real estate, but I tried it. It was fine, but I also have to be cognizant of pants waistbands/not putting pressure the next day while it’s still sensitive. It doesn’t hurt by default, but it is uncomfortable to have tight clothing against the pancake, whether that’s a tight legging/pant leg or a waist band. Or in my case, a back brace that I wear – so I’ll only use my abdomen site occasionally when I know the next day I don’t need to be wearing my back brace for riding in the car or sitting up unsupported somewhere. (Again, much of this is unique to my personal situation).
Why did I stop using lidocaine cream? A few reasons. One is that it was a hassle and added time to needing to do that then wait 20-30 minutes before I started. It also involved using gauze to wipe it off and then alcohol swab and then go to insert the needle – but by the time I wiped it off and cleaned it, I couldn’t always see the spot that had been lidocaine creamed! So one time I ended up inserting definitely not in the cream spot and I could tell a difference, but it didn’t hurt. So the next time I tried without it (week 4) and it went fine. I have had one (out of the 12) needle slightly hurt as I put it in but that’s because I went super slow and didn’t quite break the skin so I need to try again. Now, since I’m not doing lidocaine cream, I find it easier to use the alcohol swab and clean a much larger area (think a two inch square) rather than just cleaning the inch around the lidocaine cream spot and that way I can just pinch the area and insert without having to find the magical spot and worry about whether it’s right, and it’s faster. The other reason is because I looked it up and apparently you do need to put tape (not just press and seal) on the lidocaine cream so it can get through the skin barrier. Press and seal keeps it from getting on your clothes but doesn’t actually help it get through the skin barrier, so it’s mostly placebo. Argh. I’m frustrated that the nurse gave me wrong information and that the pharmacy didn’t send tape in the first place. I could have asked them to send it in the next box, but I was tired of arguing with them and it doesn’t hurt and it is a lot easier (for me) without the whole process.
The other thing that has made things easier over time is that weeks 3-6, I chose to lay down in bed while infusing. I sit up to get everything inserted and start, then lay down and read a book on my phone or listen to a podcast. This may be unique to my situation with my muscles, but I found that while I’m still a little tired the next day, it’s a lot more manageable when I rest during my infusion.
TL;DR (this section): keep an eye on the ‘pancake’ or fluid depot of where the liquid goes. If you’re like me, you may find that the tissue there is sensitive for a week or two and so while you can insert nearby for your next infusion, you may (like me) prefer to keep them spread farther apart to limit discomfort.
Traveling with ScIG
One of the major benefits is the ability to travel with your ScIG. You can really do it anywhere and it’s nice that it’s shelf-stable, so other than not letting the IG itself get too warm (package says keep it below 77 F and also don’t freeze it), it’s not something you have to think much about. If you’re like me and you take each shipment and organize it so each ‘week’ is in a bag ready to go, it’s as easy as being at home to grab the week’s bag + the pump bag and taking it with you.
The one thing to think about is managing your ‘sharps’ at the end of the infusion. My nurse told me I can use scissors and cut the needle ends off the tubing, and put the needles in a sharps container, and throw everything else (tubing, tape, cartridges) in the trash. To save space in the sharps container, she suggested cutting the needle ends off. So at the end of each infusion, when I pull a needle site out, I place it into a (very) small tupperware container and use scissors to cut the tubing. The needle part drops into the tupperware container. I do that with all needles, then put the lid on and give it to my husband who goes and puts it in the big sharps container in the other room. When I did my first travel ScIG, the only supply that I didn’t bring with me and needed was a pair of scissors for this (and opening some packets), but we were staying at an rental house that had them. Otherwise I would’ve found a way to wrap them thoroughly in bubble wrap or similar to bring them home and then dispose of them. But since I have this little tupperware container (one inch tall), I put labels on it that says “SHARPS” on the top and the side in case I need to show TSA my bag and disclose yes that I have sharps but they should be labeled and sealed for safe transport while traveling.
When I’m at home, I have been using a little laptop table set on the bed that I put my sterile drape on top of and lay out supplies onto. During my trip, I ended up cleaning and using a ‘cookie sheet’ with a lip in the same way, putting the sterile drape on top and using it like a big tray to hold everything. That was actually so convenient I’ve switched to doing that at home, because it makes it easy to set everything up and do my site insertion, then move the tray and myself onto the bed to lay down for the infusion and have everything I need (other cartridges during; gauze and bandaids and scissors at the end) in arm’s reach.
Resupply and dealing with the pharmacy
After my first infusion I was sent home with the rest (three weeks’ worth) of the supplies. I got a call from my patient navigator from the infusion company two weeks later to talk about my next box. I needed to get it early because of travel after the Thanksgiving holiday, and luckily they had no problem shipping it the Tuesday before Thanksgiving. They went over everything that would be in my box and I was able to make requests about which number of sites and tubing I wanted. I was also able to speak to a pharmacist (this time, someone with a better clue about things) about the ‘lump’ bruises under the skin and my needle choices and talk through things, so generally that felt like a smooth process. I also ran into an issue where I got my supplies and had everything they ordered, but they didn’t send me more gauze. Because I had been doing lidocaine the first few times, it meant I used up my box of gauze wipes for the first month and they sent me zero gauze the second month. But I called them back and they shipped just a box of gauze to my doorstop easily and without hassle, which was nice. So thankfully despite the annoyance of onboarding and getting set up, the re-order process has generally been fairly reasonable to deal with and easy to correct mistakes. That’s a good reason to sort your supplies within a few days of them arriving, and put them into each ‘week’ of what you need, so you can see if you’re going to run out of anything. In my case, I know I need to make sure there are more bandaids in my third box, because I sorted the end of my bandaids into the second box’s worth of supplies.
How much time does ScIG take? Does it save time compared to IVIG?
The first infusions take longer than the others, especially the very first one where you are limited to very conservative per-site volume limits and per-site flow rate limits.
The rest of this is influenced by how many sites; what tubing speed; and what volume you are getting, which is determined by your body weight. The fewer needles means it actually takes longer (despite the same size/speed of tubing) because at some point the infusion dispersion under your skin slows down. Therefore, more needles is faster, so if you want to prioritize time saving, you would prefer more needles (and faster tubing, if you can tolerate the higher speeds). For me, I care less about the total time, but I am happy that in week 7 when I can try transitioning to the fastest possible tubing, for my volume that will mean going down to 2h15-2h30min infusion times (depending on whether I am using 5 or 4 sites) as opposed to the 3h30-3h50min infusion times (for 5 or 4 sites) that I’ve been doing on the tubing speed I have now. As I mentioned, on top of the infusion time, it takes me about half an hour (sometimes less now without lidocaine) to open and prep everything and insert and tape all the sites. It also takes me 15-20 minutes to take everything out, because I am trying to go slow and put pressure on each site to minimize bleeding and lumps before placing bandaids, so 5 sites times 2-3 minutes of removal means 15 minutes of removal, minimum. (People who don’t typically have bleeding/bruises/lumps maybe can do this faster than I do.) All in all, right now it’s a 4.5 hour ish process for me, but in a few weeks it should go down to 3-3.5 hours overall and feel more manageable. Again, that’s because it takes time to transition down in the number of needles and transition up in tubing speed.
But for the first month or so, I’m spending about 1.5x time total than what I would be spending (including drive time) for an IVIG session every two weeks. But starting week 7, I will go down to matching the time it would take to do an IVIG session every two weeks versus ScIG every week. For me, timing wasn’t a big factor, and again, for most people with lower volumes etc. this math will probably work out better in their favor for ScIG being faster/less time than IVIG, depending on volume and regimen, etc.
The verdict of ScIG versus IVIG after 6 weeks of ScIG – and is it worth it?
I was lucky (in a sense, after being unlucky by getting whatever disease this is) that ScIG clearly works for me. I started to feel/notice a difference within the end of the first 7 days from my infusion, and it’s continued to improve things from there. Unlike IVIG (see above), I’m not experiencing a “tail off”. I was a little nervous that maybe I was just getting a first week or two “boost”, but I’m over 6 weeks in and still seeing the sustained improvement. Hooray. That made it easier to push through the first few weeks of discomfort and the learning curve of figuring out how to do ScIG, because it is clearly working for me much better than IVIG did (even on a two week cadence!!), it’s getting easier to do over time, and I’m figuring out how to optimize my site placement so it’s more comfortable. Hooray, hooray, hooray. Also, I don’t have to take as much Tylenol throughout the week like I did on IVIG to prevent or manage headaches. I still take “pre-med” doses of Tylenol (to avoid a headache) and Benadryl (to help limit allergic reactions, although I could probably go without this since I’ve never had an allergic reaction) but most weeks don’t find myself taking Tylenol later in the week anymore like I did post-IVIG.
I am still apprehensive about long term site management but hopeful that getting down to only using 4 needles will be manageable with the volume per site and being able to rotate areas of my body that get the infusion each week. There’s a chance my disease will progress and this will no longer work. But there’s also a chance that for me, ScIG will continue suppressing my disease. The mechanism of administration results in lower amplitude difference between the ‘peak’ and ‘trough’ levels of IG, because it is slow to absorb (because it takes a while to go from pancakes into systemic absorption) and then get used by the body. That’s very different from a big bolus/dose on a single day of IVIG which gives you 100% of the dose within hours, into your bloodstream via an IV. That’s a big peak and a fast tail down to lower troughs, versus a medium ‘steady state’ on ScIG. There is also a possibility for me that I may be able to titrate down (e.g. decrease the volume) and use less, which means smaller pancakes. This won’t be a fast experiment and I won’t start testing titration strategies until 2-3 months of steady dosing on my starter dose. But it’s possible I don’t need this much, and also it is easier to test lower doses on ScIG (where I can just infuse less) without having to re-go through prior authorization and change doctor’s orders via the insurance company in order to do this. We can just…do it ourselves. That’s the whole point of ScIG and also makes titration a lot easier than IVIG.
Tips and tricks for those on ScIG
Everyone probably has different ways of doing ScIG and probably has different advice. But I wanted to share some of the things I wish I knew or figured out sooner or things that help smooth the process.
Lidocaine cream can be helpful, but not necessary. If you find the timing/taping/waiting/wiping/etc. process annoying, use one of your sites on a spot where you didn’t lidocaine (don’t forget to cleanse it, though) and try it at least once. If you don’t mind it, then you can consider skipping the lidocaine cream process next time and see if you prefer doing it with or without. You can always swap back to it, but if you’re like me and find the benefit minimal and the process burdensome, it is an option to cut back on some of the steps for infusing. And save time.
Cut a piece of cardboard (or something) with slits on the side so you can unwind your site tubing and put one per slot so it is easier to ‘dry’ prime (priming so that the IG gets close to the end but doesn’t actually end up in the needle: this cuts down on skin reactions) and also easier to grab one site at a time as you are inserting. I have a piece of cardboard I cut and keep in my bag of supplies along with the pump that I use every time.
Spread out your sites and watch where your fluid depots go and whether there’s any relationship to discomfort during or after your infusion and the tissue you’re infusing in. Areas where I’ve infused more recently or had pancake (fluid depot) edges touching tend to be more sensitive during and after. Areas that are very lean/very muscle-y tend to result in it being more of a hill/dome than a flat pancake, with less spread outward but the bigger bump can be more uncomfortable for me.
If you can, make notes of where you infused. You can draw on a piece of paper and use numbers (e.g. weeks) or symbols (e.g. x’s and triangles and boxes and stars) to track where you did sites. But per above, it’s not just about where the needle went in – it may also be that you want to think about how big the pancake was. I finally realized that each week marking down what I just infused and putting hypothetical sites marked for the next week was helpful, both in terms of making sure I was thinking about the current infusion pancake and staying far away from it, which was easier to do when the pancakes are visible as opposed to a week later right before I infuse. I actually found I most prefer a powerpoint slide where I have circles showing the pancakes, and numbers in the center representing the week, to be able to see how I’m using my real estate over time. I can also mark lumps/bruises that I want to avoid for longer than a one week gap, and this will also help me see if I have a trend of any problems and if they’re location specific or more general.
Get comfortable for your infusion time, however that looks for you. Maybe that’s finding a way to sit with a laptop tray up off your lap so you can work while you infuse. Maybe that’s being like me and finding it easier to do in the evening when you can lay down and watch TV or read or hang out with family. Don’t feel like you have to do it the way anyone else does or even the way you used to do it. I figured out that I like to have a heating pad on low that I can place over my lower legs or later push down near my feet, which is both for staying warm and cozy but also as a sensory distraction at the start of the infusion.
Take your time applying the tape over your needle sites. The first week I was anxious (at the ambulatory center) and clumsy (because my hand muscles were worn out) and my tape job was a little sloppy. Because of that, and the site placement, as the fluid depot grew one of the wings was up away from the skin, and I eventually had a little leakage (not all of the IG was going under the skin). Argh. It was a waste of IG and risked my skin getting irritated at/around the needle site because of the IG leaking. Luckily, it didn’t irritate my skin, but now I go as slow as I need to and take my time placing the tape to fully cover the wings. If I have a wing ever so slightly at the edge of the tape, I peel off the number strip of tape on the end (a bonus piece of tape you can ignore, or use as an extra piece) to make sure it’s fully covered and taped down on the ends. (Or you can use another piece of tape if needed). But ever since I started focusing on a better tape job, nothing has leaked (and after 29 sites, having only one ever leak the very first time is a pretty good rate of success!).
Use the infusion pump guide or the online calculator to see how long 1 cartridge takes to infuse. Put in the volume of one cartridge (not your full dose) and the correct size gauge and number of needles (e.g. 24G or 26G, 4 or 6 or whatever number of sites you are using), then look at the “average time” to infuse. That usually is a good estimate of how long it will take the cartridge to run. Since my mechanical pump doesn’t tell you when it’s done, you have to watch and estimate when it’s done. The best method I’ve found for doing this is starting the stopwatch on my phone every time I turn the infusion pump on. Then I can track how long it’s been and around the time I’m expecting it to finish, watch the pump and see. Sometimes it’s a little faster or slower, but it’s about right. This is useful to do if you’re watching TV or reading or working or not staring at the pump, that way you don’t waste time not infusing. I ended up making a spreadsheet that shows the number of sites and how long a cartridge takes for each of those: that way as I change from 6 to 5 to 4 needles – and change tubing speed – I can track how long it takes overall to infuse (so I can plan my schedule) and watch as I go to make sure I don’t lose 10 minutes in the middle where I’m not infusing because one cartridge is done and needs to be swapped for the next. Like during IVIG, I don’t like the uncertainty of not knowing how long an infusion will take and having to pay attention during to cartridge changes timing (because I want to optimize and minimize downtime but also not have to stare at it and babysit it), so a spreadsheet helps overall and running the stopwatch during helps track each cartridge.
Don’t be afraid to ask for help. Or rather: don’t be shy about asking for an extra pair of hands to chip in where it’s convenient. I found it less overwhelming to ask my husband to help, even though I don’t need or want him to do a lot. This is partly because I wanted him to be familiar with the supplies and process and also because it made it feel less overwhelming and reassuring the first few times. I mostly have him help at the start and at the end. I have him open the needle sites tubing and pull off the paper and unwind the tubing lines. I then get a cartridge ready to connect and together we prime the tubing. Then I do everything else myself, but after the prep part he clears away the pile of trash and at the end after I have removed and clipped all the needle ends into a mini tupperware, he takes that and deposits them in the bigger sharps container and also throws away the rest of the trash. Could I do all that? Yeah, but I don’t have to, and it’s nice to not have to do “it all”.
If you have any other tips to share with others (or me!), please do comment below to share them.
How to help someone on ScIG
If you’re reading this because someone you know or love is considering or starting on ScIG – thanks for caring. You can be a big help just by understanding what is going on and listening to us vent or share our concerns about the process or how hard it is. Because, while it is beneficial (otherwise we wouldn’t keep doing it), it is hard. It’s hard to insert needles (sometimes that’s a big mental blocker) and infuse liquid into the skin, knowing that it will sometimes hurt and often be uncomfortable. And the discomfort can last for hours to days. Obviously, you should ask the person doing ScIG what would be helpful before, during, and after.
Here are some areas you can ask whether it would be helpful/not or if they would prefer you to do (but you’re not limited to this list!):
For mail order shipments, you have to sign for the box which means someone has to be at the address. Offer to help cover part of the day when the shipment might arrive, so the person doesn’t have to lose an entire day to watch for the shipment and sign for it.
Offer to help sort supplies once they arrive: checking that everything that was supposed to come did come in the box, and organizing into weekly bags/boxes to make it easier each week to grab and go.
Ask if they want help figuring out an easy way to record their infusion sites, if they haven’t figured out a good method for them. (Could be using an app, a hand written list, a hand drawn picture, a spreadsheet, a digital picture e.g. like my powerpoint)
Ask what you can do to prepare for/during ScIG. For example, offer to carry in their supplies to where they want to set up and offer to wash your hands, lay out the sterile drape, and open supply bags, etc. I prefer to do my own needle insertions but it’s nice to have my husband help open the tubing bags and unwind the sites and lay them out (into my slotted cardboard), plus help prime so we have two sets of eyes making sure we ‘dry prime’. Offer to come take away a pile of trash after they do the insertions, so they have less ‘stuff’ around.
You could also offer to do the needle insertions, if you’re comfortable doing that and if they are comfortable/prefer someone else to do that! You can also offer to stay around – or be out of the way – when they start or during the infusion, depending on their preference. I like to have a quiet room to myself when I put the needles in, but the first few infusions I wanted my husband to come back in when I was starting (mostly because the noise of starting the mechanical infusion pump was so noisy and stressful until I got used to it), and found it nice to have him rub my feet as it started infusing, as a sensory distraction so it wasn’t just the infusion in my thighs feeling at the time I started infusing.
Because my infusions take a long time, he’ll also bring a chair in and come hang out, eat dinner with me, or putter on his phone so I don’t feel isolated from the house. (He also plays defense with the cats, who LOVE to lay on me when I’m laying down, but isn’t something I want during infusions!) There’s probably a bunch of “small” things like this that are unique to your person and your house and the situation as to what they find helpful or find not having to deal with to be a nice change from having to do it themselves. Offer a few things if you think of them, but say yes to the ones they ask for if you can – it does make the experience a lot nicer! Even if it’s something you don’t think you would care about – it doesn’t matter, it’s what they care about and what they would find helpful.
Also ask for the after process. This starts with cleanup – my husband carries away the last pile of trash and also takes my mini sharps container that I find it easiest to use (when cutting off the ends of the needle sites) and putting the needle sites into the big sharps container, as well as taking the leftover supplies and pump bag back to the supply stash.
Be aware that the infusion sites will be sensitive for a day or two: for us, that means being careful when my husband gets in the bed not to roll over and into an area where I just infused on the side of my leg, or avoiding my infusion area if he reaches over to give me a hug or comforting squeeze. I’m really sensitive the first ~24 hours and then a little less cautious but still sensitive a day or two after that, then back to normal. Some people may have longer or shorter timelines for when they want to be careful around the areas they just infused.
Overall – also be willing (and ask) to listen to any frustration, or any type of emotion people have. It’s a lot to deal with whatever disease or condition is going on that necessitates the ScIG, and then ScIG itself is painful or uncomfortable or just overwhelming and annoying to have to do on top of that. It can take a while to get comfortable with the process of doing ScIG, although it does get easier over time and you and they will find ways for it to feel easier and integrated into your life and find what works well. But, that takes time, so be patient with them and each other as everyone figures it out.
—
ScIG works for me (in a possibly very unique situation) better than IVIG does, and helps confirm that my disease is likely autoimmune related since it is responding to IG therapy, even though it’s still technically undiagnosed/doesn’t have a name (and no, isn’t one of the conditions that IG is usually used for). I am thrilled to finally be feeling somewhat better even though ScIG is not a cure but a partial bandaid (for me). A really expensive bandaid. But ScIG is a more flexible bandaid that I can do on my schedule and have control over and without having to hassle with other people’s schedules or the variety of administration approaches that comes from a rotating cast of infusion nurses at the ambulatory infusion center. And it’s cheaper than IV. But, we’ll see how long this is sustainable in terms of being able to manage the real estate that it requires to be subcutaneous. Keep your fingers crossed, please, that I can keep doing it as long as it’s working for me.
And if you’re looking into ScIG for yourself and have any questions, feel free to drop them below: I’m happy to answer questions if there’s anything about the experience you’re wondering about.
In August, I bought a Hypershell X Pro exoskeleton, for many reasons. For me, and my individual situation, it has been a huge instrument of freedom, allowing me to get back to some semblance of ‘normal’ volumes and duration of activity (at least for hiking) than I was able to do earlier this year. I put ~250 miles on it within the first 3 months of using it.
Because I’ve been using it, I joined one of the Hypershell groups on Facebook and saw them post about a contest, where they were seeking 10 people who would create user-generated content (aka, take pictures and videos of themselves using it) of their next version, called the Hypershell Ultra. It was centered around doing a ‘challenge’ hike or experience. I applied, thinking I wouldn’t get selected, because 1) I have a condition which is why I’m using it; 2) and/or I already have the Pro so they’d maybe pick people who are all brand new to exoskeletons and 3) I post a lot of trail/adventure pictures but it’s more of nature, not myself, and I don’t have a ton of followers on public platforms – I’m not really an “influencer”. But you don’t get a ‘yes’ unless you apply and try, so I applied anyway. And somehow, I was selected! That means they sent me a Hypershell X Ultra, for free. If I meet all the terms and conditions of the challenge, I get to keep it, if not they’ll want it back. But I was given it to use for free, so factor that in below accordingly (although you might be surprised when you read to the very end of this post).
Why I wanted to do the challenge and try the Hypershell X Ultra
There are a few specific reasons why I really wanted to try the Ultra and was excited about getting access to one. For context, they came out this fall and were marketed at $1,999. That’s…a lot of money. I spent $1,199 on a Pro model which was a lot (but I’m definitely getting my money’s worth from it and am glad I got it). However, as someone who just bought a Pro, I was not interested in buying an Ultra at the $2,000 price point. But I definitely wanted to try it, because the Ultra has some differences from the Pro. Namely, 1) it supposedly has reengineered motors that are more efficient, so they claimed you would get more mileage out of each battery; 2) it has Apple watch support so you don’t have to pull your phone out and unlock it and open the app in order to do certain things while active.
Those, for my use case, would be a nice improvement. In most of my hikes, I have had Scott (my husband) carry the spare battery and we swap it out mid-hike so that I can use as much power as I need. With two batteries, I can do 8-10 mile round trip hikes (and even those with ~3000+ feet of elevation gain) without fully running down the second battery. For me, and the type of adventures I’m doing, one battery isn’t enough (it handles about 4-5 miles of moderate-high intensity flat and maybe 3-4 miles of uphill adventures). So more mileage out of the same two batteries sounded great. That’s also where the watch view comes into play. I found, with the Pro model, that I didn’t like leaving adaptive mode on and instead, having it on Walking mode worked better for me (it still adapts to downhill etc automatically). (More on why about the modes in my other post). But, there are times where I would want to change the mode or would need to check the battery because I’m prone to getting in the zone and charging uphill on my hike and running the battery all the way down to 0, where it dies without warning. There’s no audio or visual cue on the device if you’re actively moving to indicate that you’re about to run the battery down – you just get to the point where it suddenly stops providing assistance and you notice it. Then you stop and change the battery. Which is not a major big deal, but the Hypershell mobile app on iOS has a long-running bug where if you don’t open your app during the hike and you manage to run the battery down to zero…it tracks none of the steps or the mileage. It’s not the only way I’m tracking mileage, but it usually means I lose 4+ miles off the lifetime mileage which I think (because I’ve now done this half a dozen times already!) is going to add up over time and influence my ability to see where I am relative to the expected lifetime of the device. (This is an app issue they should be able to fix with software, they just haven’t yet). TL;DR for that part – the Ultra has a watch app where you can change settings AND see the battery, so I’d have more of a clue without having to pull my phone out to know when I’m getting close to the end of the battery and better plan for it so it doesn’t die halfway up a hilly stretch or that I remember to open the app before that happens.
I also wanted to do it as a motivation to get back out there and do a patented, Dana-and-Scott-special, which is what we jokingly call a chicken and fox adventure day (named after the river-crossing puzzle).
A chicken-and-fox adventure is something we started doing years ago, when I got into ultrarunning. Scott runs, but he doesn’t have the patience for long, flat runs like I do. He’d rather do long distance biking (which I have less patience for), or hike. So on long ultra training days, we’d drive out to the mountains somewhere and I’d pick a running route where Scott could drop me off and then go bike somewhere long and/or interesting, and we’d meet up at the end. Often, that turned into him dropping me off then parking the car at the end of the route, then he’d bike elsewhere, and I’d run my 20-30 miles to the car, grab the car, and drive to wherever his adventure ended and pick him up. Or vice versa with dropping him off at the start and then going for my run. We have had many awesome adventures like this, where “together” we are going out for really cool adventures even though we do them slightly differently, and we have great experiences to share with each other.
In the past year and a half or so…we haven’t had those adventures, because I haven’t been running, and I can’t ride my bike in the same way, and I didn’t feel confident hiking alone for very long. But, since August, my confidence began to grow after a lot of hiking (I’ve put 40,000 feet of elevation gain into my hikes between August and now, all with the Hypershell X Pro exoskeleton).
Thinking about the Hypershell X Ultra “Challenge” made me realize that I could – and wanted – to challenge myself to get back out and do a chicken-and-fox adventure.
The challenge I chose was a chicken and fox adventure on Rattlesnake Mountain (the one in western Washington state in the US)
The adventure I had in mind was a route I have always wanted to do, which is the full end to end Rattlesnake mountain hike. I’ve done parts of it – many people have, especially from Rattlesnake Lake to the Rattlesnake Ledges, which is a famous hike near Seattle that a lot of people do. Rattlesnake Ledges is one of our favorite places to take visitors, so we’ve actually done that twice this year. The other side of the mountain is also a good hike, although more about the wander through the forest. It starts at a mountain biking shared trailhead and meanders up to a few turnaround views (e.g. Grand Prospect) that also makes for a good out and back hike. If you want to hike the entire mountain, you need two cars…or you need someone who will do part of the hike, turn around and hike back down, drive around and meet you at the other side while you hike up and over the rest by yourself.
I had mentioned this hike / idea of an up and over several times, but the idea of hiking by myself made me nervous, especially with my physical abilities changing, because I sometimes need a hand getting up or down really steep, rocky terrain and I’m less sure-footed than most people. However, after ~250 miles of experience hiking with the Hypershell X Pro, my perspective was changing, and I was less nervous hiking in general *and* with the idea of hiking ~6-7 miles by myself up and over the mountain. So I pitched it to Scott and got him to agree to be the chicken* in our chicken-and-fox adventure day, with the plan of starting our hike on the Rattlesnake Ledges side, hiking up to the Ledges, then having him turn around and hike down and drive around to meet me on the other side…while I hiked from Rattlesnake Ledges up and over the remaining segments of the mountain trail by myself!
And that’s what we did (*although Scott claims he was the raft, as the car driver, rather than the chicken or the fox).
PS – if you’re in the area and doing the Rattlesnake Ledges hike, the “Ledges” you come to are actually the “first” ledges – there are two more ledge areas that you can hit! Yes, it’s more climbing, but only a few hundred feet between the ledges and the second ledges, and then up to the third ledges. There are really cool views at each set of ledges where you can see the other ledges, so it’s worth doing on some of your Ledges hikes.
What using the Ultra was like
Like I do for all my hikes, I got out of the car at the parking lot and put it on, which entails clipping the belt around my waist, clipping on each leg strap, and turning it on by pressing the button on the device. It auto-connects to the app and your phone without you having to open your phone each time (which is why, see above, I sometimes manage to run down an entire battery without having the app open so it doesn’t record the mileage in that scenario).
(Also like on most of my hikes, I made it 20 steps from the car before someone I walked by commented on the exoskeleton. It’s always really fun to be able to share with people, because often it’s people who have previous injuries or knee problems or other challenges who have heard about them, watched a video online, but never seen one in person before!)
Based on my experience using the Pro version, I know I like to do most of my flat or slightly uphill efforts on “eco” (green) mode at about 50% power. When I get to hillier sections, I’ll put it into “hyper” (red) mode and toggle the power up as needed for a bigger boost of power on lifting my legs as I climb, but for this hike with smooth terrain with more gradual climbs, I start on my personal defaults (eco, 50%). However, with the Ultra, the ‘re-engineered’ motors mean that the settings I use from my Pro don’t feel strong enough to assist me at the same level. I found myself bumping up to “eco” 75% to feel closer to what I experience with “eco” 50% on the Pro. (I thought maybe this was a one-off, but that does seem to hold true across a couple weeks of using it.)
Like using the Pro, having the Hypershell X Ultra makes it so I could do this full hike. It’s not a short hike: the full Rattlesnake Mountain hike is marked as 10.2 miles but from parking lot to parking lot it is closer to 10.9 miles and I tracked over 3,000 feet of elevation gain. I could do “just” the Rattlesnake Ledges hike (4.3 miles round trip, ~1100 feet of elevation gain), I could do the other side, but my muscles would be too fatigued to safely do a 10+ mile hike, so we wouldn’t even try it without an exoskeleton. And, there’s no way I would have considered doing it alone. Which…I did!
Scott hiked up with me to the main Rattlesnake Ledges (the ‘first’ ledges), and we took some pictures, then decided he would hike up with me to the next ledges as well. (In part because I estimated the hiking speed and he would be killing a lot of time waiting on me at the other side, and so he’d have more enjoyable views going up to the extra ledges than hiking through the forest without a view on the other side). We went up to the next ledges, and then he handed over my poles and headed back down the mountain, while I took off up the rest of the mountain…by myself!
(Earlier this year, I found that I needed to use hiking poles on uphill climbs to help me compensate for the very specific leg muscle function I was impaired by. But with the exoskeleton helping target lifting my leg, I have found that I rarely need poles going uphill anymore. Instead, we usually carry them folded up and bust them out of the backpack and use them for stability/confidence on downhill terrain. When Scott turned around, I still had another few thousand feet of elevation gain to go, so I didn’t need the poles, but I took them with me just in case and also so that I had them for the downhill side, which I would do solo.)
We swapped batteries before Scott left, so that I had a fully charged battery for my solo segment. I think at the time I had used only ~40% of the first battery. In retrospect, I should’ve kept the other battery with me, but I didn’t (we put it in his backpack).
I hiked up all the way to East Peak, which is the farthest I had ever been up this side of the trail. I eventually crested onto a ridge where there was a logging area and really clear views on both sides – and the weather had cleared so I had several miles of visibility south to see areas that I had never seen before! I saw one trail runner pass me between this section and Grand Prospect, but otherwise I had over 4 miles solo with no one else in sight…and no concerns about my ability to cover the distance, alone, up in the mountains. Which was so, so, cool. (My only hesitation came with the occasional blowdowns of trees across the trails, one of which was a little challenging to climb over. Otherwise, it was smooth sailing along the trails by myself.)
I made it over to Grand Prospect and took a picture to document being there, because this marked the section of the trail I was familiar with. At this point, I still had 4 miles to go to the trailhead! Right after this, the trail began trailing downhill into the forest and this was where I was glad I had my poles, because although this trail is very smooth (as far as trails go), it had rained pretty heavily the previous two days and was muddy and slippery in a few places. Eventually, as I meandered down and was about 1.7 or so miles from the trailhead, I suddenly noticed my legs felt heavy. I looked down and…no lights. I had run down the full battery on the exoskeleton. Oops (see note above about my partially charged battery being with Scott). Luckily we had planned for Scott to hike up and meet me (rather than sitting around at the car), so I had less than 10 minutes before he reached me and we swapped the batteries back. Ahhhh, that felt so much better. (Although you don’t lift your legs as much on downhill terrain, you still lift your leg and that’s specifically where I have muscle impairment that is really aided by the exoskeleton, so it is night and day even on flat or downhill terrain for me when I use the exoskeleton versus walking without it. So I was glad to have my powered assist back on!)
We finished out the hike at the mountain biking shared trailhead, on the other side of Rattlesnake Mountain. I did it! I was so jazzed. I had been confident about the mileage and elevation, because since August I have done some other hikes in this ballpark of elevation gain and mileage, but it was really rewarding to feel confident enough to do that many miles up on a mountain ridge all by myself and feeling confident enough to deal with whatever situations would arise while hiking solo. And I would not, at this point in my situation, have done this without an exoskeleton.
I can step up and over things more easily. This could be stepping up onto a rock step, or up and over a branch on the trail. These things used to require poles more often; see above where now I very rarely need poles for the uphill even when stepping up and hiking up a long series of rock steps!
I also less often ‘need’ poles for downhill smooth terrain, like most of the Rattlesnake Ledges hike. I still like having them for trying to move quickly, or for wet/slippery terrain, or bigger step downs, but for rolling smooth terrain I often will go without for the downhill. I didn’t feel like that was even a choice before!
Because I can get my legs moving back at a reasonable pace for both flat walking and for hiking, I found that I can actually get a good cardiovascular workout again. Meaning, I used to be limited by my legs rather than my cardiovascular system, and my heart rate rarely was elevated and I couldn’t push myself because I was leg-limited. Now, I can actually walk briskly and raise my heart rate intentionally; same for hiking. This is huge for my overall health.
At the end of hikes and walks, because the rest of my muscles are less fatigued for compensating for the missing muscle action, I am rarely scuffing my feet at the end of walks and hikes the way I was pre-exoskeleton. I also have less fatigue in my muscles, even though I am going farther and longer and working my legs and my cardiovascular system harder! Pre-exoskeleton, I realized that I was limiting us to 8 mile hikes and then more commonly 4-6 mile hikes. Now, I’m back up to regularly wanting to choose 8-10 mile hikes on a regular basis. (And same for elevation: I had limited us down to ~2000 feet of elevation gain hikes for a while, because of fatigue concerns for the end of hikes, and now have no problem choosing >3,000 feet of elevation hikes again!)
All of this was in play during my challenge hike. I actually chose to do this long hike, alone, because I felt like I could do it. I got more physically out of the hike, because I was able to actually locomote and activate my cardiovascular system more, because I wasn’t wasting all my energy just moving my legs. I didn’t need my poles for going uphill. And I didn’t scuff my feet or trip on the entire hike, even though I was out there moving nonstop for 4 hours and 15 minutes!
What using the Ultra is like, compared to the Pro
Remember that my review/experience is skewed by having a lot of experience with the Hypershell X Pro. If you want to read my gushing about how exoskeletons are an instrument of freedom and the best thing since sliced bread for me lately –read my previous post about it. Otherwise, keep in mind this is mainly a comparison between the Pro and the Ultra, rather than never having used an exoskeleton then trying the Ultra.
You should take away from my first blog post (really, read it first if you haven’t!) and this one so far that exoskeletons are awesome and for people like me, they are a huge instrument of freedom. I never want to be without one, especially as long as I’m in whatever situation I’m in where my muscles work differently than they used to. That being said, I do see a lot of people asking online about the Ultra, the Ultra versus other models, etc, and I want to explain – from my perspective – what the differences are. And this needs a major caveat: my experience is 1) that of a person with some kind of condition that affects my leg muscles and 2) that of a person who personally bought and heavily used the Pro model before being given free access to the Ultra. Then read the below two sections because I’m going to give specific answers to what you should consider getting (or not) if you already have an exoskeleton versus what you should consider if you don’t already have one.
The difference between no exoskeleton and the Pro is probably 5x stronger than the difference between the Pro and the Ultra. The Ultra does have re-engineered motors supposedly causing it to be more efficient…but in my use case (which is likely different than the average person – remember my default ‘walking’ mode is eco 50% which is a lot higher than most people’s) I found that I had to bump the power up so much higher on the Ultra – to default eco 75% for just flat walking, and often 75% hyper mode for hills, too, then also often going up to 100% hyper for bigger hills. I rarely did that on the Pro. It is possible that I’m getting more mileage per battery, but I still don’t feel confident that it is because it’s more efficient or if they changed the power settings relative to each of those modes so I’m not using as much power as I was before. And while most people maybe wouldn’t notice that, I actually do. Because of how my leg muscles are specifically impaired, I can absolutely tell the difference between these. So I was less excited after using it, because of those factors for my unique situation.
The watch mode IS a game changer, though, for people like me who are busy hiking and not looking at our phones. It gives you a way to quickly turn adaptive mode on and off or switch between eco and hyper if you’re not familiar with the on-device button way of doing it (although it’s easy to learn: it’s a two second long press to switch you back and forth). But for me, the biggest benefit is having the watch app to show me the battery level! That helps me better see as I’m getting to the end of one battery as I often do, so I can remember to open my app (until they fix that bug) and also to look at where I am on the hike and decide if I want to go ahead and swap it out if I’m in the middle of a big steep section and don’t want to have to stop mid-climb when it suddenly dies. I did see a post somewhere that the watch app will eventually come to the other models (I hope so!), in which case this will also be a selling point for the other models rather than a differentiator for the Ultra. Update: as of early December 2025, the watch app now supports all models! So this is no longer a key differentiator.
The Ultra does look different: instead of orange and silver reflector material on the leg straps and waist belt, it is primarily black. The bars that extend down your legs are also black, because they’re the lighter carbon fiber material. I think aesthetically, the Ultra is a little more ‘subtle’ because of those color changes, especially when you’re wearing it against pants. In summer, when it’s against bare legs with shorts, I think it’ll be noticeable the same amount, but because I got access to the Ultra when I started wearing longer pants for hikes and walks this fall, it does feel like it’s less visually noticeable. Weight-wise, though, I don’t notice a difference from the carbon fiber material and the Ultra being slightly lighter overall weight than the Pro. This is something I actually considered about whether to buy the Pro versus the “Carbon” version originally..but I actually am not bothered by the Pro weight at all. The weight difference is maybe there, but because the Pro weight doesn’t phase me at all, it doesn’t feel like a big differentiator to me. However, I do see some people online who perceive the weight of the Pro to be a factor for them, so I’m guessing they’d benefit more from the lighter weight than I do.
Takeaways for those considering an exoskeleton if you don’t already have one
If you’re on the fence about getting an exoskeleton – yes, you should get one. Especially for those of us who have conditions that have changed our activity levels and patterns – it really is a game changer. The question shouldn’t be “should I get one” but “which one should I get”.
And based on my experience, I look at the math on battery, power output, and my experiences with both (see the chart on my previous post if you want to breakdown all the variables for the 3 main models outside of Ultra), and say…I still think the Pro is the best deal, for most people with the current pricing models.
The $200 difference is absolutely worth it for the higher output and second battery that you get with the Pro versus the lower “Go” model.
I chose the Pro originally because I didn’t think the main difference between the Pro and the Carbon, the weight difference, was worth $500. After using it for several months and after trying the carbon fiber (lighter weight) based Ultra, I still think that’s true.
I originally thought, before trying it, that maybe the extra mileage from the ‘re-engineered, more efficient motors’ on the Ultra would be worth it, so it would be a question between the $1200 Pro and the $2000 Ultra, with it being worth it IF you were someone like me who was really putting a lot of miles in and was regularly running down 1.5-2 full batteries per activity. But…after using it… in the current iteration, I don’t think that’s the case. (Again, my perspective might be skewed by ‘how high’ I run my default power levels, starting at eco 50% most of the time. So maybe that mileage boost is more for people who don’t by default use as much power as I do for all mileage. People who are fine with lower power output and are high mileage probably would like the Ultra.)
I still think most people are best suited by the “Pro” model. And if you’re like me and really putting the mileage in, it would be cheaper to get the Pro and later buy an extra battery or two than it would be to go for the Ultra. Unless you’re not like me and are a lower power need and also maybe someone who would notice the weight difference when wearing it.
TL;DR: you should absolutely get an exoskeleton. But, for most people, see above – go with the “Pro” unless you have specific reasons (e.g. lots of mileage and/or strongly preferring the slightly lighter weight of the device) to choose the Ultra.
Takeaways for those considering an Ultra if they already have another model
I think the same outline above applies here, which is that most people who have a Pro or a Carbon likely won’t benefit enough from the Ultra to justify an upgrade while theirs is still in good working order. I think the people who would benefit would be if you started on a “Go” model which only came with one battery and doesn’t put as much power out. Then, a switch to the Ultra is a reasonable shift for a second version exoskeleton, if you can afford it: otherwise going to the Pro gives you likely 90% of the benefit of the switch. However, a Pro to Ultra or a Carbon to Ultra doesn’t make as much sense until you wear down your existing exoskeleton and it reaches end of life, or you are someone with a Pro who really needs a lighter weight version and uses lower power output but still runs the battery down, in which case you might be the use case that is suited to the Ultra. But if you’re not in those situations, you may not have as much need to upgrade until your existing one reaches its end of life.
And who knows, maybe subsequent firmware and software upgrades will change the Ultra. If they manage to change the power levels back to something that better matches the Pro where I have more range to use the upper end of the power *and* get more mileage per battery? Then I will be a huge fan and encourage people to factor that into their decisions. But until then, see above.
—
TL;DR: I love exoskeletons, they’re an instrument of freedom. I paid $1,200 in August 2025 for a Hypershell X Pro exoskeleton and love it (still love it). In late October/early November, I was given for free a Hypershell X Ultra exoskeleton after being selected for the Hypershell X Ultra Product Explorer program and have been using it and comparing it for the last several weeks. I love the opportunity and appreciate being chosen in the explorer challenge program so I could try it, and because it motivated me to head out on a big chicken-and-fox adventure up and over the full length of Rattlesnake Mountain, which I wouldn’t be able or willing to do without an exoskeleton to support my adventuring.
Instruments of freedom are devices, tools, hacks or things that help us do more than we could otherwise, and often do more with less pain or hassle or risk.
Instruments of freedom can be small everyday things, like noise cancelling headphones that help you focus or an effective rolling suitcase that’s easier to roll through the airport. They can be anything that reduces the energy cost of doing something, or increases your comfort or confidence, or expands your choices and flexibility and independence. Instruments of freedom are for everyone, but they can be especially meaningful for people with various health conditions, especially those of us impacted by physical limitations as a result of these health conditions.
I first considered the framework of instruments of freedom a few years ago. A few years ago, my mindset went from “I don’t need poles” for hiking to “I wonder if poles might be beneficial”. I tried them, and they were immensely helpful. I didn’t know if it was because my balance and proprioception has changed ever since I broke my ankle (and later a toe), or if I would have benefited from them all along. Nevertheless, they were highly impactful for helping me power up and more confidently come down hills. As my body changed for other reasons (a new autoimmune disease affecting my lungs and muscles), poles went from optional to the only way I would be able to hike at all. But as hiking has become even harder, I have kept my eyes open for additional instruments of freedom that might be helpful. Specifically, for over a year and a half I have been wanting to try a lower body exoskeleton, but could not find one that was commercially (and easily) available, light enough, and at a price point that I was willing to pay.
Until now.
I discovered one called “Hypershell”. There were 3 versions available (“Go”, “Pro”, and “Carbon”) at the time I was evaluating them, with different price points ($999, $1199, $1799) with different features and accessories.
Here’s what the features were at the time I was evaluating them:
Hypershell Go X
Hypershell Pro X
Hypershell Carbon X
Peak “Horsepower” output
0.5 HP (400W peak)
1 HP (800W peak)
1 HP (800W peak)
Motion Postures Recognized
6
10
10
Weight of device
2 kg
2 kg
1.8 kg
Battery range
~15 km (9 miles)
~17.5 km (10.5 miles)
~17.5 km (10.5 miles)
Temperature rating of battery
IP54 & Anti-Cold
Down to −10 °C
IP54 & Anti-Cold
Down to −20 °C
IP54 & Anti-Cold
Down to −20 °C
Number of batteries included
1
2
2
(As I’m writing this in August 2025, note that they’re announcing a new “Ultra” model in September 2025 but it’s not clear yet what additional features or capabilities it will have.)
I wasn’t sure, though, if I would be able to use and benefit from the Hypershell. It’s hard to explain what my physical limitation is, but it results in me feeling like I can’t press off my ankle effectively (I wear ankle braces on both side) and there’s weakness in my thigh and hip, especially on the right side, that makes it hard to step up and over when going up the stairs and hiking. I can do it, but it’s exhausting, and it results in a weird sick-muscle type feeling after I do it a lot. I joined a Hypershell user group on Facebook and also the “Hypershell disability users” Facebook group. The second disability-based group kept cautioning that you needed to be able to lift up your foot 3-4 inches and take a step in order for the device to kick in. I was nervous about getting it and it not being able to work for me. But, there is a 2 week (14 day) return period, so I was hopeful that if it didn’t work I would be able to return it and get a refund. (But there were also not-so-great reviews of their customer service communication and the refund process, so I was nervous about that.)
I decided to get one and try it. I also specifically decided to choose the “Pro” model (see table above).
Why I chose a Hypershell Pro model instead of the Hypershell Go or Hypershell Carbon
The reasons I chose the “Pro”:
$200 difference from the base model (Go), but with the 10 motion patterns. Given that I’m hopeful that I can do more types of activities like I used to, I wanted to be able to have as much capability as possible.
More power output – the Go only has half as much peak power as the Pro/Carbon.
More range (mileage, albeit slightly)
Two batteries, including the better cold-resistant ones, on the Pro/Carbon instead of only 1 on the Go.
…but I didn’t care about the .2kg weight difference, and that was really the only difference between the Pro and Carbon. That wasn’t worth $500 between the Pro and the Carbon.
Unboxing the Hypershell exoskeleton and getting set up
Before the Hypershell arrived, I went ahead and downloaded the app. It required an email address and a password, and it also asked about height and weight. It had a decent onboarding experience in the app with videos embedded to show you how to open and get started and how to size it. The height and weight was used to give you a starting setting for the waist. But then I couldn’t do anything else in the app until I had connected the device.
When it arrived, I had low expectations for being able to use it right away, because people online talked about how long it took to charge/having a hard time charging it at first. Because of that, I expected to need to wait an hour or two of charge time before I used it and also was ready with a higher power wall plug to charge it. For some reason, the Hypershell batteries came (both) at 6% charge, but it was enough to turn on and get started for setting up the device. I was able to turn it on and get it connected in the app, do the onboarding (walking you through the first mode changes etc and taking test walks around the house in the different modes) even with it in 6% low battery status.
But then I took it off and put it on the charger to charge it up. I used the same wall plug I use for my laptop, and that was sufficient for its 65W charge rate. It takes a little over an hour to charge the 72 Wh battery up to full, and the lights on the device itself will show you (4 lights) when it’s fully charged, or you can see it in the app. It’s handy to have it lit up on the device because my husband, without access to the app, can see and change batteries to charge the next one himself.
In terms of getting set up and putting it on, it’s very straight forward. It gave me a starting suggestion to use for the waist size. I used that (and have never changed it), tightened up the waist strap and leg straps, and it was good to go from there. Once I got the waist strap tightened, I haven’t had to re-tighten or change that. I have had to tweak the leg straps a little bit here and there, partially because of how it slides around on my leg (see below re: sweating, chafing, and wearing in the summer as opposed to wearing it over a layer of clothing), but it’s quick and easy to tighten the leg strap or loosen it when needed and not a big deal adjustment wise. I did read a few people saying it slips down their hips and they got suspenders to help, but I haven’t had that experience (I’m female, so I have plenty of hip bone for it to rest against, and maybe that’s in part what makes the difference?). The first time I put it on, because I was adjusting straps, I put it on while sitting at the edge of a chair and getting everything set up and tightened, then stood up and tweaked the straps, then turned it on and began using it. Now, I can grab it and put on the waist belt while standing, then slightly lean over and attach each leg strap (so I don’t have to sit down to put it on). Because it carries the battery in the back and the design also has the support bar around the back, it’s not really comfortable to sit with for long if you want to lean back against the back of the chair, but it’s fine if you’re sitting down briefly on something (a chair, a bench, etc) if you’re not trying to lean back or sit up against the back of anything.
My first time using the Hypershell Pro X
I was conservative with my first time using the Hypershell, in part because of users in various groups warning about taking it easy and not overdoing it. (If you have no disease/physical limitation as your reason for wanting to use this, you can probably ignore this.) After it charged fully, I put it on and went for a short mile and a half walk to see how it felt.
I knew from the onboarding experience (where it has you testing different modes) that I didn’t need “hyper” mode turned on to walk. “Eco” mode is the base mode, and you can adjust the power setting either on device (pressing a button twice increases it by 25%, triple pressing it drops it by 25%) or in the app with a slider that allows you to adjust it 5% increments.
I tried 25% power for my first walk, which was enough to feel the lift pulling my thigh and knee up. It felt so good! It made walking feel smooth and easy, especially on the right side where my thigh/hip muscles are more impaired. It felt like it made my walk more balanced in terms of not slogging along on the right side compared to my gait without assistance. I noticed a sensation of a few muscles feeling activation that normally aren’t getting activated (this is probably unique to my situation), but had no soreness or issues right after or the next day as a result of this test walk.
The next day, I did my normal length walk (of about 4 miles) with the Hypershell.
The third day? I took it hiking. And…(more about this below)
Small hiccups with adaptive mode recognition (that may be unique to my gait)
I had my app set to ‘adaptive motion recognition’, which is where it detects what you are doing (e.g. walking, going downhill or down stairs, idling, etc) and adjusts the assist based on the motion. It takes a step to kick in any assist and it takes about 2-3 steps into a new pattern (e.g., starting to go down the stairs) to swap modes. This means if I was walking toward the stairs and starting to go down the stairs, it would be the second or third step down where I would feel it change into downhill mode where I could feel it providing resistance against my thighs, as opposed to lifting my thighs as I stepped down. It was also very noticeable when I got to the landing and would take the 2-3 steps to turn the corner and continue down the flight of stairs. It would feel stiff-legged like I needed to tip toe to walk and then just as it switched to walk mode, I was going down the next flight of stairs and again it took 2-3 stairs before it was back on down hill mode. Not a big deal, but it did make me aware of it. I went down the stairs (carefully) while looking at the app which shows which motion pattern it is detecting, so I was able to see (and not just feel) that it was switching those modes and that’s why it suddenly felt different.
The other hiccup was when I was out walking on the sidewalk, which is flat. It was in walking mode and I was indeed walking, when suddenly it threw a stiff legged resistance at me. Huh?! I looked at the app and it showed “downhill” when I was walking on a flat surface. Weird. It reverted back to walk mode after 2-3 steps. It happened again later on my same walk. I must have something weird about my balance or gait that leans backward (?) or otherwise causes it to sense downhill, so it shifts to downhill mode. It didn’t trip me but it did make me go “woah” and I didn’t love it because I wanted to just be able to forget and walk without thinking about wearing it.
So as a result, I decided to turn off adaptive motion recognition and use it in ‘manual’ mode, rather than having it auto-detect. I’ve used it in “walking” mode ever since as my default mode, and it works great. It also still auto-detects and shows you what motion it detects in the app, but even with over a dozen miles of flat walking, it’s not thrown the downhill resistance in unexpectedly again. And, even in walking mode it still provides enough support and resistance for actually going down the stairs/downhill, regardless! So I get the same benefits without the risk of the sudden incorrect downhill resistance.
Kicking the tires of the Hypershell Pro X with hiking. A lot of hiking. Three days in a row!
Before using Hypershell, I could still hike. I used to hike three days in a row almost every week, but with this muscle disease, I found myself not being able to easily do it, so I would often hike Friday, rest and do something easier Saturday, then do another hike (maybe) on Sunday. This has been true for the last 6 months (or longer).
But my first hike with the Hypershell was on a Friday, and it went great. I played around with using the adaptive motion recognition and found that I couldn’t tell a big difference in the assist with ‘uphill’ mode versus ‘mountain climbing’ mode versus ‘walking’ mode. Downhill mode was good, but I also tested going downhill while in ‘walking’ mode and found it was good enough. Since all of these mode changes have to be done in the app, and the exoskeleton itself covers my pockets in a way that makes it hard to get my phone in and out of my pocket (plus I’m carrying poles), I decided I would try staying in ‘walking’ mode for everything from flat to uphill to downhill…and it did great. I felt so much more at ease stepping up and over steps and rocks and powering up hills the way I used to, and I also was thrilled that the little bit of resistance to my thighs for downhill made it easier to step and control my downsteps. All of this increased ease and control somehow resulted in me not generating the ‘sick muscle’ feeling I have been getting in my legs and glutes after hiking. In fact, I felt like I hadn’t been hiking at all! I was so thrilled that we decided we would hike again with it on Saturday, a second day in a row.
I did wake up with really tight calves on Saturday…but normal hiking tight calves, the way I used to get after the first few hikes of a new season when my calves are out of shape for climbing. I was thrilled because that meant that I was activating and using my legs MORE (despite the powered assistance of the exoskeleton!) on that first hike. Tightness and all, we decided we would hike again, and we actually chose a longer second-day hike with reasonable elevation now that I felt confident I could handle more of it with the exoskeleton. And I could: the second hike was also great, and I left it in ‘walking’ mode the entire time on the way up, but did find that I wanted to use higher power settings (still in eco) as a baseline and increase it further for hills. I think I used 30-40% as my base power, then would increase it more for bigger inclines. The nice thing is that for downhill, you are using less power, so even with ⅔ or so of the battery used up on my first and uphill half of the hike, I ended up at the bottom of the second hike with just above 10% battery left because the downhill uses so much less battery. (I had it in ‘downhill’ mode for the way down, where it provides resistance on the way down but when you’re on flats it’s not lifting your legs much as it would in walking mode.)
That went so well that…we headed out for a third day in a row. My first three-day weekend in a long time! Again, we chose a long hike with more elevation than we ever would have predicted would be possible for even a second day in a row, let alone a third day. This time, I was feeling more overall fatigue (hello, three days of hiking in a row!) and so I started with 50% power (eco mode) and cranked it up on hills. I finally remembered that I could adjust power with the button on the device, double clicking to add 25% as I went up a hill and triple clicking once I was on a flat (to decrease it back by 25%), without having to pull out my phone and open it and navigate to the app and slide the toggle. That made it easier, because I could still do that with poles in my hand.
Because I was cranking up the power more on this third day in a row, I did run out of battery on this hike. This was in part because there was a pretty steep climb on our return route about 2 miles from the end (of an 8.8 mile hike), and I wanted to crank the power all the way up to 100% (still on eco). I managed to get the battery down to 10% about halfway up that steep climb, and when it hits 10% it still goes but it definitely decreases the output. So we stopped and swapped to the second battery (that I had Scott carrying in his backpack). It’s quick and easy to pop off and swap (I let Scott do it). I powered it on and it instantly reconnected to the app, I put it back on 100%, and cranked my way up the rest of the hill with relative ease. Then I bopped the power back down to 50% for the rest of the hike. One of the reasons I ran down the first battery is because on the downhill/return portion, I kept it in “walking” mode for more assist rather than “downhill” mode. Again, three days in a row meant I was more tired overall and my legs were tired (but normal tired, not disease-tired), so I wanted the extra power to make sure I kept good form and didn’t cause injury by doing an atypical gait in my fatigue.
And I didn’t – I finished the hike, tired (normal tired) and with legs feeling in no way like we had hiked for three days, even though we did.
In three days in a row (which I can’t do without the Hypershell), we hiked 25 miles and over 6000 feet of elevation gain (which I wouldn’t be able to do without the Hypershell).
Instrument of freedom, indeed.
A view of me walking on a trail through an alpine meadow with the mountain I hiked in the background. At first glance you may not notice it, but if you look you’ll see black straps above the knee, which are the Hypershell straps, and you can also see the bar that goes around the back of my hips with the black battery, and you can also see the motors on the sides of my hips. But at a glance, you may not even notice it.
Did I keep the Hypershell Pro or did I return it? Is it worth it?
By the middle of the very first day of hiking, I knew I was keeping the Hypershell.
It works so well for me, and it really is an instrument of freedom for me. I love walking even on my flat paved trails with it, again because it makes my right hip and leg movement so much closer to what I used to experience (before my muscle disease).
Between my daily walks and the first two weekends of hiking, I have put around 60 miles on foot with the Hypershell Pro.
I’m definitely keeping it. It will be interesting to see if I run into any issues with my high-mileage use. The warranty is supposed to last for a year, and the website estimates ‘normal use’ service lifetime is 3000 km (1,900 miles). If I kept up my current pace of use (averaging 60 miles in two weeks) for a year, that would be around 1,560 miles, still under the expected lifetime use. I’d probably run into that life expectancy (which doesn’t mean it’ll stop working but might be when I expect it to run into issues) in about 14-15 months (or less if I increase my mileage).
But given how much it empowers me to move in the ways I want to move… it’s worth it. And I’m excited to see what other exoskeletons are coming to the market in the future, too. There may be more options for me to consider when this one eventually breaks or wears out.
Does it help with downhill or going down the stairs?
One of the things I really was hoping the Hypershell would help with is going downhill. I have trouble exerting power all the way through my foot, which is really noticeable when I am going downhill on looser dirt or rocks, where it feels like my foot is likely to slip sideways and cause me to jolt/lose my balance. As a result, my downhill hiking became as slow as the outbound uphill hikes (instead of faster, which is common for many people and the way it used to be for me) and made me really rely on my poles for balance. Plus it was super stressful and made hiking less fun, and I also skipped a lot of hikes that had a lot of rocky steps or rocky and loose rock downhill gravel terrain. But because of the Hypershell experience on my first hike, I actually chose a pretty rocky hike for the second hike because I was hopeful that it would help my sure-footedness. And it did! So much so that my second weekend of hiking, I chose a 9 mile hike with 3,100 feet of elevation gain that had a two mile stretch of loose rock and loose dirt with a good portion (1800 feet) of the downhill elevation. And I did great, with the Hypershell on.
But I didn’t know it would help when I got it. A lot of people talked about how it ‘didn’t help going down stairs’, so I had low expectations. When I went down stairs the first time, I didn’t notice a big difference, but when I hit the landing and took those 2-3 steps toward the next flight of stairs, I could feel that stiff legged feeling that definitely indicated it was providing resistance! So it was doing SOMETHING, but sometimes it was hard to tell what it was. Over time, with more experimentation on stairs and testing ‘downhill’ and ‘walking’ mode on different downhill terrains while hiking, I realized that I could feel the thigh-based resistance more strongly when in a higher power setting. The way it seems to work is it either provides some kind of down force against the leg as you are stepping down, or it provides resistance against your leg movement. I’m not quite sure which it is, but it results in a bit of pressure against your thigh, and probably some resistance on the sides (to limit lateral movement while stepping down), and it definitely helps me.
The other way I’ve figured out how to notice it is that with higher power modes while walking (and in walking mode), you can feel the lift ‘up’ from the thigh but depending on how quickly your leg is moving you can also feel the bar pushing back down into the down step. So the motor is able to move the bars (and thus your thighs) both up and down, and that’s likely also similar to what’s happening in downhill/stairs mode, but it’s less noticeable because you don’t lift your thigh as high (or at least, I don’t) when stepping down and it’s a much subtler force against your legs. But if you have stairs with landings, that’s a great place to put it in downhill mode and feel that type of sensation when you get to the landing and take a few steps before you do the next flight of stairs down.
There is also a setting you can adjust call “hill descent control” and once you toggle it on, you can adjust it between ‘weak’ and ‘strong’ (defaults to the middle of that range). I turned mine on but haven’t experimented with adjusting the slider to be stronger, but that may be another reason why I notice a benefit on downhills, whereas other people may not have turned that on.
Is it annoying to charge?
You have to charge the battery on the device itself (with a USB-C cord, and as I mentioned a beefy enough wall charger) or in a special hub that doesn’t come with it. The special hub can charge 4 batteries at once, off-device. Mine came with two batteries and since they charge up in an hour-ish, even if I run both batteries down and get home, it’s always going to be 12+ hours before I want to use it again and that’s plenty enough time to re-charge everything, even with swapping to the second battery to recharge.
I can see how if I went to having 3 batteries and using them regularly that I might want to also get the multi-battery charger, but for 1-2 batteries and my usage, it’s generally not a big deal.
Is there anything I don’t like about the Hypershell Pro X?
I have two (ok, three) issues with the Hypershell. All are minor.
For me, the adaptive motion recognition setting triggering ‘downhill’ when I am walking on a flat surface (albeit randomly and only occasionally) is annoying. Again, I don’t know if it is because of my gait or if there’s a bug in the pattern recognition. There is a workaround – putting it in ‘walking’ mode. I have found that it’s totally fine to keep it in ‘walking’ mode when going up or down stairs, up or down hills, on varying terrain, on flat surfaces. It still provides the lift to pull my thigh up just fine, and it also does the ‘resistance’ force for downhill and down stairs the same (or very similar) to the actual downhill setting. If I want to do more, I can easily turn the power up or down using the on-device button and get more force (for either lifting or resisting), and that is faster than trying to swap modes on my phone.
The second issue is chafing against bare skin. Ohhh, the chafing. You’ll notice that all of the pictures on their website and videos are of people wearing it over pants for winter-type activities. Some people hike in pants during the summer, but I got mine in July and I don’t wear long pants to walk or hike, so the straps around my thighs are against bare skin. I didn’t have any issues for the first few walks (which were all around an hour) but my first hike, which was 3 hours, caused some chafing. So on the second day, I covered those spots with bandaids. It wasn’t enough, I ended up with more chafing spots. So on the third day, I tried putting kinesio tape on my legs where I thought spots would chafe or were already chafed. That did help, but because I’m hiking so long (3-4 hours, multiple days in a row), just like ultrarunning in dealing with pack chafing, it’s hard to deal with once you have chafed spots.
The second week, I tried additional solutions. First I tried wrapping the pads themselves with “adhesive bandages” (think ‘vet wrap’, the stretch stuff that can stick to itself). I was trying to see if just covering the back of the front thigh pad would work, because there are seams underneath it. That helped some, but the force of the corner of the pad itself was chafing. I then bought a roll of 5 inch “tubular bandages”. I got 5” because I have more muscular thighs and I wanted to try putting a piece on my leg like a leg sleeve, and then having the pads against that, so it would rub against the bandage and not my skin. It helped some, but it was still digging in at the corners. So then I tried the leg bandage sleeve AND adding a layer of that material over the pad, double wrapping it at the corners. It helped some. But again, because I already had chafing, I don’t quite know what would work best to completely prevent or eliminate chafing. (I also have tried a 4 inch tubular bandage that was black, to better blend in with the leg strap, because the 5″ worked well but really popped in color and drew the eye to my legs, whereas the black better matches the leg bars and leg straps. In terms of functionality, I like the 5″ tan color better for using as a leg sleeve actually on my leg, so I’ll probably use that as a base layer if I’m not taping as described below when I’m not actively chafed, and then use the black on top of the leg pads and around the buckles directly.)
The next thing I have tried is hydrocolloid bandages (example, there are a lot of different brands and sizes and I’ve found no difference between name brand and off brand versions) on top of the biggest already-chafed spots, with the idea that it will provide cushion and also the pad corners will be more likely to slip on that versus digging in at the exact same spot. Because hydrocolloid (“blister” bandages) stick directly on the skin, I added a bit of neosporin on top of the chafing before applying, so that the bandages don’t stick to the slightly raw skin. The challenge with hydrocolloid bandages is that they take up any fluid, like blister fluid, but also sweat – so as you get sweaty, they’re more prone to peeling up or getting rubbed off via the edges. If you have a big enough bandage that’s less of an issue, but don’t expect to be able to cover a tiny area with a tiny hydrocolloid bandage and not have it peel up from the friction of the leg strap/pad itself or have it start to come off from sweat. I also tried applying larger strips of kinesio tape on top of the hydrocolloid bandages that are smaller, and the hydrocolloid seems to provide a nice cushion against the already chafed spots and the kinesio tape helps prevent it from rubbing the hydrocolloid bandage off.
It’ll be better in winter, when I’m wearing it on top of a layer of pants, and it’s not a reason to stop using it. In fact, most people probably won’t wear it long enough even in hot weather to experience it, but I wanted to document some of the solutions I tried in case anyone else does run into it.
UPDATE: the best solution I found is:
1) as soon as I notice the chafing begin in any spot, I stop and put a strip of kinesio tape in that area. (I pre-cut kinesio tape strips and carry them in my pack).
2) if I miss preventing a chafing spot and something has rubbed, I do a combined strategy of first putting a piece of hydrocolloid tape (I bought a roll so I could cut strips rather than using bandaid-sized – it’s cheaper and easier to apply different shapes) AND then putting a piece of kinesio tape over it. Why? Because as noted above, the hydrocolloid will collect sweat and fluid under the skin and start to come up during an activity, unless it’s anchored – and it’s best to do that when you apply it. That double strategy (hydrocolloi+kinesio, applied when your skin is dry) lasts for several days or longer (I’ve had it last up to a full week, even with multiple showers per day and using the exoskeleton every day), and it both heals up the chafed raw spots and protects subsequent spots from building up. So that’s a great solution during multi-hour bare-legged hike/activity season.
We’ve now also gotten to fall and I can confirm that chafing is not an issue at all when wearing it over long pants.
The third minor issue is accessing my pockets. The motor is on the outside of my hips and although the bars curve around down the front of my thighs, the access to my side pockets on my shorts is blocked. This is where I typically store fast-acting carbs on one side (because I have type 1 diabetes) and my phone on the other side, but I basically have to stop walking and pause and really finagle my hand in under the motor and bar to access something in my pocket. It’s annoying, so I actually stopped carrying my phone in my pocket while wearing it. I decided to get a phone carrying case that mounts to a backpack strap – or in my case, a Hypershell waist strap! It lives on the strap and I’m able to slip my phone into the 4 corners whenever I want to. I also like that the webbed strap comes out of the case, so I can pull my phone off it and use it (while it’s still in the straps) and then quickly put it back on the belt mount. There’s a little more friction to the experience than without the Hypershell, but it’s 5x easier than finagling my phone out of my pocket under the Hypershell.
If you want a referral code for a Hypershell, here is a referral code.
Right after I bought my Hypershell, I automatically got an email for a referral program. If you use this code, and you buy a Hypershell, it gets you $30 off. It’s not a lot, but it’s better than nothing. Sometimes they run deals where you can get accessories for free or some dollars off particular accessories. The ones I’ve seen are usually for more than the value of the referral code – e.g. they might offer an additional battery which is a $99 value instead of the $30 off. Depending on your situation, you may like one or the other better. I mention it because it doesn’t seem like it’s compatible to use the $30 off referral code at the same time as the other deals (or it wasn’t at the time that I tried to use someone else’s referral code at the time of my purchase).
My experiences above are as someone living with an autoimmune disease that is affecting my muscles. But now that I’ve gotten it and tried it, I think I would love it even without the need for assistance with my muscle disease. Why? It’s like an e-bike for the legs. Not in the sense that it can do all the work (it can’t, it can only provide up to 20-30% assistance: you’re still doing a lot of work), but because it is an equalizer.
My husband and I have had e-bikes for years. We loved them, because of the equalizing effect. I can bike longer with e-bikes than I would without an e-bike. In fact, before we got e-bikes, we didn’t have bikes and would only sporadically ride (rentals), because biking wasn’t my thing. When we got e-bikes, we biked for dozens of miles at a time, together. I could bike at whatever power assist level I needed or wanted for the day, and he could use less assist and get more of a workout, but it enabled us to bike together (and to WANT to bike together) in ways that we couldn’t or wouldn’t otherwise.
An exoskeleton is the same situation, roughly, as e-biking in this sense. I talk to several people who ask questions when I’m out walking or hiking with the Hypershell on. Sometimes people ask about it for bad knees (I don’t have knee problems but I can imagine it would help – if you have knee issues and Hypershell experience, please share in a comment below!), but a few people have asked about it for backpacking experiences. One couple immediately said “I wonder if this would help for backpacking” and I said probably, yes – because the company advertises it to be able to do more for longer, especially with gear (e.g. they show people hiking with photography gear or big backpacks). So even without medical conditions, I could see getting a lot of use out of it when you have a pair of people who have different capabilities or range who want to go adventuring together. Especially if you’re a set of people (or an individual) who like to put in a lot of miles throughout the year…just like I am. I’ve already done 5 hikes in two weeks (plus a bunch of paved walks) and just hiking alone, that takes the per-hike cost down to $240, and will drop further each time I use it – remember that I wouldn’t have done some of these hikes at all (either because I couldn’t do them in subsequent days or I couldn’t do particular terrain at all). That per-hike cost will continue to drop over the course of the year (or more) of use that I expect to get out of this Hypershell Pro X.
How much work are you really doing when you wear a Hypershell exoskeleton? Doesn’t it do all the work for you?
Each of the two Hypershell batteries I have are 72 Wh (5000 mAh). That’s…actually not that much. It’s the equivalent to ~62 kcal if you’re thinking about food calories as a comparison. If you could continuously run the motors at full power, it would d only last 5-6 minutes. (That’s why I ran it down fast on 100% power on a really steep hill at the end of my third hike). With less power output, it goes longer time/mileage (e.g. the around 10 miles range estimation on lower power setting in eco mode), but it’s still only 62 calories of total energy, whereas I might be burning the equivalent of 1000+ calories of active energy in the course of a 3-4 hour hike. Yes, it provides power, but it’s targeted power to your legs (and there’s also heat loss), and you do a LOT of other work controlling your trunk, hips, core, arms, balance, etc. so it maybe contributes to 10-20% of energy savings. But again, you’re likely to do more – remember the e-bike analogy – and burn a lot more than you would without the Hypershell by doing more, well above and beyond anything you saved by using the Hypershell. You still do 90% of the work, for longer time and longer mileage and more elevation, resulting in more effort overall. You will still do plenty of work, but it will be easier to go further, longer, etc.
—
TLDR: I got a Hypershell Pro, I love it, and it’s enabling me to do more than I could before (in my unique situation with a muscle-related autoimmune disease). I do recommend it, for a variety of different situations, whether or not you have any physical limitations. It’s an instrument of freedom for anyone who wants it.
Feel free to ask any questions below. I can’t answer questions specifically about whether it would work for your specific setup or medical condition, but I can try my best to generalize from my experience & what I’ve read from others online.
 It’s exciting to keep adding to existing projects, building new projects you didn’t have time to do before, and building the projects that you only figured out how to dream up with the help of new technology.
It’s exciting to keep adding to existing projects, building new projects you didn’t have time to do before, and building the projects that you only figured out how to dream up with the help of new technology. The point isn’t convincing you to want to use my app. Most people don’t have a use case for this. But I want more people to build the patterns of recognizing when their feelings are trying to tell them something (e.g. this is a problem we could work on improving, even if it is not solvable) and build the skills of identifying when this is a software-shaped feeling. Especially when we are dealing with health-related situations and especially chronic non-curable diseases, and especially ones with treatments or medications that are not fun, it is so important to solve friction and frustration whenever and wherever we can. Not everything is a software-shaped feeling, but the more we recognize and address, the better off we are. Or at least I am, and I hope to help others do the same.
The point isn’t convincing you to want to use my app. Most people don’t have a use case for this. But I want more people to build the patterns of recognizing when their feelings are trying to tell them something (e.g. this is a problem we could work on improving, even if it is not solvable) and build the skills of identifying when this is a software-shaped feeling. Especially when we are dealing with health-related situations and especially chronic non-curable diseases, and especially ones with treatments or medications that are not fun, it is so important to solve friction and frustration whenever and wherever we can. Not everything is a software-shaped feeling, but the more we recognize and address, the better off we are. Or at least I am, and I hope to help others do the same. Maybe painting isn’t your thing (it wasn’t my thing until I tried it this year!), but the point is to find something that you could learn to do or use something you can do and tie it into doing things for other people. It will feel better than having the cycles of negative feelings where you feel like you can’t do anything. And maybe you can’t do anything about the situation that causes the negative feelings, but maybe you could. And if not, doing something else to distract yourself or inject more positive feelings into your life could be a great strategy to try.
Maybe painting isn’t your thing (it wasn’t my thing until I tried it this year!), but the point is to find something that you could learn to do or use something you can do and tie it into doing things for other people. It will feel better than having the cycles of negative feelings where you feel like you can’t do anything. And maybe you can’t do anything about the situation that causes the negative feelings, but maybe you could. And if not, doing something else to distract yourself or inject more positive feelings into your life could be a great strategy to try. Think “motion is lotion” and by doing something, anything, it will give you momentum so then you can do something else, including tackling bigger issues or problems or needs that you have.
Think “motion is lotion” and by doing something, anything, it will give you momentum so then you can do something else, including tackling bigger issues or problems or needs that you have.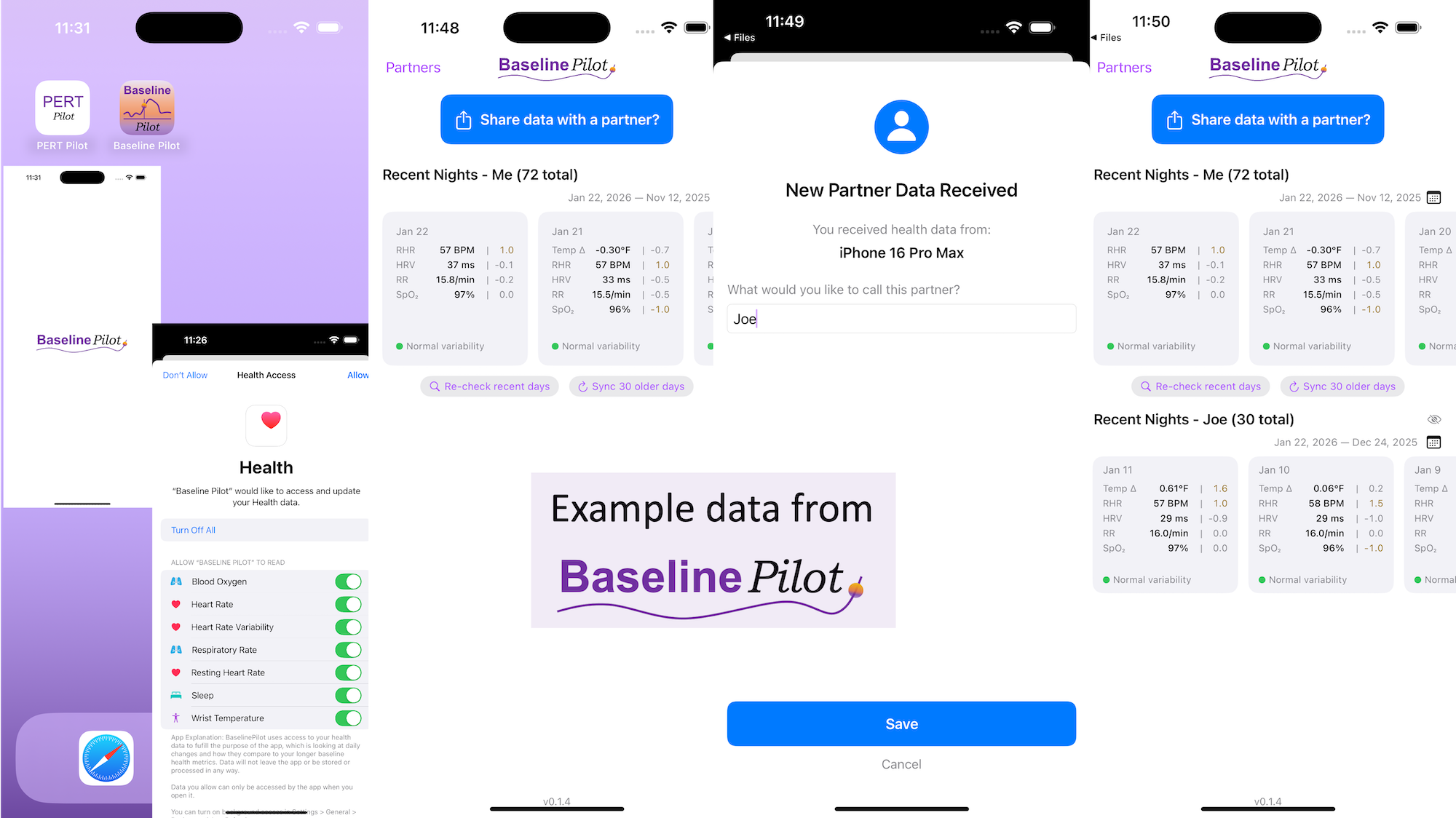
 All of this data is local to the app and not being shared via a server or anywhere else. It makes it quick and easy to see this data and easier to spot changes from your normal, for whatever normal is for you. It makes it easy to share with a designated person who you might be interacting with regularly in person or living with, to make it easier to facilitate interventions as needed with major deviations. In general, I am a big fan of being able to see my data and the deviations from baseline for all kinds of reasons. It helps me understand my recovery status from big endurance activities and see when I’ve returned to baseline from that, too. Plus the spotting of infections earlier and preventing spread, so fewer people get sick during infection season. There’s all kinds of reasons someone might use this, either to quickly see their own data (the Vitals access problem) or being able to share it with someone else, and I love how it’s becoming easier and easier to whip up custom software to solve these data access or display ‘problems’ rather than just stewing about how the standard design is blocking us from solving these issues!
All of this data is local to the app and not being shared via a server or anywhere else. It makes it quick and easy to see this data and easier to spot changes from your normal, for whatever normal is for you. It makes it easy to share with a designated person who you might be interacting with regularly in person or living with, to make it easier to facilitate interventions as needed with major deviations. In general, I am a big fan of being able to see my data and the deviations from baseline for all kinds of reasons. It helps me understand my recovery status from big endurance activities and see when I’ve returned to baseline from that, too. Plus the spotting of infections earlier and preventing spread, so fewer people get sick during infection season. There’s all kinds of reasons someone might use this, either to quickly see their own data (the Vitals access problem) or being able to share it with someone else, and I love how it’s becoming easier and easier to whip up custom software to solve these data access or display ‘problems’ rather than just stewing about how the standard design is blocking us from solving these issues!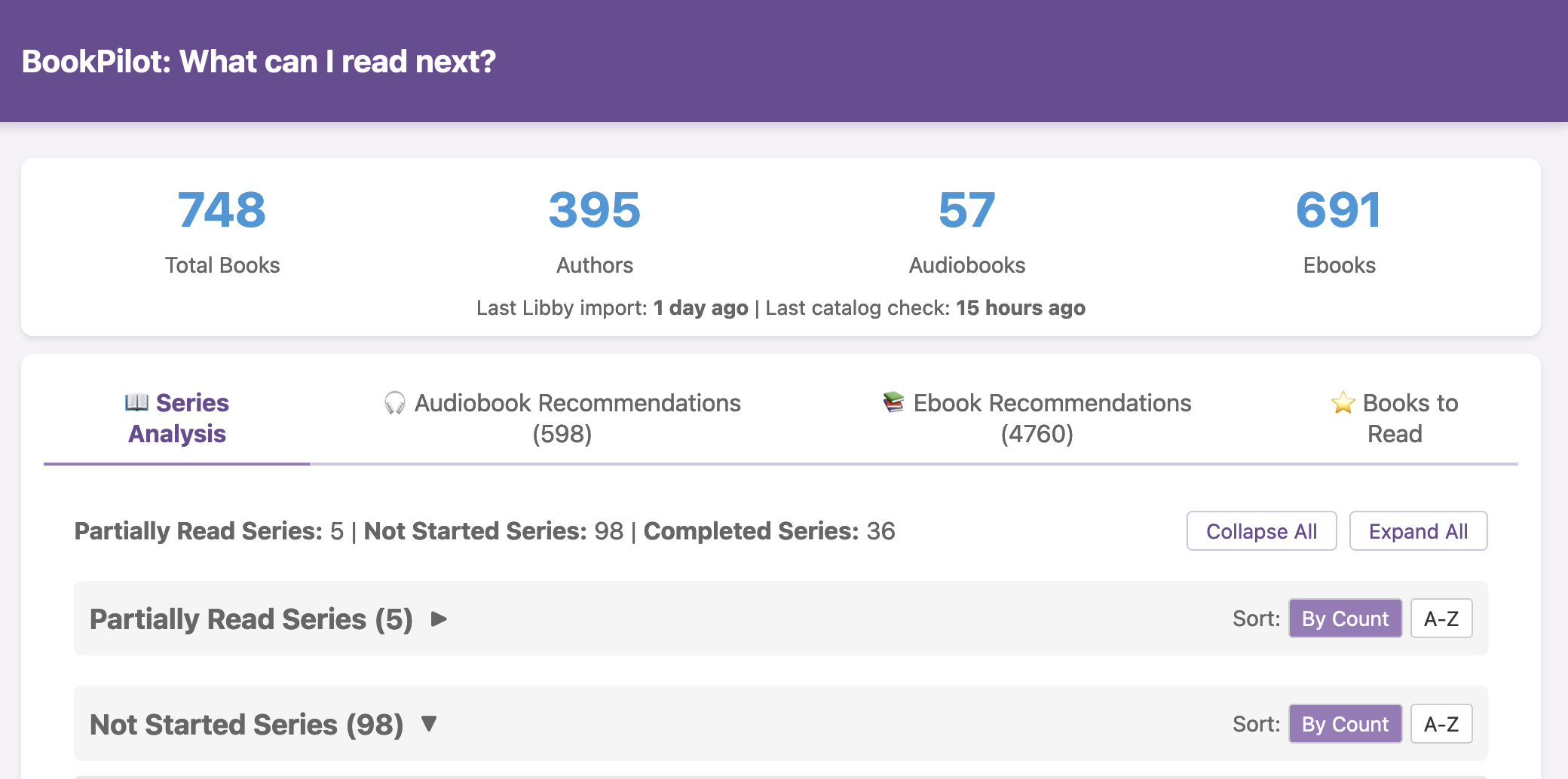
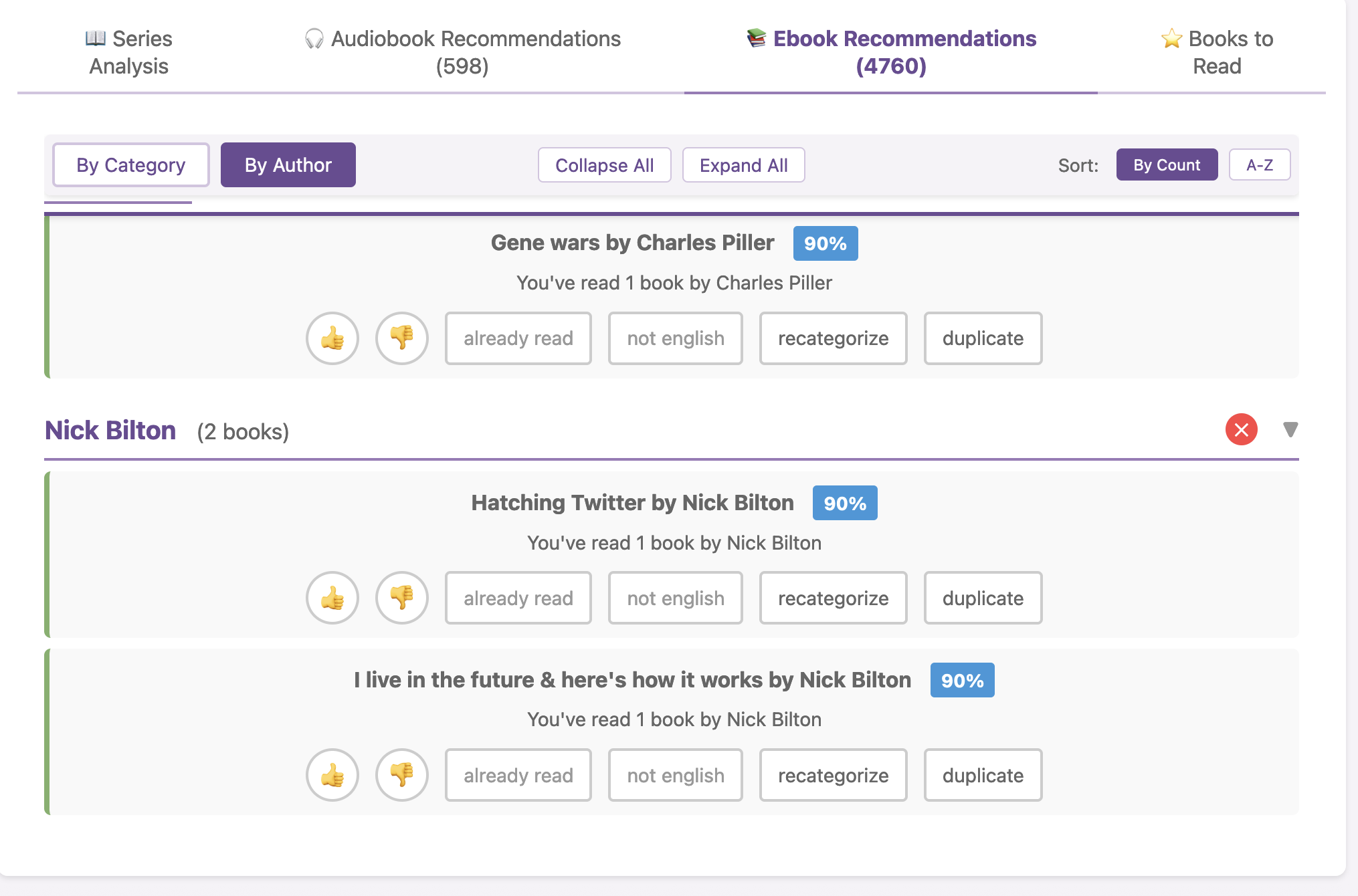
 I haven’t open-sourced BookPilot yet, but I can (
I haven’t open-sourced BookPilot yet, but I can ( I know some of the answers to the question of why clinicians aren’t doing this. But, the question I asked the Stanford AI+Health audience was to consider why we focus so much on informed consent for taking action, but we ignore the risks and negative outcomes that occur when not taking action.
I know some of the answers to the question of why clinicians aren’t doing this. But, the question I asked the Stanford AI+Health audience was to consider why we focus so much on informed consent for taking action, but we ignore the risks and negative outcomes that occur when not taking action.
 ScIG works for me (in a possibly very unique situation) better than IVIG does, and helps confirm that my disease is likely autoimmune related since it is responding to IG therapy, even though it’s still technically undiagnosed/doesn’t have a name (and no, isn’t one of the conditions that IG is usually used for). I am thrilled to finally be feeling somewhat better even though ScIG is not a cure but a partial bandaid (for me). A really expensive bandaid. But ScIG is a more flexible bandaid that I can do on my schedule and have control over and without having to hassle with other people’s schedules or the variety of administration approaches that comes from a rotating cast of infusion nurses at the ambulatory infusion center. And it’s cheaper than IV. But, we’ll see how long this is sustainable in terms of being able to manage the real estate that it requires to be subcutaneous. Keep your fingers crossed, please, that I can keep doing it as long as it’s working for me.
ScIG works for me (in a possibly very unique situation) better than IVIG does, and helps confirm that my disease is likely autoimmune related since it is responding to IG therapy, even though it’s still technically undiagnosed/doesn’t have a name (and no, isn’t one of the conditions that IG is usually used for). I am thrilled to finally be feeling somewhat better even though ScIG is not a cure but a partial bandaid (for me). A really expensive bandaid. But ScIG is a more flexible bandaid that I can do on my schedule and have control over and without having to hassle with other people’s schedules or the variety of administration approaches that comes from a rotating cast of infusion nurses at the ambulatory infusion center. And it’s cheaper than IV. But, we’ll see how long this is sustainable in terms of being able to manage the real estate that it requires to be subcutaneous. Keep your fingers crossed, please, that I can keep doing it as long as it’s working for me. Like using the Pro, having the Hypershell X Ultra makes it so I could do this full hike. It’s not a short hike: the full Rattlesnake Mountain hike is marked as 10.2 miles but from parking lot to parking lot it is closer to 10.9 miles and I tracked over 3,000 feet of elevation gain. I could do “just” the Rattlesnake Ledges hike (4.3 miles round trip, ~1100 feet of elevation gain), I could do the other side, but my muscles would be too fatigued to safely do a 10+ mile hike, so we wouldn’t even try it without an exoskeleton. And, there’s no way I would have considered doing it alone. Which…I did!
Like using the Pro, having the Hypershell X Ultra makes it so I could do this full hike. It’s not a short hike: the full Rattlesnake Mountain hike is marked as 10.2 miles but from parking lot to parking lot it is closer to 10.9 miles and I tracked over 3,000 feet of elevation gain. I could do “just” the Rattlesnake Ledges hike (4.3 miles round trip, ~1100 feet of elevation gain), I could do the other side, but my muscles would be too fatigued to safely do a 10+ mile hike, so we wouldn’t even try it without an exoskeleton. And, there’s no way I would have considered doing it alone. Which…I did!

 TL;DR: I love exoskeletons, they’re an instrument of freedom. I paid $1,200 in August 2025 for a Hypershell X Pro exoskeleton and love it (still love it). In late October/early November, I was given for free a Hypershell X Ultra exoskeleton after being selected for the Hypershell X Ultra Product Explorer program and have been using it and comparing it for the last several weeks. I love the opportunity and appreciate being chosen in the explorer challenge program so I could try it, and because it motivated me to head out on a big chicken-and-fox adventure up and over the full length of Rattlesnake Mountain, which I wouldn’t be able or willing to do without an exoskeleton to support my adventuring.
TL;DR: I love exoskeletons, they’re an instrument of freedom. I paid $1,200 in August 2025 for a Hypershell X Pro exoskeleton and love it (still love it). In late October/early November, I was given for free a Hypershell X Ultra exoskeleton after being selected for the Hypershell X Ultra Product Explorer program and have been using it and comparing it for the last several weeks. I love the opportunity and appreciate being chosen in the explorer challenge program so I could try it, and because it motivated me to head out on a big chicken-and-fox adventure up and over the full length of Rattlesnake Mountain, which I wouldn’t be able or willing to do without an exoskeleton to support my adventuring. In terms of getting set up and putting it on, it’s very straight forward. It gave me a starting suggestion to use for the waist size. I used that (and have never changed it), tightened up the waist strap and leg straps, and it was good to go from there. Once I got the waist strap tightened, I haven’t had to re-tighten or change that. I have had to tweak the leg straps a little bit here and there, partially because of how it slides around on my leg (see below re: sweating, chafing, and wearing in the summer as opposed to wearing it over a layer of clothing), but it’s quick and easy to tighten the leg strap or loosen it when needed and not a big deal adjustment wise. I did read a few people saying it slips down their hips and they got suspenders to help, but I haven’t had that experience (I’m female, so I have plenty of hip bone for it to rest against, and maybe that’s in part what makes the difference?). The first time I put it on, because I was adjusting straps, I put it on while sitting at the edge of a chair and getting everything set up and tightened, then stood up and tweaked the straps, then turned it on and began using it. Now, I can grab it and put on the waist belt while standing, then slightly lean over and attach each leg strap (so I don’t have to sit down to put it on). Because it carries the battery in the back and the design also has the support bar around the back, it’s not really comfortable to sit with for long if you want to lean back against the back of the chair, but it’s fine if you’re sitting down briefly on something (a chair, a bench, etc) if you’re not trying to lean back or sit up against the back of anything.
In terms of getting set up and putting it on, it’s very straight forward. It gave me a starting suggestion to use for the waist size. I used that (and have never changed it), tightened up the waist strap and leg straps, and it was good to go from there. Once I got the waist strap tightened, I haven’t had to re-tighten or change that. I have had to tweak the leg straps a little bit here and there, partially because of how it slides around on my leg (see below re: sweating, chafing, and wearing in the summer as opposed to wearing it over a layer of clothing), but it’s quick and easy to tighten the leg strap or loosen it when needed and not a big deal adjustment wise. I did read a few people saying it slips down their hips and they got suspenders to help, but I haven’t had that experience (I’m female, so I have plenty of hip bone for it to rest against, and maybe that’s in part what makes the difference?). The first time I put it on, because I was adjusting straps, I put it on while sitting at the edge of a chair and getting everything set up and tightened, then stood up and tweaked the straps, then turned it on and began using it. Now, I can grab it and put on the waist belt while standing, then slightly lean over and attach each leg strap (so I don’t have to sit down to put it on). Because it carries the battery in the back and the design also has the support bar around the back, it’s not really comfortable to sit with for long if you want to lean back against the back of the chair, but it’s fine if you’re sitting down briefly on something (a chair, a bench, etc) if you’re not trying to lean back or sit up against the back of anything.
Recent Comments