Like our previous RWJF-funded project, “Opening Pathways”, where we took time to reflect at the end of the project and also openly shared our grant-end narrative report that we submit to RWJF, John Harlow and I wanted to also share the grant-end narrative report that we created for RWJF for the Convening The Center project. The questions are based on their template. If you have any other questions about the Convening The Center project (background about it here), please do ask!
—
- What was the goal of your project? Do you have measures of your performance?
Our original goal was to convene THE center of healthcare, which means patients and caregivers and those working to effect change in the healthcare system from the ‘outside’. We originally planned for an all-expenses paid in-person physical meeting, gathering people from within the U.S. at a central location that would be relatively easy (within 2-3 hours of flying) to travel to for most individual participants. We aimed to gather 25 participants.
However, we were awarded our grant in December 2019 and saw the impact of COVID-19 early on in our communities (especially PI Lewis’s community of Seattle, where COVID-19 was first detected in the US in late January/early February 2020), and knew we would need to postpone the physical meeting from 2020 to at least spring 2021 at the earliest. As months passed, we realized the pandemic would not in fact be ‘over’, and debated between cancelling the grant or converting to a digital experience. We did not want to lose the opportunity to gather this type of community, and chose to switch to a digital meeting.
We spent significant amounts of time considering how to achieve the goals of our meeting (bringing together 25 people who didn’t necessarily know each other or have shared goals, beyond a broad overarching goal of improving healthcare, and giving them space to connect without forcing an agenda upon them). We ultimately decided to make our digital meeting a three-phase “experience:”
- The first phase would involve one-to-one conversations that would allow us to deeply listen and understand the perspectives of each participant. We would use a visual notetaker to illustrate their story and work as a way to reflect back what we heard, as well as offer the artwork as a gift to participants as a thank you for sharing their experiences with us. These conversations would then shape the following phases.
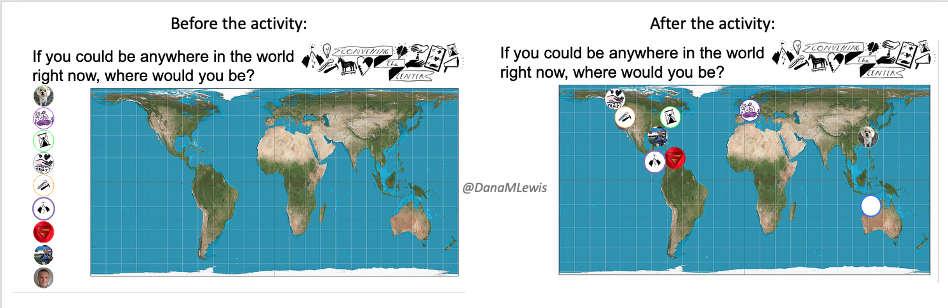
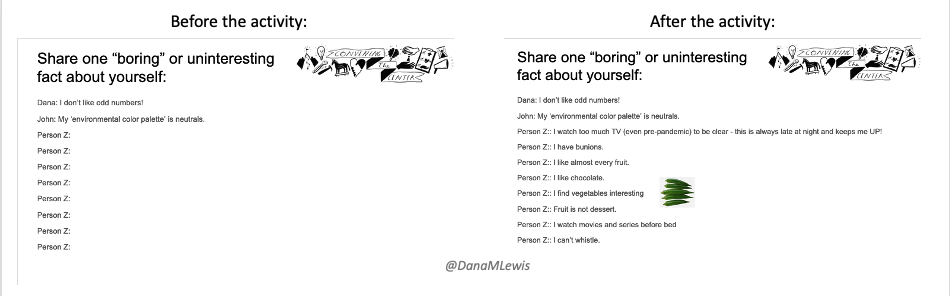
- The second phase was small-group conversations of up to 8 people maximum, which we chose based on a combination of availability and ensuring a mixed group of participants where there wasn’t necessarily one person or personality that would dominate a group conversation. There was no agenda, but we used Google Slides with some introductory activities to help people introduce themselves or their work in a non-threatening way, and facilitated topics of conversation for the group to dive into. We had four total groups in phase 2. We again had visual notetaking to represent each group’s conversation.
- The third phase was a single meeting with all 25 participants present. We chose a mix of small group breakouts, based on thematic topics that were discussed in phase 2 and voted upon by participants; as well as providing a small group mix based on people they had not yet met in previous groupings; and also small groups based on affinity groups that the PI/Co-PI selected based on what we learned of people’s work in phase 1-2. After the rounds of breakouts, the group returned together for a discussion with all 25 participants based on whatever topic they wished to discuss.
And, at the end of the project we had $9,000 USD remaining as a result of the pivot to a digital meeting. We decided to select nine individuals (through additional public recruitment) for “internet scholarships”, to continue to address the needs of this community. We successfully selected 9 recipients who each accepted the scholarship.
The project overall was a success.
- We were able to convene 25 participants from around the world and allow them to discuss whatever topics were most important to them.
- Because we went digital/virtual, we were able to facilitate participation from non-US based participants which greatly enriched the discussions.
- Participants consistently communicated surprise and delight after each phase of the project regarding how well they felt listened to, respected, and treated during the experience.
- We used a visual notetaker as a subcontractor, and her work was a critical factor of our success. Rebeka Ryvola is an experienced conference visual notetaker and artist, and although she had not previously worked in healthcare, her ability to listen to a deeply technical healthcare conversation and reflect high level themes from individual stories as well as across a diverse group of participants is unparalleled. Her art as an artifact of each discussion was critical for allowing participants to feel heard and respected, as well as providing a way to introduce themselves to each other within the cohort.
- Rebeka’s art for the individuals in phase 1 as well as the Phase 2 and Phase 3 pieces of art is already being widely shared and touted.
- All 9 selected recipients of the internet scholarships accepted them.
- Do you have any stories that capture the impact of this project?
One of our goals was to pay people for their time. Patients and caregivers are seldom paid for their time and expertise, although they offer invaluable expertise and solutions for improving healthcare.One individual, a parent with their own health situation as well as a parent of children with their own health situations, had served on a hospital advisory committee and numerous projects. However, until Convening The Center, this individual had never been paid for their time or work. They mentioned this numerous times throughout the project, almost in disbelief, that they were being paid for the first time for this type of time commitment. It was almost embarrassing to us for being the first people to pay them for their time on a project, although we are grateful for the resources of this grant that enabled us to pay each participant for their time.
In general, while we as PI/Co-PI know the power of bringing people together through social media and virtually, and we expected many of the participants (by virtue of finding this project) were already connected to numerous patient communities or organizations, we were surprised by the number of comments that participants made about the power of this convening. Two quotes stuck out to us, from an experienced patient advocate and from a newer patient advocate:
- “Getting to meet you all, truly made me feel not alone in what often feels overwhelming and hard.”
- [It was powerful] “bringing so many people from all corners together. I’m still building my confidence as a speaker and these opportunities to connect in a Round Robin sort of way was impactful, for someone who is still finding their voice as an advocate”(See Appendix at end for additional stories!)
- Did RWJF assist or hinder your project in any way?
RWJF assisted immensely by allowing us to submit a re-budget request and allowing us to shift to a virtual meeting while maintaining the existing level of budget. This was significant, because had we originally submitted a proposal for a virtual meeting, I think the grant would have been rejected/not awarded. Or, it may have been awarded with a significantly lower budget amount.
However, keeping the level of budget allowed us to spend significant amounts of time designing an inclusive, immersive digital experience that allowed us to bridge the participants’ physical worlds with our virtual meeting. We were able to do this by designing a “kit” to send to each participant, including international participants, with thoughtfully designed and curated items to aid them in their participation in this project. A typical virtual meeting would not have supported the budget for this type of ‘kit’ nor the PI/Co-PI’s increased time to design a thoughtful, effective, inclusive virtual meeting.
It also allowed us to facilitate the inclusion of participants from around the world. With a physical meeting, we were limited in budget to only US participants because of the travel cost variance with international travel. We were able to include participants from Costa Rica, Sweden, India, Pakistan, as well as across the US. We were also able to reach more diverse, under-resourced (including under-funded and under-included), and often minority perspective community members who maybe would not have been able to participate without it being virtual – even with us paying for their time and travel, because of their other family or community commitments.
Finally, because we went to a virtual experience and chose to do three ‘phases’ to build up to the final meeting, rather than a one-day in person meeting, we were able to get to know each participant and build trust over the phases that would not have happened by dropping 25 people into a room together for a physical meeting.
As a result, the permission and support with the same budget to shift to a virtual meeting greatly enriched the experience beyond what we would have originally predicted, and we hope RWJF considers this moving forward when thinking about facilitating similar gatherings of communities or projects.
Specifically within RWJF, our project manager Paul Tarini was helpful as always throughout the project. When we chose to pivot to a virtual meeting, we asked him for his perspective on thoughtful digital gatherings, and he shared not only his own experiences but also introduced us to a number of other RWJF grantees or collaborators to help us research best practices for online engagement for conferences and meetings. Many of the ideas we learned from collaborators such as New Public ended up shaping the phases of our work.
- If the project encountered internal or external challenges, how did they affect the project and how did you address them? Was there something RWJF could have done to assist you?
Our main challenges were the COVID-19 pandemic and the timing overall for our grant, because the primary goal was hosting a physical in-person meeting, Per the above section, RWJF assisted us by allowing us to re-budget from a physical in-person meeting to a digital gathering, while permitting the same overall level of budget. This was crucial for our success, because simply hosting a one-time 25 person meeting would not have achieved the goal without the additional design work that was done.
- Has your organization received funding from other foundations, corporations or government bodies for the project RWJF has been supporting?
No.
- When considering the design and implementation of this project, what lessons did you learn that might help other grantees implement similar work in this field?
We learned quite a lot regarding designing digital experiences that we hope other grantees will be able to leverage, and we hope RWJF will take this feedback into consideration and support other future projects that host virtual convenings.
For example, we learned that it takes more time to design impactful virtual gatherings that are not ‘just another zoom’. It takes design of the meeting itself with a clear ‘run of show’ or agenda, as well as clear pre-communication to participants about what to expect and how the meeting or gathering will go. In some cases, such as for our project, we also found it necessary to break the gathering up into multiple stages, to allow us to get to know participants and build trust to have the open, thoughtful discussions that emerged in phase 2 and 3. Had we simply plopped 25 people together in a virtual meeting as a one-off, it would not have been successful. We also were cognizant of the demand on participants in terms of overall time commitment – people don’t have the stamina for more than 2 hours on a video call – and the demands on internet bandwidth and personal energy for requesting a video call for that time period. We chose max 2 hours for each phase, and encouraged people to choose for themselves whether they had video on or off. We also designed activities to facilitate trust and comfort in the digital environment.
As a result, we learned that going from individual conversations to small group to larger conversations worked well for establishing safe spaces for open conversations. This also enabled relationships to begin growing throughout the project and not only after the ‘main event’ of phase 3. This facilitated the network within the cohort that began to grow as a community. You can’t force a community by dumping people in a place, but you can create a space and facilitate interactions that lead to relationship and network growth, and ultimately a community did evolve.
We also ended up developing a physical ‘kit’ to send to participants. It included a variety of useful items (such as a device cleaning cloth and a device stand, since many people are spending increased amounts of time on devices during the pandemic as well as we were asking them to spend more time on devices for this project). We also custom designed a few special items to honor people’s participation in the project. One of these items was a pack of playing cards that they could give to family or the people supporting them to help them be able to make the space for participating in the project. We also created a custom CTC keychain and provided several additional keychains that each participant could gift to others to honor other advocates, clinicians, and “doers” in the healthcare space who have helped them in their journey or that they want to honor their work. We hoped these keychains would also serve as a memento of their time in the project and be something they could physically hold in the future to give them strength, if they need it. This kit also included a whiteboard and markers, which we used in a variety of ways throughout the project including holding up to show something on screen, which we aimed to tie the offline/online experiences together. We didn’t want to send people “junk” “swag” that would end up in a landfill, and so we included things that we thought would be used by everyone in the cohort and had meaningful ties to the project.
Overall, one of our key design principles was to consistently signal that our gathering was and would be different from random meetings and conferences where people show up, say the same thing, and leave unchanged. We aimed to achieve this by doing everything different, from paying participants, to surprising people with their CTC ‘kit’, and to providing the visual note art as a gift after phase 1 in addition to doing visual notetaking from phase 2 and phase 3 as well. We consistently heard surprise and delight from participants beyond what you would typically receive from participants at a meeting or a conference, so we believe all of these elements of doing a gathering differently were successful, and that “surprise and delight” is an effective design principle for building relationships, creating spaces, and encouraging participation.
- What impact do you think the project has had to date?
The project was impactful in and of itself by successfully gathering 25 diverse individuals who have not previously had the opportunity to gather without an agenda forced upon them. Additionally, we were successful by paying each and every participant for their time. (Several individuals had never been paid before for their contributions to meetings, conferences, advisory committees, and/or research projects.)
In addition, it was successful for creating connections to enable network development and growth of relationships for people who don’t have traditional ‘professional development resources’ but benefit greatly from seeing other people ‘like them’ who are working to improve healthcare from the outside.
Through this project, people were able to surface similar challenges and experiences among individuals who felt isolated and ‘lonely’ in their work. They also were able to recognize shared challenges and solutions across disease areas, when they previously were not aware of resources. One example is a participant who shared research advocate training program materials from a specific cancer community, with other participants planning to leverage or mirror those resources in other disease spaces.
Additionally, participants began recognizing similarities across disease communities, with consistent gaps around areas such as transitioning out of pediatric to (young) adult care; lack of inclusivity with established advocacy organizations and online communities; and challenges with interacting with healthcare providers.
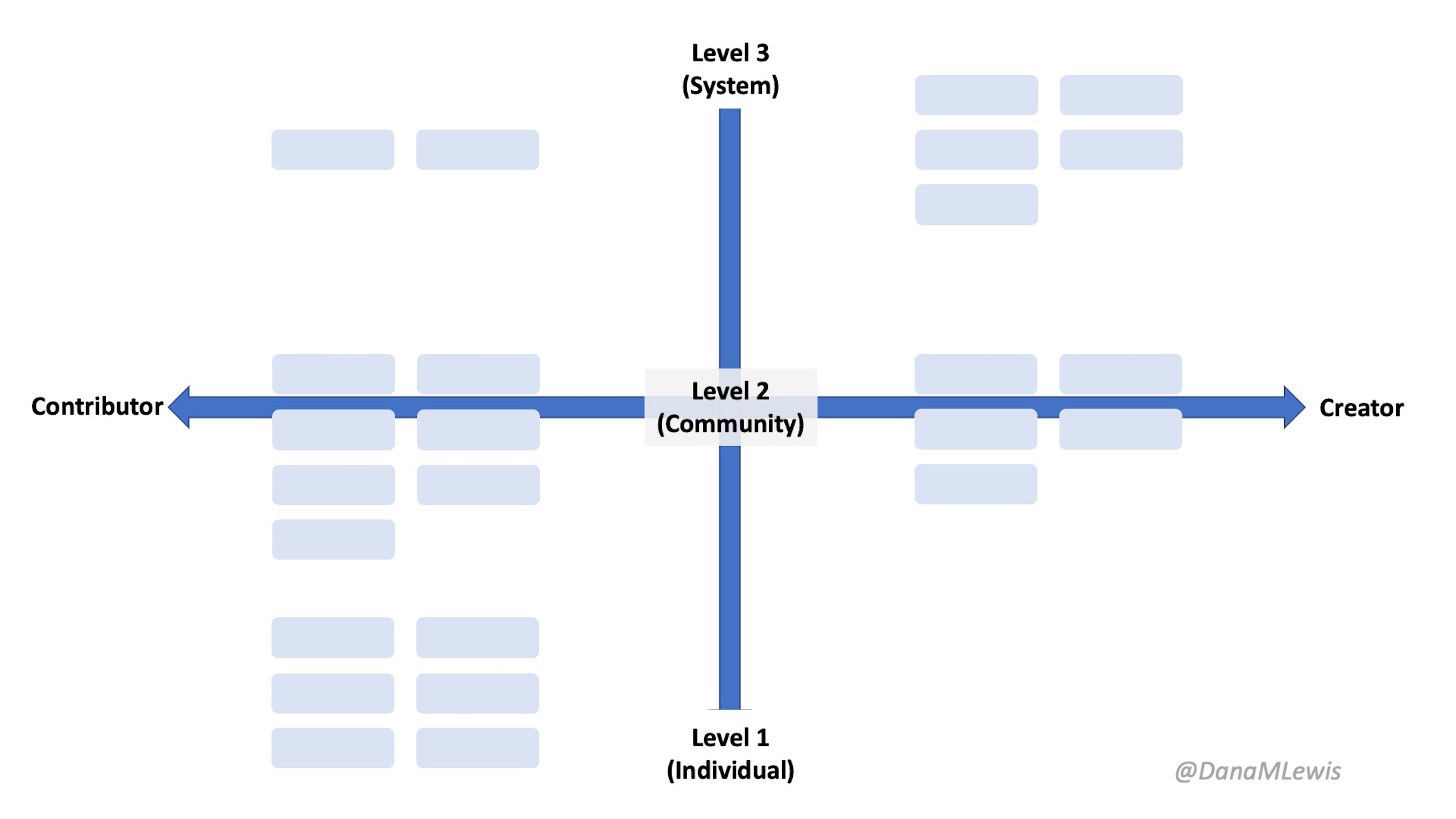
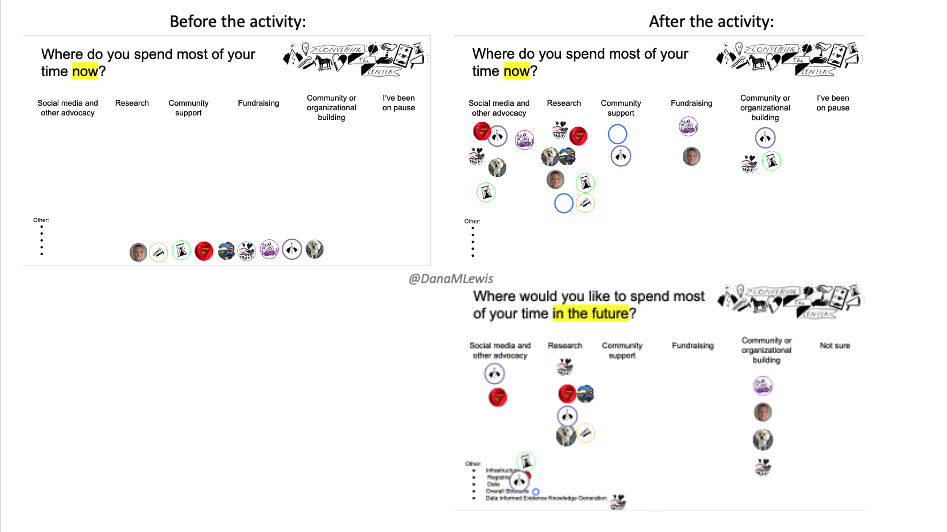
As PI/Co-PI we have also developed a novel framework for mapping the efforts of individuals by convening the center of health and healthcare. This is an innovative framework that assesses a spectrum of patient experiences based on what patients do when they go beyond navigating their personal or individual level of lived healthcare experiences and transition toward community or systemic level involvement. We have written up this framework and the results of thematic discussions from CTC in a research article, which we plan to submit to a peer-reviewed publication (and then share here soon!). We hope to inspire further work with this proposed model for facilitating improved matching between individuals and their current or future levels of interest and involvement with researchers, advocacy organizations, and other opportunities.
- What are post-grant plans for the project, if it does not conclude with the grant?
No specific plans, as the project technically concludes with the end of the grant.
However, many individuals who participated in this project are planning to work together in the future. For example, several post-meeting meetings have already happened among small groups within the cohort. One such meeting involved a discussion around patient-led research publications and strategy for utilizing blog posts and mainstream media compared to academic journals and traditional research conferences as methods of dissemination of patient community knowledge.
- With a perspective on the entire project, what were its most effective communications and advocacy approaches, its key publications, and its national/regional communications activities?
Our most effective communication was through social media. We publicized the project via a blog post shared across Facebook, Twitter, and LinkedIn. It was successful as measured by receiving applications from >60% of individuals that the PI did not recognize the name. From within the selected cohort, there were ~75% unknown participants to the PI/Co-PI, which indicated success in outreach to new networks and communities.
We believe the most effective advocacy approach was empowering individual participants. This project was not about name recognition of the project itself, but we believe by surprising and delighting participants and giving them a positive experience in the project, the ripple effects of this project and RWJF’s funding will continue to be felt for years to come.
APPENDIX:
We shared a draft version of this report with participants of the Convening The Center Cohort, asking for any additional feedback and stories we should include. The following stories and comments were shared as a result:
- “I appreciate how you have effectively captured the essence of our Convening The Center experiences. Surprise and delight are positive reinforcements and pragmatic concepts that can catalyze trust leading to trustworthiness; and overall the gatherings were very beneficial in developing a community of individuals who had similar interests with advancing patient and caregiver engagement. I do believe we were each pleased with the concrete extras including; fair compensation, bio-‘art’ifacts, CTC shareable reminders and reflected stories that we each will carry forward. The three tiered model was an effective method allowing for Conveners to listen and learn from each other.”
- “I think you captured the essence of my personal experience (I can’t/won’t/shouldn’t speak to the experiences of the others). The only thing I have to say is a hearty thank you to RWJF for allowing this project to proceed virtually. It was an enriching experience, filled with far more diversity (as you pointed out).”
- “Many thanks to CTC & grantor RWJF for allowing the power of the pivot to take place!
Do you have any stories that capture the impact of this project?
I would add that this experience presented an opportunity to amplify voices of women of color. This group was accepting of my perspective and participating in it further ignited my passion to embrace my efforts as an advocate for an underserved patient population.
What impact do you think the project has had to date?
The project inspired me to challenge old ideas of self-doubt and redefine what advocacy means to me. Since the convening, I’ve been empowered to participate in projects that bring forth HPV, Cervical, & Gynecologic Cancer awareness for the Black-Hispanic population. This was a huge moment of growth and development for someone who struggles with social anxiety.
When considering the design and implementation of this project, what lessons did you learn that might help other grantees implement similar work in this field
I just wished to add, if others would like to duplicate a similar idea in a virtual capacity, it is important to have systems in place that allow for free flowing communication. This was my first time using Slack and it performed well in my opinion. The platform could be accessed on both pc or mobile device.
I always felt connected & well-informed. The [Slack] app made it easy to contribute to the discussion with the group throughout the entire project. It also presented the opportunity for members to learn more about one another through introductions and our artwork; all prior to meeting each other virtually.”
A huge thank you to each participant who was a part of Convening The Center!

Recent Comments