My name is Dana Lewis and I have a closed loop artificial pancreas (that I built) that I use every night. Also see: woot!

We closed the loop in December (click here for more details about the first week of data & basics on how the closed loop works; or here to learn more about the basic non-closed loop #DIYPS and how far we’ve come in a single year), and I’ve been using it almost nonstop since.
I’ve only been limited in using the closed loop for overnight when I inadvertently fried the SD card in the Raspberry Pi (a known issue that’s related to the number of times you plug/unplug it from power source). We promptly ordered a second Pi as a backup, and by the time it arrived, Scott managed to revive the first one, so I now have two ready to run at any time. (Because of course you need emergency backups of your essential organs!)
When I first started looping in December, I originally intended to only use it at night, but it was hard to not loop during the day, too. The idea that I could sit at my desk and work for 3-4 hours straight, and not worry about my BGs, is so appealing!
However, it’s not really practical for me to want to use 24/7 every day…yet. This is where the versions of APS that will come to market in 3+ years will be great, because it will be all-in-one (or at least limited in excess pieces you have to carry). To wear it 24/7, I have to have enough batteries to power the raspberry pi and keep it in range, which means constantly picking it up and moving it around, carrying it in my bag from meeting to meeting, etc. I’ve decided it’s not worth it for every day, but it is awesome to have the choice when sitting through an important interview to have it running and have more security and peace of mind.
Back to using the closed loop for overnights
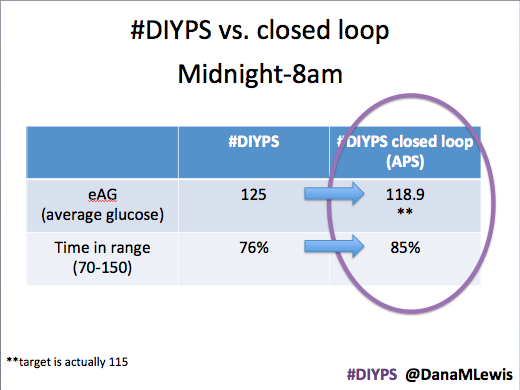
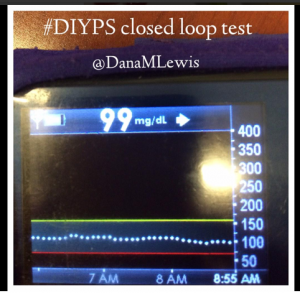
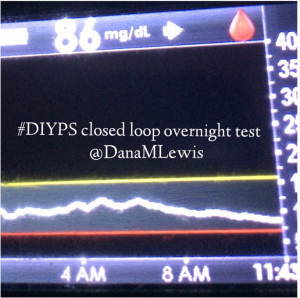
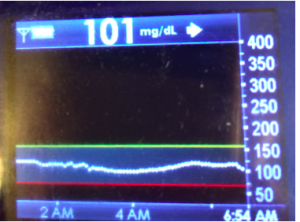
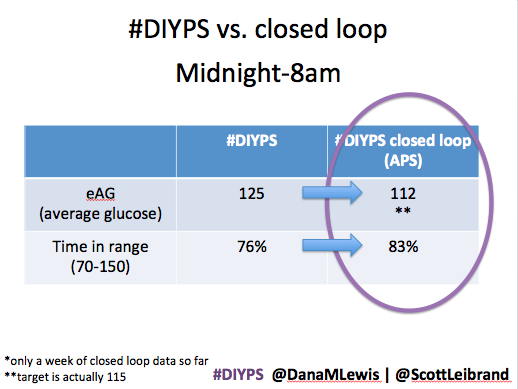
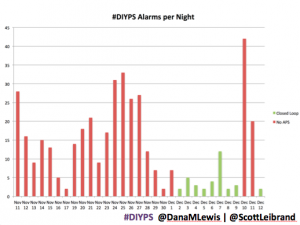
When we first showed our closed loop efforts off, we had about a week’s worth of data that already showed improved overnight blood glucose (eAG) and time in range, plus reduced number of #DIYPS alarms.
After a month, the results of using a DIY closed loop artificial pancreas system overnight continue to look promising:
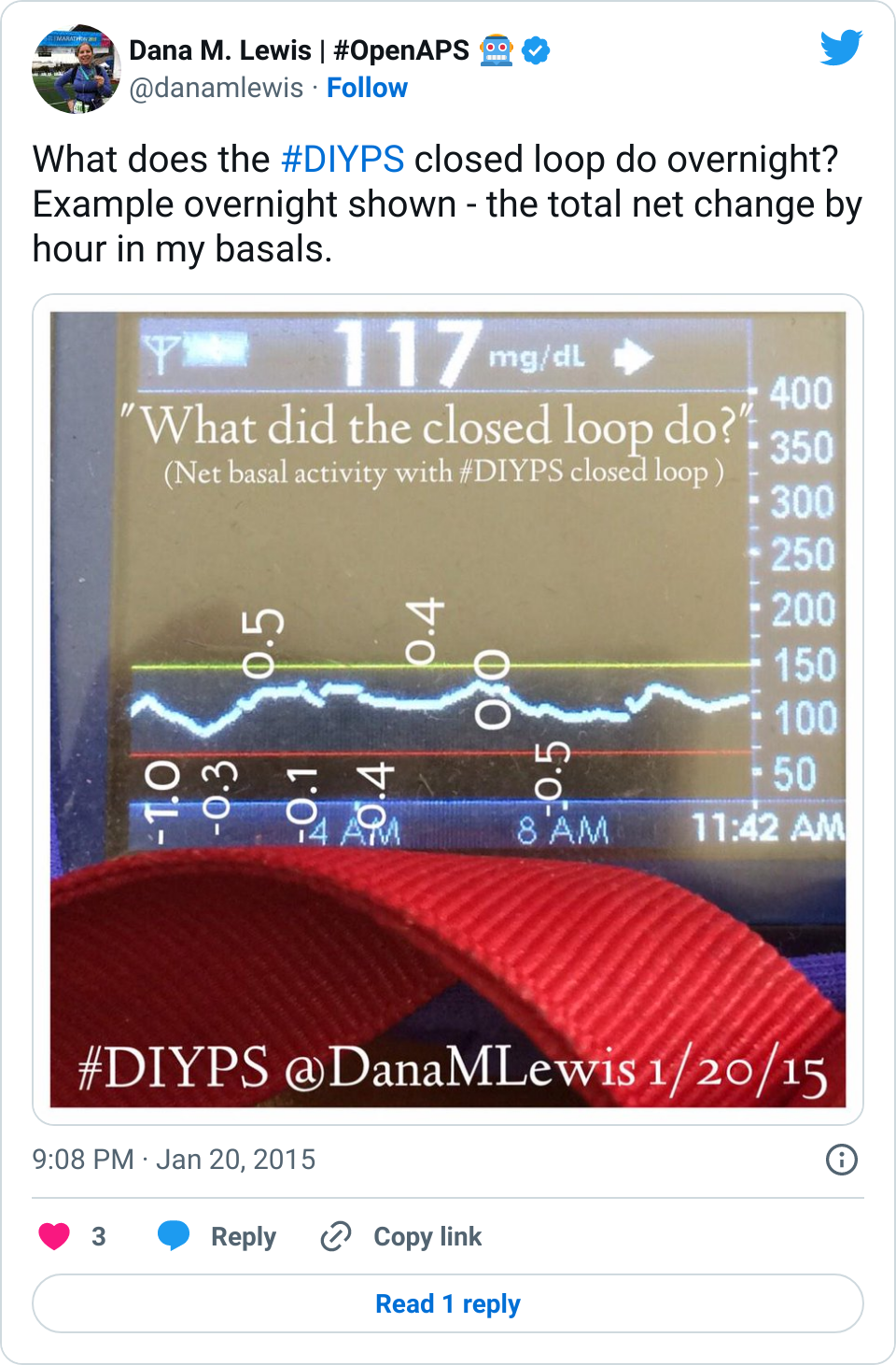
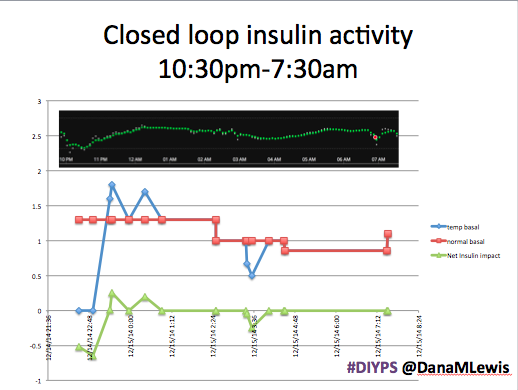
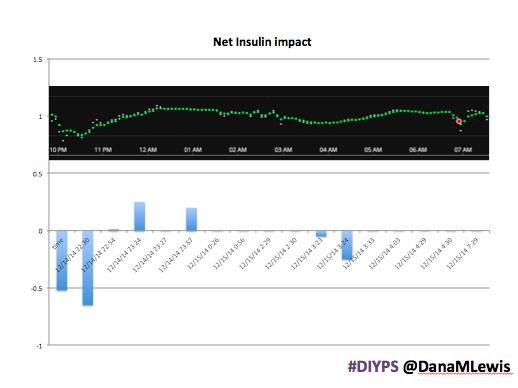
We also recently added another screen to #DIYPS so I could access and review “what happened last night”, or what was the output of the closed loop. I usually look at the net impact per hour (how much above or below my normal basal rates I ended up getting), but also at the individual numbers of how much above and how much below I ended up getting every hour. Here’s a visualization:
Using closed loop activity to spot trends and change basal rates
We also built a 7 day and 30 day view of this closed loop activity history so I can look at trends by hour overnight (versus manually compiling and visualizing them, like I did in our first closed loop data post here).
When we first looked at the data for overnight closed loop net insulin activity, I could spot a trend easily – the loop temped low from midnight to 2am, leveled out, then increased with higher temps after 5am. I can easily see why it often ends up temping low after I go to sleep, because I often do a half unit or so if I’m riding “high” (130 – ha!), and feel safe doing so with the loop to catch any more drop than I desire. (This pattern was consistent at 7, 14, and 30 days, although the average net insulin amount varied slightly.)
However, when I first started looping overnight in December, I had rises around 2am that the loop had to handle by providing higher temporary basal rates than my scheduled basals. I upped my midnight basal rate as a result, but it looks like I upped it too far since the closed loop often temps low now during that time frame. My next step is to probably change my midnight basal to be lower by 0.1u, and see if that reduces the amount of low temps needed from 12-2am, without causing spikes. My theory is that this alone may also reduce the number of higher temps from 2-4am, because those may be a result of the lower temps earlier on. Thus, I am starting overnight basal tweaking with this one change and seeing how much of a ripple effect it has for the rest of the night as well.
In pursuit of…what? Or: what are we optimizing for?
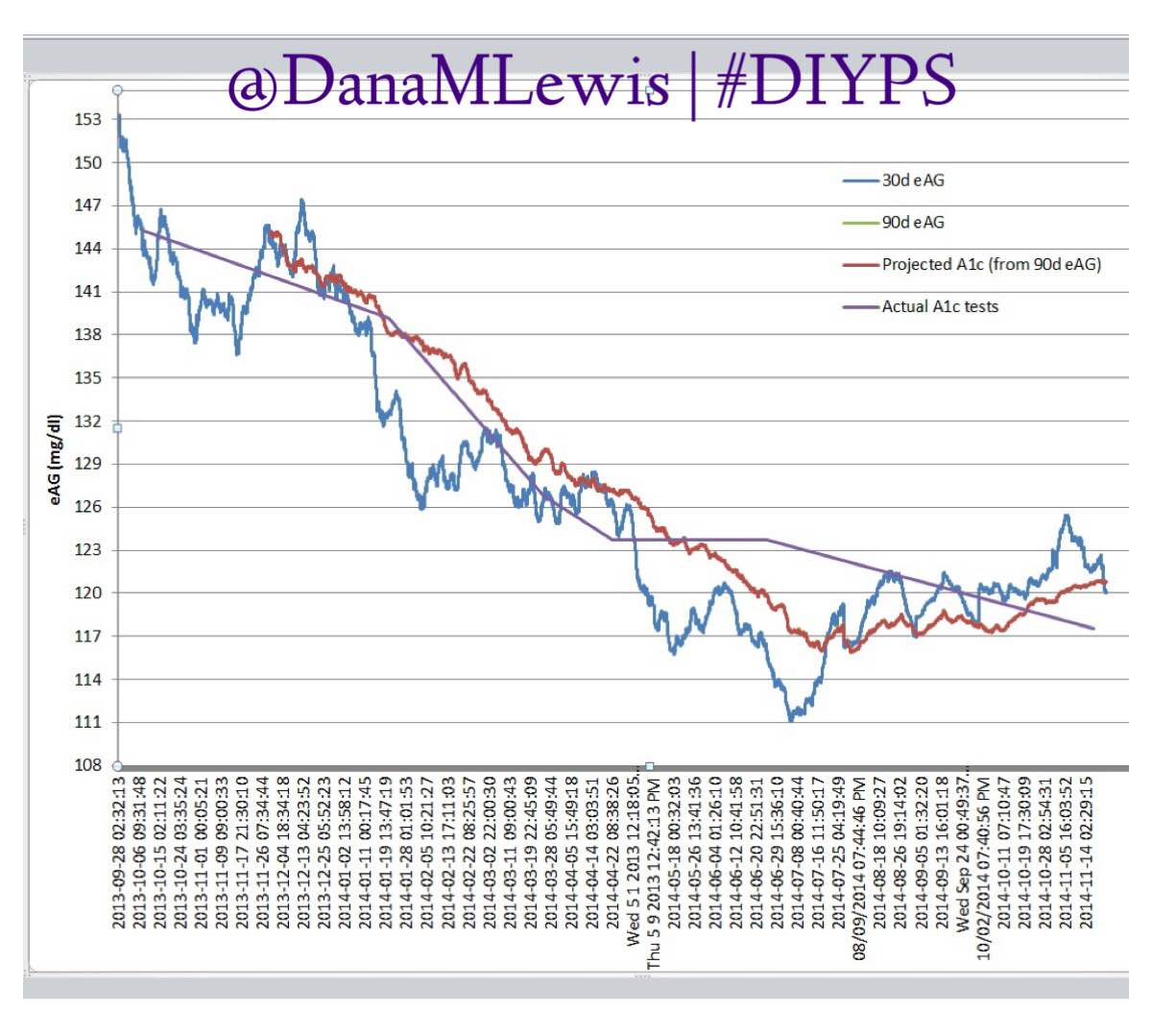
My BG averages overnight (and during the day) are excellent (well within the “normal” range <120) and time in range is continuing to grow (85% & counting) with using the closed loop #DIYPS. So, beyond minute basal tweaking, what’s next?
At this point, I think the next goal is encouraging other independent researchers to get up and running on their own closed loop overnight APS. Do we really need to wait another 3+ years for APS technology to come to market? What exactly would #WeAreNotWaiting look like if we applied it to closed loop Artificial Pancreas technology research? What do you think?



Recent Comments